
Abstract
Drowning ranks as the third leading cause of unintentional injury deaths globally. We conducted a systematic analysis of drowning mortality and its associated risk factors. Data on mortality, years of life lost (YLLs), and risk factors related to drowning (ICD–10 codes W65-74) from 204 countries and territories between 1980 and 2021 were obtained from the Global Burden of Disease 2021. Countries and territories were classified into five Socio-demographic Index (SDI) groups. The age-period-cohort (APC) model was used to estimate the effects of age, period, and cohort, along with the net drift, which reflects the annual percentage change over the study period. We additionally examined drowning mortality attributable to three risk factors: high alcohol use, high temperature, and occupational injuries. Globally, an estimated 233 906 premature deaths and 15.0 million YLLs were related to drowning in 2021, marking a 54.5% and 66.2% reduction, respectively, compared to 1980. The global age-standardised mortality rate (ASMR) also declined substantially from 11.09 per 100 000 in 1980 to 3.16 per 100 000 in 2021. Low-middle and low SDI countries exhibited the highest ASMR for drowning (3.81 and 4.47 per 100 000), nearly four times higher than high SDI countries (0.99 per 100 000). Encouragingly, certain countries like China (net drift: − 2.54%) and India (− 1.75%) demonstrated significant progress. From 1990 to 2021, the ASMR of drowning mortality attributable to high temperature or occupational injuries exhibited declining trends. Conversely, the ASMR attributable to high alcohol use showed an increasing trend in some middle, low-middle, and low SDI countries. Despite substantial reductions, drowning remains a significant contributor to premature mortality, particularly in middle, low-middle, and low SDI countries. As most premature drowning deaths are linked to preventable and modifiable risk factors, targeted strategies addressing these factors are essential to further reduce these fatalities.
Similar content being viewed by others

Drowning is a preventable public health crisis, accounting for nearly 236 000 deaths worldwide in 2019, exceeding the number of deaths from either protein-energy malnutrition or maternal conditions1. Although global efforts have contributed to extending global life expectancy2,3, drowning still causes a serious burden, and thus undermines progress4. Among adolescents, drowning is the leading cause of unintentional injuries, which is largely attributable to an underdeveloped ability to assess risk and inadequate swimming and water safety skills, underscoring the necessity of prevention5.
For a long time, rather than being recognized as a preventable cause of death, drowning was treated as an accident, reflecting a lack of supervision6. In the last decade, new narratives about the preventable nature of drowning deaths have emerged, exemplified in two reports from the WHO that highlighted evidence-based interventions to reduce drowning deaths7,8. In April 2021, the first drowning prevention resolution was adopted by the United Nations General Assembly9, which also emphasized the importance of drowning prevention. However, the resolution did not establish specific targets for drowning prevention, and drowning prevention is not embedded in the Sustainable Development Goals (SDGs)10.
The first drowning prevention resolution outlined the associations between drowning and social, economic, and environmental determinants such as rurality, poverty, access to water and sanitation, health inequities, and climate change9. Although all regions and economies have a drowning burden, a policy analysis indicated that this is disproportionately distributed, with high rates in Africa and high burdens in Asia11. Consistent with many other health burdens, low- and middle-income countries (LMICs) account for 90% of global unintentional drowning mortality7. Assessing drowning trends by country, including by Socio-demographic Index (SDI) groups, would assist in identifying regions where efforts are most needed to reduce drowning deaths. To date, studies have primarily focused on global trends12,13, specific regions14, or individual countries, often considering drowning within the larger context of injury burden4,15. Furthermore, to the best of our knowledge, no studies have assessed the age effects, period effects, and cohort effects of drowning mortality, effects which have the unique ability to parsimoniously describe the complex social, historical, and environmental factors that affect individuals and that might help understand time-varying elements in drowning epidemiology16,17. Finally, no studies have explored the extent to which drowning mortality is attributable to different risk factors or analyzed drowning mortality at a sub-regional level.
The purpose of this study is to systematically and comprehensively analyze trends in premature mortality from drowning and its risk factors in different countries and territories from 1980 to 2021, utilizing data from the Global Burden of Disease (GBD) 2021 study. We additionally aim to explore the age, period, and cohort effects of drowning mortality. We hypothesized that drowning mortality and the balance of its risk factors have shifted from 1980 to 2021, with variations across SDI groups. We additionally hypothesize that the age-period-cohort effect of drowning mortality will vary by country.
Methods
Study design
This study was a secondary analysis of GBD 2021 data provided by the Institute for Health Metrics and Evaluation (IHME), Seattle, Washington.
