
Abstract
The tubeless percutaneous nephrolithotomy (PCNL) is highly favored by endourological urologists for its advantages in patient experience and length of hospital stay. However, there is currently no guideline or consensus that precisely describes tubeless PCNL. This study explores tubeless PCNL from two aspects: patient selection and technical improvements. Clinical data of 40 cases of conventional PCNL and tubeless PCNL patients operated by the same surgeon between December 2023 and April 2024 were analyzed. The changes in the preoperative and postoperative renal function, hemoglobin and inflammatory markers were evaluated, and the operative time, pain scores, and length of hospital stay were also included. Both groups of patients achieved complete stone clearance (100%). Compared to the conventional PCNL group, the tubeless PCNL group had lower pain scores (P < 0.001) and shorter hospital stays (P = 0.005). There were no statistically significant differences between the two groups in terms of operative time (P = 0.83), renal functional impact (P = 0.699), hemoglobin reduction (P = 0.93), and changes in inflammatory markers (P > 0.05). Tubeless PCNL demonstrated better patient experience and shorter hospital stays. Tubeless PCNL patients were strictly selected according to our criteria and operated based on traditional experience and the improved technical standards in this study. Tubeless PCNL is safe and feasible under these conditions. Retrospectively registered: 0620, August, 2024.
Similar content being viewed by others


Introduction
Percutaneous nephrolithotomy (PCNL) is a key milestone in developing endoscopic urology. Compared to traditional open stone surgery, PCNL offers advantages such as minimal trauma, reduced bleeding, rapid recovery, and high stone-free rates1,2. PCNL removes stones by creating percutaneous renal access, followed by the placement of a nephrostomy tube and a ureteral stent postoperatively. To ensure a high stone-free rate, the early access is often large in diameter (> 26F), leading to a higher rate of complications and increased patient discomfort3. In this context, the concepts of miniaturized access and tubeless PCNL have been introduced. However, two cases of severe extravasation in tubeless PCNL have sparked controversy over this technique4.
With the accumulation of experience and advances in technology, tubeless PCNL is increasingly being accepted and attempted by more urological surgeons. Despite the risks with tubeless PCNL, its excellent performance in terms of reducing hospital stay, alleviating patient pain, and promoting quick recovery makes it a hot topic among endourological surgeons5. Previous experiences have shown that strict patient selection is essential to minimize complications associated with tubeless PCNL6. However, there are currently no definitive guidelines or consensus on tubeless PCNL in clinical practice.
This study combines insights from previous studies and clinical practice to summarize the criteria for patient selection in tubeless PCNL. Additionally, we summarize several key technical improvements implemented at our institution, aiming to promote the widespread adoption of tubeless PCNL and enhance the treatment experience for patients.
Methods
Statements, case selection and patient information
This retrospective study was approved by the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology, affiliated Union Hospital. All research was performed in accordance with relevant guidelines/regulations, and we confirmed that informed consent was obtained from all participants and/or their legal guardians. All research had been performed in accordance with the Declaration of Helsinki.
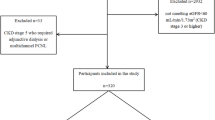
Patients are divided into the tubeless percutaneous nephrolithotomy (PCNL) group and the conventional PCNL group according to whether or not a nephrostomy tube was ultimately placed. All 40 patients, who underwent surgery by the same surgeon in the Department of Urology at Wuhan Union Hospital from December 2023 to April 2024, were included. During this period, 20 patients underwent tubeless PCNL, while the remaining 20 patients underwent conventional PCNL on the same day or week as the tubeless PCNL cases. We analyzed the clinical data of these patients, including general patient information, complete blood count, blood biochemistry, urine culture, kidney-ureter-bladder (KUB) X-ray, renal computer tomography (CT), renal ultrasound results and so on.
Surgical procedure
After anesthesia and preparation of the kidney, the patient was placed in the prone position. A Chinese one-shot dilation technique7was employed under color Doppler guidance8 to establish a working channel (typically 20F/22F), with successful establishment indicated by the ability to aspirate urine. Following channel establishment, a 10.5Fr ureterorenoscope (KARL STORZ) was introduced, and a Holmium:YAG laser (by Lumenis) was used for lithotripsy. Upon completion, residual calculi were detected using Hitachi color Doppler ultrasound. If no residual fragments or very few and small fragments (diameter < 4 mm), and no calculus likely to cause obstruction were detected, lithotripsy was finished. Subsequently, a 5F double J stent was placed, followed by a decision regarding whether to place an 18F/20F nephrostomy tube. On the first postoperative day, the urethral catheter was removed, and the nephrostomy tube was clamped. If there was no fever or urinary leakage, the nephrostomy tube was removed 12 to 24 h after clamping.
Anesthesia method
The majority of patients underwent general anesthesia for the surgery, while some patients received regional anesthesia9. The specific procedure for regional anesthesia was as follows: patients did not undergo retrograde intubation or urinary catheterization. Half an hour before the surgery, patients received an intramuscular injection of 100 mg tramadol and 25 mg dexmedetomidine. Intraoperatively, a mixture of 1% lidocaine and 0.5% ropivacaine was administered via subcutaneous infiltration (approximately 10 mL) at the puncture site for regional anesthesia. During the surgery, dexmedetomidine (5 mg) was administered intravenously, and ondansetron was given prophylactically to prevent nausea and vomiting. The remaining technical procedures were no difference from the conventional method10.
Kidney preparation
All included patients underwent kidney preparation using stimulated diuresis technology11. Upon arrival in the operating room, patients were placed in the prone position and received an intravenous injection of normal saline (500 to 1000 mL), followed by furosemide (0.5 mg/kg) to facilitate diuresis. The dilation of the renal pelvis was measured using ultrasound, which typically reached peak values in 6–15 min11. Following this, kidney preparation was completed.
Color Doppler-guided puncture and intrarenal fold-line puncture technique
All included patients underwent puncture procedures guided by color Doppler imaging. Traditionally, the center of the renal pelvis had been considered the ideal avascular puncture point (Fig. 1A, Supplementary video 1). But vascular variations were common, the center of the renal pelvis did not always indicate an avascular area (Fig. 1B, Supplementary video 2). Therefore, individualized puncture pathways were designed based on color Doppler ultrasound. The vascular distribution of the target calyx was examined, by initially setting the color Doppler blood flow velocity at 15–17 cm/s. If vascular density was low or moderate, avascular areas are identified and selected as the puncture pathway (Supplementary video 3). In cases with abundant vessels in the calyx, the avascular areas were further investigated by resetting the blood flow velocity to 25–27 cm/s8. For a few patients with significant renal artery variations, finding an optimal straight puncture pathway was challenging. Therefore, an intrarenal fold-line puncture technique was utilized under color Doppler guidance. Under these conditions, the puncture needle entered the target calyx along a fold line to avoid blood vessels (Supplementary video 4, 5).

Blood flow under color Doppler imaging. (A). Normal blood flow of renal calyx. (B). Mutated blood vessels, spanning the renal cortex.
Chinese one-shot dilation technique for channel establishment
All enrolled patients underwent channel establishment using the Chinese one-shot dilation technique7. Initially, an 18 G Chiba needle was inserted into the collecting system under color Doppler guidance8. Successful puncture was confirmed by the ability to aspirate urine after removing the stylet. A super-rigid guidewire was then introduced, followed by the withdrawal of the puncture needle. Before removing the puncture needle, the fascia and skin at the puncture site were incised. Besides, while removing the puncture needle, the direction and depth were recorded. Subsequently, a 20F/22F pencil-shaped fascial dilator with a matching oblique sheath was inserted along the super-rigid guidewire (Fig. 2A). Rotational breakthrough was employed during the passage from the renal cortex into the collecting system. The pencil-shaped fascial dilator, with its slender and pointed tip, has been clinically proven to possess single-step dilation capability7. Upon successful aspiration of urine from the dilator, the dilator was removed, maintaining the position of the oblique sheath. Thus, the working channel was completed.

Appearance and application of oblique sheath. (A). Dilator with a matching oblique sheath. (B). Front view of oblique sheath. (C). Side view of oblique sheath. (D-F). No bleeding in the channel by using oblique sheath. (G-I). Counterclockwise rotation of the oblique sheath resulted in a transition from a clear to a blurred view. The arrow indicated the site of vascular injury.