Data sources
GBD 2021 provides the incidence, prevalence, mortality, risk exposure, and burden attributable to risk factors of 371 diseases and injuries for 204 countries and territories and 811 subnational locations between 1980 and 20213,18. The detailed methodology of GBD 2021 has been published elsewhere3,18. In brief, the GBD uses all relevant data and employs the meta-regression—Bayesian, regularised, trimmed (MR–BRT) tool to derive estimates of the burden of various diseases. Data on mortality, years of life lost (YLLs), and risk factors for drowning, as well as population data for those younger than 70 years (in five-year age groups) were obtained from the GBD 2021 study for 204 countries and territories over a 42-year period (https://vizhub.healthdata.org/gbd-results/). The SDI for each country and territory was also obtained from GBD (https://www.healthdata.org/research-analysis/gbd).
Variables and definitions
In this study, we define premature mortality as any death before 70 years of age19. The term “drowning” refers to unintentional drowning and submersion (ICD–10 codes W65-74)12, which we used to measure the burden of drowning deaths.
Statistical analysis
We used mortality and the global standard population in 2021 to calculate the age-standardized mortality rate (ASMR) for people aged 0 to 69 years in each country and territory. SDI in 2019 was used to classify 204 countries and territories into five groups: high SDI, high-middle SDI, middle SDI, low-middle SDI, and low SDI. We fitted a local polynomial curve to reflect the nonlinear relationship between premature mortality and SDI20.
Age-period-cohort analysis
The age-period-cohort (APC) model was utilized to estimate age, period, and cohort effects. Within this model, age effects–reflecting biological, social processes, and social role or status of specific age groups (e.g., physiologic changes related to aging16,17)–were defined as the fitted longitudinal age-specific rates in the reference cohort adjusted for period deviations. Period effects–reflecting the external factors that affect all age groups simultaneously at a specific period (e.g., environmental or socio-economic factors16,17)–were defined as the rate ratio (RR) in a specific calendar year compared with the reference calendar year. Cohort effects– reflecting the unique experiences or exposures of specific cohorts as they move across periods (e.g., an education policy unique to each cohort16,17)–were defined as the RR in a specific birth cohort compared with the reference birth cohort. The regular relationship of age, period, and birth cohort is fully collinear, so it is statistically impossible to estimate their effects independently21. However, several methods have been developed to address this problem;22 for instance, the web tool (https://analysistools.cancer.gov/apc/) developed by the National Cancer Institute (NIH) can be used to estimate these effects23. We conducted an APC analysis for premature drowning mortality for all five SDI groups and all countries and territories in these SDI groups. To illustrate this, several representative countries and territories were selected from each group that either aligned with or deviated from the overall trend. The APC analysis was conducted using the R version 4.2.1 and code obtained from the web tool.
In the APC model, individuals aged 0 to 69 were divided into 14 five-year age groups, ranging from 0–4 to 65–69 years. We divided the period of time into eight periods of five years (1982–1986, 1987–1991, 1992–1996, 1997–2001, 2002–2006, 2007–2011, 2012–2016, 2017–2021). We then identified 21 five-year birth cohorts, from 1915 to 1919 (referred to by the midpoint as the 1917 cohort) to 2015–2019 (the 2017 cohort). For each cohort, we used the average five-year population data and the average five-year mortality data to indicate the population and mortality data of that cohort. We set the period 1987–1991 and the 2002 cohort as the reference period and cohort by default, respectively. Besides that, we also calculated local drift and net drift, representing the annual percentage change in each age group and the average annual percentage change of all groups, respectively. The Wald \(\:{\chi\:}^{2}\) test was utilized to test the significance of the parameters and the goodness-of-fit of the model24.
Risk factor analysis
In GBD 2021, the attributable mortality of 88 risk factors and combinations of risk factors were estimated at the global level, regionally, and for 204 countries and territories during 1990 and 202118. High alcohol use, high temperature and occupational injuries are identified as risk factors for drowning, while low temperature is reported to have a protective effect25,26. In this study, we focused on the three factors associated with the excess risk of drowning. High temperature is a risk factor for people aged 0 to 69 years old, while GBD models high alcohol use and occupational injuries as risk factors for people aged 15 to 69 years old. GBD estimates the attributable burden of high alcohol use, high temperature and occupational injuries through a series of processes, including the estimation of relative risk as a function of exposure for pairs between drowning and each risk factor, the determination of theoretical minimum risk exposure level, the estimation of population attributable fraction and attributable burden, and the evaluation of the direct relationship between these risk factors and drowning, as previously described18. The estimation of risk factors in GBD is based on the comparative risk assessment, and attributable burden and avoidable burden were used to complete the estimation of each risk-outcome pair18. In this study, we analyzed the burden of drowning mortality attributable to these three risk factors in each SDI group as well as at the country level. All analyses were conducted in the R version 4.2.1.