Application of oblique sheath
Prior to establishing the channel, the sheaths were trimmed. The anterior end of the sheath was trimmed into an oblique opening (Fig. 2B,2C). This modification has demonstrated several advantages in application. First, it facilitated matching with the inner dilator. Second, it provided ease of dilation and entry into narrow calyces and ureters, thereby reducing mucosal injury and calyceal tear (Supplementary video 6, 7). Third, it enhanced visibility for locating and observing relatively parallel renal calyces (Supplementary video 8). Fourth, it allows for the retraction of the sheath to the renal capsule, rotation of the outer sheath to observe any bleeding in the channel, and reduction of the channel loss rate (Fig. 2D-I, Supplementary video 9, 10).
Case selection of tubeless PCNL
Based on preoperative evaluations and intraoperative performance, patients meeting the following criteria were prioritized for tubeless procedures:
-
a)
Preoperative hemoglobin level higher than 90 g/L and normal coagulation function.
-
b)
Low risk of sepsis preoperatively and intraoperatively.
-
c)
No renal upper calyx puncture.
-
d)
No significant residual stones.
-
e)
No significant bleeding in the channel.
Early clinical data indicate that postoperative hemoglobin decrease did not exceed 30 g/L under the strict principle of no bleeding in the channel12. Therefore, patients with preoperative hemoglobin greater than 90 g/L are at low risk of requiring postoperative blood transfusion.
Sepsis is one of the most common complications, with a high mortality rate ranging from 22 to 76%13. The risk of sepsis must be assessed on both preoperative and intraoperative performance: preoperatively, absence of fever, normal blood leukocyte counts, and normal procalcitonin levels; intraoperatively, clear urine, absence of pus and purulent deposits in the kidney, and absence of fibrinous material on the stone surface, indicate a lower risk of sepsis14,15,16.
Tubeless PCNL is not chosen for upper calyx punctures due to the relatively higher risk of pleural injury17,18. If pleural injury occurs and tubeless procedures are performed, respiratory efforts combined with urinary leakage can easily lead to pleural effusion and hemorrhage.
The residual condition of stones should undergo a comprehensive evaluation to avoid secondary surgeries: Preoperatively, confirm the stone locations based on imaging results; intraoperatively, identify the stones in the renal pelvis and calyces according to anatomical features and imaging results, and confirm whether the positions change with ultrasound; postoperatively, check for residual stones using ultrasound.
Ensuring there is no bleeding in the channel is important, since one of the functions of the nephrostomy tube is to drain potential blood and effusion. The presence of bleeding in the channel can be assessed by the oblique sheath: After lithotripsy, retract the anterior end of the oblique sheath to the renal capsule, then rotate the dilator, and observe the entire renal puncture channel for significant bleeding (under conditions of 150 mmHg pressure and 300 ml/min flow rate, clear visibility indicates no bleeding, Supplementary video 9, 10).
Statistical analysis
For all the patients of two groups, the following parameters were evaluated: 1. Stone clearance rate: Kidney-ureter-bladder (KUB) radiographs were routinely performed before removing the double J tube. No residual stones or residual stones < 4 mm were considered to be stone free; 2. Duration of surgery; 3. Pain level: Assessed by using the Visual Analog Scale (VAS) on the first postoperative day; 4. Postoperative hospital stay; 5. Postoperative change in hemoglobin (Hb) levels; 6. Postoperative change in serum creatinine (umol/L) and estimated glomerular filtration rate (eGFR, ml/min/1.73m2); 7. Postoperative changes in inflammatory markers, including neutrophil count, procalcitonin (PCT), and C-reactive protein (CRP).
Statistical analysis was conducted using SPSS 26.0.2 software19. Continuous data were presented as mean ± standard deviation. Student’s t-test was employed to analyze intergroup differences in the mean values. P < 0.05 was considered statistically significant.
Results
The patients included were from the Department of Urology at Wuhan Union Hospital. They underwent surgery during the period of December 2023-May 2024, performed by the same surgeon. During the time, 20 patients underwent tubeless PCNL. Cases for conventional PCNL were selected from patients who underwent surgery on the same day or within the same week as tubeless PCNL patients. Information for all 40 patients is presented in Table 1.
Both groups of patients achieved successful stone clearance, with one working channel established (Fig. 3A,3B). The tubeless PCNL group had a shorter hospital stay (P = 0.005). Additionally, the VAS scores were significantly lower in the tubeless PCNL group (P < 0.001). However, there was no significant difference in surgical duration between the two groups. Moreover, there were no significant differences in renal function and inflammatory responses (P > 0.05). None of the included patients developed fever postoperatively (Table 2).

Representative KUB radiography of a 40-year-old man who underwent tubeless PCNL. The patient had multiple left kidney stones with a maximum diameter of 14 mm and no hydronephrosis. (A). Preoperative. (B). Postoperative. The arrows showed the position of kidney calculus.
Discussion
The first report of PCNL was published in 197620. Since then, extensive clinical experience has accumulated. Based on institutional experience, clinical guidelines21, and expert opinions22, we believe that in the following clinical scenarios, PCNL is superior to ureteroscopy and flexible ureteroscopy: A. large stone burden (> 2 cm); b. prolonged stone impaction (more than six months) combined with suspected ureteral stricture; c. recent history of ipsilateral ureteroscopy with incomplete stone clearance, potential due to suspected ureteral stricture; d. severe hydronephrosis, thinning of the renal cortex or atrophic kidney, with poor renal function making stone clearance difficult; e. combination of ureteral stones with a large number of lower pole stones; f. lower pole stones with a ureter-lower calyx distance (ULD) of less than 2.5 cm23; g. intolerance to general anesthesia; h. CT evidence of significant renal swelling with perinephric exudative changes; i. gross hematuria indicating poor visualization during ureteroscopy; j. renal anatomical abnormalities (e.g., duplicated kidneys, horseshoe kidneys, etc.).
PCNL patients are routinely placed with internal and external drains, which are nephrostomy tubes and double J stents. The nephrostomy tube compresses the tract to achieve hemostasis, drains renal fluids to decrease intrarenal pressure, and prevents potential bloodstream infections24. Still, it preserves a pathway for the next operation if needed. The double J tube ensures patency of the renal-bladder pathway, preventing secondary ureteral strictures due to operative injury, stone impaction, or infection. However, nephrostomy tubes have several limitations. They increase patient discomfort, impose an economic burden, and raise the risk of urinary leakage and secondary infections5,24,25. Thus, tubeless PCNL has become a primary focus for endourologists. Our goal is to balance the pros and cons and select suitable patients for tubeless PCNL.
We select patients eligible for tubeless PCNL based on preoperative and intraoperative performance. A hemoglobin level above 90 g/L significantly reduces the need for postoperative transfusion. Normal coagulation function and absence of significant bleeding in the channel effectively prevent increases in intrarenal pressure, a potential adverse consequence of tubeless PCNL. Absence of fever, normal blood leukocyte counts, and preoperative procalcitonin (PCT) preoperatively, along with clear renal urine and absence of pus or debris on stone surfaces intraoperatively, reduce the risk of postoperative renal infection and greatly lower the probability of sepsis. Avoiding upper calyx puncture prevents pleural effusion, which is a potential complication of tubeless PCNL. The absence of obvious stone residue avoids the possibility of secondary surgery.
Furthermore, we incorporate new technologies to enhance the feasibility of tubeless PCNL for patients. Individualized path planning and fold-line puncture guided by color Doppler greatly avoid blood vessels, significantly reducing bleeding rate8. The Chinese one-shot dilation technique eliminates the need for repeated dilator changes, further lowering the bleeding rate7. Additionally, the use of oblique sheaths allows for a larger field of view within a smaller range of sheath movement, further reducing the risks associated with tubeless procedures.
Our research results also demonstrated the significant advantages of tubeless PCNL. Tubeless PCNL significantly shortened patients’ hospital stay, reduced postoperative pain, and had no significant impact on renal function (serum creatinine and eGFR). Based on the patient selection and technical improvements mentioned above, both groups exhibited similar postoperative hemoglobin decreases, with no cases requiring postoperative transfusion. Moreover, inflammatory markers including neutrophil count, PCT, CRP, showed no significant differences between the two groups, suggesting that, under strict indications, tubeless PCNL might not affect infectious probability. No patients developed fever postoperatively, including those with preoperative positive urine cultures. It suggested that preoperative positive urine cultures might not be an absolute exclusion criterion for tubeless PCNL, although this result was limited by the sample size and might not be definitive.