Results
Global and national trends of premature drowning mortality, 1980–2021
Globally in 2021, there were approximately 233 906 (95% confidence intervals [CI]: 211 954, 257 154, male: 170 790 [154 634, 186 423] vs. female: 63 153 [56 115, 70 561]) deaths from drowning and 15.0 (13.4, 16.8) million YLLs (male: 10.8 [9.7, 12.1] million vs. female: 4.2 [3.6, 4.8] million). Compared with 1980, this was a 59.3% and 66.2% reduction in drowning deaths and YLLs, respectively (Fig. 1, Figure S1, Figure S2, Figure S3). In 2021, 135 countries had at least 50 drowning deaths (Table S1). The leading five countries for the number of drowning deaths in 2021 were India (44 228, [36 707, 52 808]), China (42 657, [34 949, 51 896]), Pakistan (13 741, [10 054, 18 324]), Nigeria (9 923, [5 640, 15 278]), and Bangladesh (8 316, [5 867, 11 366]), all of which were in middle, low-middle or low SDI groups. Moreover, 83.8% of drowning deaths occurred in middle SDI (70 144 [64 123, 75 924]), low-middle SDI (71 264 [62 880, 79 369]), and low SDI (54 383 [43 725, 64 398]) groups in 2021.
The ASMR of premature drowning mortality was 3.16 (95%CI 2.87,3.48) per 100 000 (male: 4.56 [4.14, 5.00] per 100 000 vs. female: 1.73 [1.54, 1.94] per 100 000), representing a 71.5% decrease from 1980. The ASMR of drowning was inversely related to SDI, with a higher ASMR in countries and territories from low SDI (4.47 [4.43, 4.52] per 100 000) and low-middle SDI groups (3.81 [3.78, 3.84] per 100 000), nearly four times as high as in the high SDI group (0.99 [0.97, 1.01] per 100 000) in 2021 (Figs. 1 and 3). In the middle SDI (18.38 [18.31, 18.45] in 1980 vs. 6.73 [6.68, 6.77] in 2021) and low-middle SDI (20.21 [20.12, 20.30] vs. 7.83 [7.77, 7.88]) groups, the proportion of drowning among total injury deaths declined significantly from 1980 to 2021, but the decline was less significant in the low SDI group (15.37 [15.27, 15.48] vs. 8.69 [8.62, 8.76]). (Figs. 1, 2 and 3). Drowning was the second and fifth leading cause of injuries in children aged 0 to 14 and in those aged 15 to 69, respectively, in 2021 (Figure S4).
The three countries with the highest ASMR for premature drowning mortality in 2021 were the Solomon Islands (12.12 [95%CI 9.40, 15.69] per 100 000), Central African Republic (11.57 [10.65, 12.61] per 100 000), and Haiti (9.87 [9.33, 10.43] per 100 000) (Fig. 2, Table S1, Figure S5, Figure S6). 117 countries and territories showed significantly declining trends in ASMR from 1980 to 2021. Among these, the Republic of Korea (net drift: − 5.81 [− 6.02, − 5.59]) declined fastest, followed by Latvia (− 4.00 [− 4.52, − 3.48]) and Georgia (− 3.99 [− 4.47, − 3.51]). Other large population countries, such as China (− 2.54 [− 2.67, − 2.42]), India (1.75 [− 1.92, − 1.58]), and Brazil (− 2.45 [− 2.55, − 2.34]), also experienced positive trends. Two countries showed deteriorating trends in drowning, both from the low-middle SDI group, namely Zimbabwe (0.92 [0.39, 1.45]) and Lesotho (1.96 [1.95, 2.88]) (Fig. 4, Table S1, Figure S7).
Age, period, and cohort effects on premature drowning mortality
We found that in the high and high-middle SDI groups, many countries, including the United States of America (Net drift: − 1.42 [95%CI − 1.56, − 1.28]) and France (− 2.31 [− 2.54, − 2.08]), showed positive trends, driven by declining period and cohort risks, along with low premature drowning mortality rates. However, exceptions do exist—for example, the burden of drowning mortality among Japanese people aged 60 to 69 years showed a significantly rising trend, the mortality rate remained high throughout the study period.