Tubeless PCNL is being explored by numerous urologists domestically and internationally. Zhang et al. pointed out that a renal cortex thickness (> 5 mm) at the site of channel favored tract contraction, reducing urine leakage, which can serve as a screening criterion for tubeless PCNL26. Mao and Jian et al. argue that patients with ureteropelvic junction obstruction (UPJO) or ipsilateral ureteral stricture are not suitable for tubeless PCNL, due to potential drainage obstruction and increased intrarenal pressure5,27. Furthermore, studies by Lei et al. suggest that patients with renal collecting system perforation are also not suitable for tubeless PCNL, as nephrostomy tubes will provide better drainage28. However, Jou et al. hold the opposite opinion29. Additionally, single puncture, single tract, no intraoperative bleeding, no extravasation, and no pus intraoperatively all tend to favor tubeless PCNL with experience. Although tubeless PCNL criteria may vary slightly among different institutions, all show lower pain scores, shorter operation and hospitalization times, reduced surgical costs, and comparable surgical outcomes when compared to conventional methods.
Conclusion
In conclusion, this study, along with various related studies, highlights the advantages of tubeless PCNL. Additionally, this study details several technical improvements implemented in our institution for both conventional and tubeless PCNL patients. These improvements standardize the inclusion and exclusion criteria for tubeless PCNL, enhancing patient safety while ensuring stone clearance rates. A limitation of the study is the small number of patients included in this study, which leaves some potential risks and complications remain unknown. Undoubtedly, a prospective study with randomization is needed, and we hope to apply these techniques to more eligible patients in future clinical work, further optimizing procedural details. Meanwhile, with advancing technology and accumulated experience, we are also exploring the possibility of a completely tubeless PCNL (without nephrostomy tubes or double J tubes), which will undoubtedly enhance patient experience in terms of both comfort and time.
Availability of data and materials
All data generated or analysed during this study are included in this published article and its supplementary information files.
References
de la Rosette, J. J. et al. Categorisation of complications and validation of the Clavien score for percutaneous nephrolithotomy. Eur. Urol. 62(2), 246–255 (2012).
Tang, R. et al. Percutaneous nephrolithotomy versus open surgery in the treatment of urinary calculi. Altern. Ther. Health Med. 30(12), 291–295 (2024).
Sahin, A. et al. Percutaneous nephrolithotomy in patients aged 60 years or older. J. Endourol. 15(5), 489–491 (2001).
Winfield, H. N., Weyman, P. & Clayman, R. V. Percutaneous nephrostolithotomy: complications of premature nephrostomy tube removal. J. Urol. 136(1), 77–79 (1986).
Mao, Y. et al. Case selection and implementation of tubeless percutaneous nephrolithotomy. Transl. Androl. Urol 10(8), 3415–3422 (2021).
Wang, J. et al. Risk factors for deterioration of renal function after percutaneous nephrolithotomy in solitary kidney patients with staghorn calculi. Transl. Androl. Urol. 9(5), 2022–2030 (2020).
Xiong, J., Shi, Y., Zhang, X., Xing, Y. & Li, W. Chinese one-shot dilation versus sequential fascial dilation for percutaneous nephrolithotomy: A feasibility study and comparison. Urol. J. 16(1), 21–26 (2019).
Shi, Y., Yang, X., Mathis, B. J. & Li, W. Can color doppler ultrasound challenge the paradigm in percutaneous nephrolithotomy?. J. Endourol. 36(3), 373–380 (2022).
Shahait, M., Farkouh, A., Mucksavage, P., Proietti, S. & Somani, B. Outcomes of percutaneous nephrolithotomy under local anesthesia: Outcomes of a systematic review of literature. J. Endourol. 37(8), 855–862 (2023).
Tailly, T. & Denstedt, J. Innovations in percutaneous nephrolithotomy. Int. J. Surg. (London, England) 36(Pt D), 665–672 (2016).
Shi, Y. et al. Ultrasonography-guided percutaneous nephrolithotomy with Chinese one-shot tract dilation technique based on stimulated diuresis: A report of 67 cases. J. Huazhong Univ. Sci. Technol Med. Sci.= Huazhong keji daxue xuebao Yixue Yingdewen ban 36(6), 881–886 (2016).
Ding, M. et al. Comparing balloon dilation to non-balloon dilation for access in ultrasound-guided percutaneous nephrolithotomy: A systematic review and meta-analysis. Int. Braz J. Urol. 50(1), 7–19 (2024).