In the middle SDI group, the burden of drowning deaths remained high, although many countries, such as China (− 2.54 [95%CI − 2.67, − 2.42]) and Indonesia (− 1.30 [− 1.54, − 1.07]), showed decreasing period and cohort risks and had therefore achieved improvements over the entire period. In Thailand (0.01 [− 0.22, 0.25]), the period risk only declined after 2005.
In the low-middle and low SDI groups, although some countries, such as India (1.75 [95%CI − 1.92, − 1.58]) and Ethiopia (− 3.36 [− 3.63, − 3.09]), had notably declining trends across both periods and birth cohorts, Zimbabwe (0.92 [0.39, 1.45]) and Lesotho (1.96 [1.95, 2.88]) were the only two countries with increasing cohort risks for near all cohort and period risks for the period after 1994, with deteriorating drowning trends in almost all age groups across the past four decades. (Fig. 4, Figure S8, Figure S9).
Risk factors for premature drowning mortality
A decreasing burden of drowning mortality attributable to high alcohol use was found in many high-middle and high SDI countries. Conversely, an increasing burden was found in some middle, low-middle, and low SDI countries, such as Lesotho, where the ASMR increased from 0.12 (95% CI 0.00, 0.92) per 100 000 in 1990 to 0.26 (0.05, 0.92) per 100 000 in 2021.
Although declining trends in the risks of drowning attributable to high temperatures were found in all five SDI groups, there were only marginal improvements in the low SDI group, with total deaths decreasing from 2 771 (1 217, 4 158) in 1990 to 2 604 (1 105, 3 829) in 2021. These trends were also observed in some low SDI countries, such as Guinea (41 in 2021 vs. 34 in 1990) and Mozambique (59 vs. 54).
For drowning mortality attributable to occupational injuries, many countries and territories showed declining ASMR trends. The exception was some high SDI countries, such as the United States of America and France, which had low ASMR in both 1990 and 2021. However, the number of drowning deaths attributable to occupational injuries showed little change between 1990 and 2021 in some low-middle and low SDI groups, such as India (14 913 in 1990 vs. 14 094 in 2021) and Zimbabwe (59 vs. 48). Some countries even had increasing numbers of deaths attributable to occupational injuries, such as Mozambique (124 vs. 158) and Kenya (86 vs. 115) (Fig. 5, Figure S10).
Discussion
In this study, we found a substantial reduction in global deaths from drowning over the past four decades, with more than a two-thirds (71.5%) reduction in the ASMR of premature drowning. As with other causes of mortality from injuries, males are disproportionately represented in these deaths, with nearly three times as many deaths as females. Unlike many other causes of injury, young children have the greatest risk of mortality from drowning. In 2021, countries in middle, low-middle, and low SDI groups persisted in having the highest burden of premature drowning deaths. Despite impressive gains in countries such as China, India, and Brazil, several countries had rising period and cohort risks. Furthermore, despite impressive overall declines, occupational injuries still caused a particularly heavy burden in many middle and low-middle SDI countries, including India and China, that in part explain the substantial sex differences in drowning deaths.
Adding to previous analyses from GBD 2017 and GBD 201912,13, we found high drowning premature mortality rates in middle, low-middle, and low SDI groups, which might be explained by the rising period and cohort risks in some countries, as well as the high burden attributable to all three risk factors. This phenomenon was consistent with recent findings of wider injuries among adolescents4, suggesting that countries from middle, low-middle, and low SDI groups warrant greater policy attention to drowning prevention. This is also the first study to distinguish the age, period, and cohort effects of drowning. In the context of knowledge of the nature and timing of various policy interventions, examining period and cohort effects can provide valuable insight into why some countries, especially within the same SDI group, have similar or divergent trends in drowning mortality.
The world’s two most populous countries, India and China, contribute substantially to the global burden of drowning mortality. As these countries constitute about 36% of the global population, they accounted for nearly 34% of global YLLs and 37% of global deaths from drowning in 2021, making them immensely significant due to their concentration of approximately one-third of the global burden of drowning27. However, both countries have made great progress in drowning prevention in the past four decades. In China, this was driven by a declining period risk from 1980 to 2021 and a declining cohort risk for those born after 1997. Rapid urbanization and greater participation in education may contribute to these cohort effects28. Urbanization is expected to reduce access to many natural water hazards (dams, lakes, rivers, oceans), which have a higher risk for drowning than swimming pools, which are more common in urban regions29. Occupational activities also change in the context of urbanization28. Comprehensive measures, including better monitoring of water hazards, safety signs, and greater supervision from families, may also have contributed to this declining period risk, especially for children and adolescents30. India has achieved a lower annual percentage improvement in preventable deaths from drowning than China, suggesting that greater attention is needed. In Thailand, a declining risk was seen, especially for the period after 2004, which may reflect a child drowning prevention program implemented by the Ministry of Public Health in 200631. While Bangladesh is recognised as having the world’s highest child drowning rates32, it has made strong gains, with a reduction of 80.3% for drowning ASMR from 1980 to 2021, driven by beneficial period and cohort effects. Bangladesh was early to implement drowning interventions11, such as parent education about the importance of closely supervising children, encouraging parents to use playpens to safely contain children, increasing community supervision and implementing swimming education programs33. Notwithstanding these gains, the persistently high ASMR for drowning in Bangladesh indicates residual challenges. In contrast, many countries have failed to benefit from either period or cohort effects. Zimbabwe showed a rising trend in drowning over the 25-year period from 1994 and for nearly all cohorts; no age group showed improvement in the past few decades and disappointingly, deaths increased in adults aged 25 to 50 years. These trends in Zimbabwe might be due to economic issues with growing poverty4, potentially resulting in less parent supervision, as well as gradual decay in key health and education infrastructure, especially since 200034.
Premature mortality from drowning was substantially lower in high and high-middle SDI countries. In the United States of America for example, many states have laws and policies which might contribute to this, including pool safety guidelines (e.g., self-latching gates and pool covers35), boating and water safety standards, lifeguards at beaches and public pools, as well as community norms promoting swimming lessons and basic water safety skills36. Notwithstanding this, drowning remained the 2nd leading cause of death in 1-4-year old children in high SDI countries. This, along with rebound period risks observed in some countries (e.g., Turkey and Russian Federation), suggested a need for greater emphasis on child supervision and swimming lessons for school-aged children1,37. Furthermore, we found older people in Japan suffered a heavy burden of drowning, with deteriorating trends in those aged 60 to 69 years. As one of three major causes of unintentional deaths among older adults in Japan, this might reflect patterns of bathing and additional risks of alcohol38, which warrants further attention.
Despite the high burden of premature mortality among the middle, low-middle, and low SDI groups, our analysis revealed that the low SDI group showed the least improvement from 1980 to 2021. In these countries, occupational injuries, high temperature and alcohol variably contributed to drowning mortality. Rapid industrialization, as seen in China and India, is expected to lead to more occupational-related injuries39, and while China and India have both invested in prevention of occupational injuries39,40, they do not yet have the extent of policy developments expected in high SDI countries41. High temperatures already increase the probability of water access in many middle and low-middle SDI countries, which will only be exacerbated by the climate crisis given its impact on floods42. Despite poverty providing a major challenge for countries to implement drowning prevention efforts41, there were more high temperature-related drownings in Thailand, India, and Bangladesh than in most low SDI countries. Economic growth is also expected to increase alcohol use and may be especially potent for young adult males43. Knowledge of the risk factor profile by country, as provided in this study, enables countries to implement more specific policy responses, such as those relating to occupational standards, those that reduce water hazards, and others that reduce alcohol consumption. Frustratingly, many countries in the low SDI group have made limited progress in premature drowning mortality across the past four decades. A prominent exception is Ethiopia, which experienced a sharp decline in premature drowning mortality, and improvements over the whole study period and for all birth cohorts. This might reflect deployment of Health Extension Workers to each sub-district with resultant benefits for community and parenting approaches to drowning prevention, which could serve as a valuable reference for other low-SDI countries44. Many low SDI countries, including Ethiopia, Kenya, and Somalia also experienced severe drought over this period45. While drought might be expected to reduce exposure to water hazards, it has also been reported to lead to riskier behaviour around water42.