Levy, M. M. et al. Outcomes of the surviving sepsis campaign in intensive care units in the USA and Europe: A prospective cohort study. Lancet Infect. Dis. 12(12), 919–924 (2012).
Falahatkar, R. et al. The global, prevalence, and risk factors of postoperative fever after percutaneous nephrolithotomy: A systematic review and meta-analysis. Asian J. Urol. 11(2), 253–260 (2024).
Qiu, Z. et al. Construction and validation of the nomogram predictive model for post-percutaneous nephrolithotomy urinary sepsis. World J. Urol. 42(1), 135 (2024).
Noviardi, D. et al. Preoperative inflammatory biomarkers analysis in prognosis of systemic inflammatory response syndrome following percutaneous nephrolithotomy: A systematic review and meta-analysis. Arab. J. Urol. 21(2), 108–117 (2023).
Sahan, A. et al. Safety of upper pole puncture in percutaneous nephrolithotomy with the guidance of ultrasonography versus fluoroscopy: A comparative study. Urol. Int. 104(9–10), 769–774 (2020).
Ghani, K. R. et al. Trends in percutaneous nephrolithotomy use and outcomes in the United States. J. Urol. 190(2), 558–564 (2013).
IBM Corp. Released 2019. BM SPSS Statistics for Windows VA, NY: IBM Corp. In.
Fernström, I. & Johansson, B. Percutaneous pyelolithotomy. A new extraction technique. Scandinavian J. Urol Nephrol. 10(3), 257–259 (1976).
Türk, C. et al. EAU guidelines on diagnosis and conservative management of urolithiasis. Eur. Urol. 69(3), 468–474 (2016).
Soderberg, L. et al. Percutaneous nephrolithotomy versus retrograde intrarenal surgery for treatment of renal stones in adults. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD013445.pub2 (2023).
Xiong, Y. et al. Application of ureter-lower calyx distance in the treatment of flexible ureteroscopy for less than 2 cm lower pole kidney stones. J. Clin. Urol. 38(06), 418–420 (2023).
Ghani, K. R. et al. Percutaneous nephrolithotomy: Update, trends, and future directions. Eur. Urol. 70(2), 382–396 (2016).
Liu, M. et al. Selective tubeless minimally invasive percutaneous nephrolithotomy for upper urinary calculi. Minerva Urol. Nefrol.= Italian J. Urol. Nephrol. 69(4), 366–371 (2017).
Xingyu, Z. et al. Indication selection and efficacy observation of tubeless percutaneous nephrolithotomy. Chin. J. Endourol. 17(05), 512–515 (2023).
Jian, L., Qiang, W., Shuang, C., Shouyan, L. & Xiubo, Z. Clinical comparative study on different kinds of tubeless PCNL in the treatment of patients with renal calculi. J. Clin. Urol. 35(07), 562–565 (2020).
Lei, B. Discussion on the indications for complete and partial tubeless percutaneous nephrolithotomy. Guide China Med. 18(29), 12–14 (2020).
Jou, Y. C., Cheng, M. C., Sheen, J. H., Lin, C. T. & Chen, P. C. Cauterization of access tract for nephrostomy tube-free percutaneous nephrolithotomy. J. Endourol. 18(6), 547–549 (2004).
Funding
National Outstanding Youth Science Fund Project of National Natural Science Foundation of China, 82102787.
Author information
Authors and Affiliations
Contributions
Lei Liu, Xiaoping Zhang and Wencheng Li designed and performed the research; Xinwei Li and Gen Yang collected the data; Yuanpeng Zhang analysed the data; Yuanpeng Zhang and Lei Liu wrote the paper.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical statement
This retrospective study was approved by the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology, affiliated Union Hospital(0620). All research was performed in accordance with relevant guidelines/regulations, and we confirmed that informed consent was obtained from all participants and/or their legal guardians. All research had been performed in accordance with the Declaration of Helsinki.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary Video 1.
Supplementary Video 2.
Supplementary Video 3.
Supplementary Video 4.
Supplementary Video 5.
Supplementary Video 6.
Supplementary Video 7.
Supplementary Video 8.
Supplementary Video 9.
Supplementary Video 10.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, Y., Li, X., Yang, G. et al. Therapeutic experience and key techniques of tubeless percutaneous nephrolithotomy. Sci Rep 15, 1106 (2025). https://doi.org/10.1038/s41598-024-84806-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-84806-1