Despite its systematic approach, this paper also has several limitations. Firstly, as a secondary analysis of the GBD data, our study is limited by the inherent limitations of the GBD study itself3. However, without the complex statistical models that the GBD study uses to estimate mortality including uncertainty estimates, low coverage of vital registration in LMICs would otherwise preclude such global analyses3,9,46. Secondly, we used unintentional drowning and submersion codes (ICD–10 W65-74) to measure the burden of drowning deaths which do not account for disaster and transport-related drownings in some countries47. These analyses should therefore be considered to underestimate the burden of death from drowning, especially in countries like Uganda, where boating accidents are a major contribution to drowning deaths48. Thirdly, our use of the APC model to explore the age, period, and cohort effects was based on repeated cross-sectional data rather than cohort data. Greater access to cohort studies is needed to further delineate relative risks. Fourthly, in this study, we only analyzed drowning mortality attributed to the three risk factors defined in GBD. This does not account for other recognized risk factors for drowning out of the GBD study, such as rurality, poverty, access to fresh water and sanitation, and climate change, which might hinder the ability to fully account for the drowning trends9. Fifthly, as data for premature drowning mortality attributed to occupational injuries and high alcohol use are only modelled by GBD for those over 15 years of age, the extent that these risks contribute to premature deaths in younger children, who are known to be particularly vulnerable to occupational injuries49, remains unknown. Considering the greatest burden of drowning deaths lies in the young in most countries, distinct policies such as family and community supervision30,33, and teaching children to swim33, are needed to reduce the drowning burden.
Conclusions
In conclusion, despite significant improvements in premature drowning mortality worldwide, a substantial burden persists, especially in children and adolescents from middle, low-middle and low SDI countries. Greater attention to these three risk factors is warranted given their variable contribution to the burden of premature drowning mortality in these types of countries. Prioritize interventions that have been proven effective in countries with a similar SDI is encouraged, with the goal of extending life expectancy and contributing to the Sustainable Development Goals.

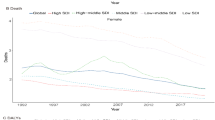
Trends of premature drowning deaths in each SDI group, between 1980 and 2021. (A) Number of premature drowning deaths. (B) ASMR of premature drowning mortality. (C) Proportion of drowning deaths among total injury deaths. Note: ASMR = age standardized mortality rate. SDI = Socio-demographic Index.

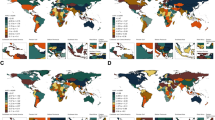
Heatmap of premature mortality (ASMR) from drowning among 204 countries and territories in (A) 1980 and (B) 2021. Note: ASMR = age standardized mortality rate. Map created using R version 4.2.1 (https://www.r-project.org/).

Association between premature drowning mortality (ASMR) and Socio-demographic Index (SDI) in 2021. Note: ASMR = age standardized mortality rate. SDI = Socio-demographic Index. BGD = Bangladesh, BRA = Brazil, CHN = China, ETH = Ethiopia, IDN = Indonesia, IND = India, MEX = Mexico, NGA = Nigeria, PAK = Pakistan, PHL = Philippines, RUS = Russian Federation, USA = United States of America. EGY = Egypt.

Age, period, and cohort trends in premature drowning mortality in selected typical countries and territories, 1982–2021. Note: SDI = socio-demographic Index. MR = mortality rate. RR = rate ratio. The error bars represent the 95% confidence interval of the estimate.

Premature drowning mortality attributable to three risk factors in selected countries and territories in 1990 and 2021. (A) ASMR. (B) Number of deaths. Note: ASMR = age standardized mortality rate. SDI = socio-demographic index.
Data availability
All data utilized in this study can be accessed freely at the GBD 2021 portal (https://vizhub.healthdata.org/gbd-results/).
References
Meddings, D. R., Scarr, J. P., Larson, K., Vaughan, J. & Krug, E. G. Drowning prevention: turning the tide on a leading killer. Lancet Public. Health. 6(9), e692–e5 (2021).
United Nations. THE SDGS IN ACTION. https://www.undp.org/sustainable-development-goals?utm_source=EN&utm_medium=GSR&utm_content=US_UNDP_PaidSearch_Brand_English&utm_campaign=CENTRAL&c_src=CENTRAL&c_src2=GSR&gclid=Cj0KCQjw54iXBhCXARIsADWpsG8yOCQYs-sLVhxpnOn29JGXMhLN9Evhk_ZlcEsdxCoux2oDL3Z39f8aAuG2EALw_wcB (2015).
Ferrari, A. J. et al. Global incidence. prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet 403(10440), 2133–2161 (2024).
GBD Adolescent Transport and Unintentional Injuries Collaborators. Adolescent transport and unintentional injuries: A systematic analysis using the global burden of disease study 2019. Lancet Public. Health 7(8), e657–e69 (2022).
World Health Organization. Drowning (2021). https://www.who.int/news-room/fact-sheets/detail/drowning.
Flooding drowning, and health equity: The lancet regional health - Western Pacific august editorial. Lancet Reg. Health Western Pac. 13, 100264 (2021).
World Health Organization. Global report on drowning: preventing a leading killer. (2014). https://www.who.int/publications/i/item/global-report-on-drowning-preventing-a-leading-killer.
World Health Organization. Preventing drowning: An implementation guide. 2017-05-01. https://www.who.int/publications/i/item/9789241511933.
United Nations. Global drowning prevention: Resolution/adopted by the General Assembly. (2021). https://digitallibrary.un.org/record/3925005?ln=en#record-files-collapse-header.
Ma, T. et al. Out of the silos: embedding injury prevention into the sustainable development goals. Injury Prevention: J. Int. Soc. Child. Adolesc. Injury Prev. 27(2), 166–171 (2021).
Scarr, J. P., Buse, K., Norton, R., Meddings, D. R. & Jagnoor, J. Tracing the emergence of drowning prevention on the global health and development agenda: A policy analysis. Lancet Global Health 10(7), e1058–e66 (2022).
Franklin, R. C. et al. The burden of unintentional drowning: Global, regional and national estimates of mortality from the global burden of disease 2017 study. Injury Prevention: J. Int. Soc. Child. Adolesc. Injury Prev. 26 (Supp 1), i83–i95 (2020).
Tan, H. et al. Change in global burden of unintentional drowning from 1990 to 2019 and its association with social determinants of health: Findings from the global burden of disease study 2019. BMJ Open. 13(4), e070772 (2023).
Clemens, T., Moreland, B. & Lee, R. Persistent racial/ethnic disparities in fatal unintentional drowning rates among persons aged </=29 years - United States, 1999–2019. MMWR Morbidity Mortal. Wkly. Rep. 70(24), 869–874 (2021).
Reddy, B. V., Pundhir, A. & Gupta, A. Unintentional injury and its determinants among adolescents. J. Public. Health Res. 10(4) (2021).
Columbia Public Health. Age-Period-Cohort Analysis. https://www.publichealth.columbia.edu/research/population-health-methods/age-period-cohort-analysis#Description.
Yang, Y. C. & Land, K. C. The Statistical Properties of the Intrinsic Estimator for Age-Period-Cohort Analysis. (2013).
Global burden and strength of evidence for. 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: A systematic analysis for the global burden of disease study 2021. Lancet 403(10440), 2162–2203 (2024).
World Health Organization. Premature mortality from noncommunicable disease. https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3411.
Cleveland, W. S., Grosse, E. & Shyu, W. M. Local regression models. Statistical models in S: Routledge 309 –376. (2017).
Rosenberg, P. S. & Anderson, W. F. Age-period-cohort models in cancer surveillance research: ready for prime time? Cancer Epidemiol. Biomarkers Prev. 20(7), 1263–1268 (2011).
Dinas, E. & Stoker, L. Age-period-cohort analysis: A design-based approach. Electoral. Stud. 33, 28–40 (2014).
Rosenberg, P. S., Check, D. P. & Anderson, W. F. A web tool for age-period-cohort analysis of cancer incidence and mortality rates. Cancer Epidemiol. Biomarkers Prev. 23(11), 2296–2302 (2014).
Rosenberg, P. S. & Anderson, W. F. Proportional hazards models and age-period-cohort analysis of cancer rates. Stat. Med. 29(11), 1228–1238 (2010).
IHME. Global Burden of Disease (GBD). https://www.healthdata.org/gbd/2019.
Burkart, K. G. et al. Estimating the cause-specific relative risks of non-optimal temperature on daily mortality: A two-part modelling approach applied to the global burden of disease study. Lancet 398(10301), 685–697 (2021).
Lukaszyk, C., Ivers, R. Q. & Jagnoor, J. Systematic review of drowning in india: assessment of burden and risk. Injury Prevention: J. Int. Soc. Child. Adolesc. Injury Prev. 24(6), 451–458 (2018).
Wang, Z. et al. Age-Period-Cohort analysis of trends in mortality from drowning in china: data from the global burden of disease study 2015. Sci. Rep. 8(1), 5829 (2018).
Wang, L. et al. Unintentional drowning mortality in china, 2006–2013. Injury Prevention: J. Int. Soc. Child. Adolesc. Injury Prev. 25(1), 47–51 (2019).
Ministry of Education of the People’s Republic of China. The ministry of education and other four departments plans to prevent drowning among primary and middle school students (in Chinese). (2022). http://www.moe.gov.cn/jyb_xwfb/gzdt_gzdt/s5987/202207/t20220729_649584.html.
Ministry of Public Health Thailand. Drowning Prevention in Thailand (2014).
Jagnoor, J., Kobusingye, O. & Scarr, J. P. Drowning prevention: Priorities to accelerate multisectoral action. Lancet 398(10300), 564–566 (2021).
Linnan, M., Scarr, J. & Giersing, M. Toward a world where children do not drown. JAMA Pediatr. 167(2), 110–111 (2013).
Makoni, M. COVID-19 worsens zimbabwe’s health crisis. Lancet 396(10249), 457 (2020).
Theodorou, C. M., Rajasekar, G., McFadden, N. R., Brown, E. G. & Nuno, M. Epidemiology of paediatric drowning hospitalisations in the USA: A population-based study. Injury Prevention: J. Int. Soc. Child. Adolesc. Injury Prev. 28(2), 148–155 (2022).
Moreland, B., Ortmann, N. & Clemens, T. Increased unintentional drowning deaths in 2020 by age, race/ethnicity, sex, and ___location, United States. J. Saf. Res. 82, 463–468 (2022).
Denny, S. A. et al. Prevention of drowning. Pediatrics 148(2) (2021).
Aoki, Y., Ishizawa, M. & Hirata, H. Recent trends in three major unintentional accidental deaths among older people in japan: stumbling falls, bathtub drowning and food choking. Geriatr. Gerontol. Int. 24(1), 182–184 (2024).
Gong, P. et al. Urbanisation and health in China. Lancet 379(9818), 843–852 (2012).
Saha, R. K. Occupational health in India. Annals Global Health. 84(3), 330–333 (2018).
LaDou, J., London, L. & Watterson, A. Occupational health: A world of false promises. Environ. Health: Global Access. Sci. Source 17(1), 81 (2018).
Sindall, R. et al. Drowning risk and climate change: a state-of-the-art review. Injury Prev.: J. Int. Soc. Child. Adolesc. Injury Prev. 28(2), 185–191 (2022).
GBD Alcohol Collaborators. Population-level risks of alcohol consumption by amount, geography, age, sex, and year: A systematic analysis for the global burden of disease study 2020. Lancet 400(10347), 185–235 (2022).
Amouzou, A. et al. Using health extension workers for monitoring child mortality in real-time: Validation against household survey data in rural Ethiopia. PloS One 10(11), e0126909 (2015).
Center for Disaster Philanthropy. Horn of Africa Hunger Crisis. (2023). https://disasterphilanthropy.org/disasters/horn-of-africa-hunger-crisis/?gclid=EAIaIQobChMItbax4suU_QIVvw2tBh2mFA17EAAYASAAEgLVcvD_BwE.
Haagsma, J. A. et al. The global burden of injury: incidence, mortality, disability-adjusted life years and time trends from the global burden of disease study 2013. Injury Prev.: J. Int. Soc. Child. Adolesc. Injury Prev. 22(1), 3–18 (2016).
Peden, A. E., Franklin, R. C., Mahony, A. J., Scarr, J. & Barnsley, P. D. Using a retrospective cross-sectional study to analyse unintentional fatal drowning in australia: ICD-10 coding-based methodologies verses actual deaths. BMJ Open. 7(12), e019407 (2017).
Clemens, T. et al. Drowning in uganda: examining data from administrative sources. Injury Prev.: J. Int. Soc. Child. Adolesc. Injury Prev. 28(1), 9–15 (2022).
Patton, G. C. et al. Our future: A lancet commission on adolescent health and wellbeing. Lancet 387(10036), 2423–2478 (2016).
Funding
Supported by National Natural Science Foundation of China (82273654, 82073573).
Author information
Authors and Affiliations
Contributions
Y.L., Z.Z., and Y.S. conceived this study. Y.L. accessed the data, did the primary analysis, formulated the figure and table, and drafted the first version of the manuscript. D.L., P.Z., J.D. contributed to the interpretation the results and the review of manuscript. D.S., S.C., Z.C., M.F., P.T. contributed to reviewing the manuscript. J.M. and S.M.S. critically reviewed and substantially edited the manuscript. Z.Z. and Y.S. were responsible for general supervision and had final responsibility for the decision to submit for publication. All authors reviewed the article, read the final version of manuscript and approved the submission.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liu, Y., Luo, D., Zhong, P. et al. Burden and risk factors of premature drowning mortality in 204 countries and territories, 1980–2021. Sci Rep 15, 21036 (2025). https://doi.org/10.1038/s41598-025-05418-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-05418-x
