
Abstract
Evidence supports the efficacy of positive psychology interventions (PPIs) for enhancing mental well-being, yet the effectiveness of brief, multicomponent PPIs and the role of civic engagement within educational settings remain inadequately understood. This study investigated both the impact of an 8-week positive education programme on student mental well-being in Hong Kong and other Asia Pacific regions, and examined civic engagement’s mediating role in intervention outcomes. Participants (N = 112) were randomly assigned to experimental or waitlist control groups. The intervention incorporated multiple positive psychology topics and civic engagement components. The experimental group demonstrated significant improvements in growth mindset, resilience, prosocialness, positive emotions, general health, and reduced insomnia severity compared to the waitlist control group, with civic engagement behaviors also showing a significant increase. Mediation analyses revealed that civic engagement mediated the relationship between resilience and well-being in the experimental group, while showing an unexpected negative association in the waitlist control group. This differential effect highlights civic engagement’s complex role in well-being interventions, while demonstrating the effectiveness of structured brief, multicomponent PPIs in enhancing participants’ well-being. The study reveals that structured support is potentially crucial for maximizing benefits. These insights inform the design of effective well-being interventions in higher education settings.
Similar content being viewed by others
Introduction
Mental well-being, according to the WHO1, allows individuals to cope with life’s challenges, realize personal abilities, work productively, and contribute to society, forming a crucial part of overall health. It goes beyond the absence of mental disorders, highlighting positive functioning and fulfillment in daily life. As a fundamental component of overall health, mental well-being is positively correlated with a variety of critical outcomes during adolescence and young adulthood, such as increased long-term life satisfaction, academic success, and enhanced relationships2,3,4. Despite the broad recognition of these benefits, university students often face specific sets of challenges that jeopardize their mental well-being, including academic pressures, financial concerns, and social transitions5,6. These challenges to student mental well-being have become increasingly concerning globally, particularly in competitive higher education environments. This is evidenced by the detrimental impact of the post-pandemic mental health crisis observed7, and the increasing proportion of students suffering from moderate to severe levels of anxiety and depressive symptoms8,9. Our study, conducted with participants from Hong Kong and other Asia Pacific regions, provides an opportunity to examine the intervention’s general effectiveness in diversified student populations. Given these challenges, there is a pressing need for suitable and effective interventions that can promote well-being among a diverse range of university students. By including participants from diverse Asia Pacific regions, our study aims to assess the broad applicability of this intervention.
Positive psychology interventions (PPIs) and positive education
Positive psychology, a field dedicated to understanding how individuals and communities thrive and achieve their fullest potential10,11, has garnered increasing attention in mental health research. The field of mental health has seen the rise of positive psychology interventions (PPIs) as a method for boosting psychological well-being in various groups. Research has indicated that these approaches generally yield favorable results, though the extent of their impact can differ2,10,12,13,14. These interventions aim to boost positive emotions, thoughts, and behaviors by focusing on key positive psychological constructs, including resilience15,16,17, gratitude18,19, growth mindset20,21,22 and stress coping strategies23, all of which play crucial roles in promoting overall well-being. Resilience refers to an individual’s capacity to adapt positively in the face of adversity17,24. Gratitude is about recognizing and appreciating the positive dimensions and experiences in life18,25. Growth mindset represents the belief that abilities and intelligence can be developed through effort and learning21,26. Stress coping strategies involve employing healthy and adaptive techniques for managing stress, such as problem-solving, seeking social support, and engaging in relaxation techniques27. These constructs, among others, form the foundation of many PPIs and play crucial roles in promoting psychological well-being15,19,22.
Additionally, PPIs can equip participants with practical skills beneficial for well-being. One such skill often incorporated is basic counseling techniques, which can enhance individuals’ ability to provide emotional support and engage in effective communication28,29. These skills not only benefit the participants themselves but can also positively impact their interpersonal relationships and community interactions.
On the other hand, recent meta-analyses have provided a more nuanced understanding of the efficacy of PPIs, highlighting that the effect could vary across various populations and contexts. The study by Hendriks and collaborators30 revealed that PPIs enhanced both subjective and psychological wellness, yielding small to medium-sized effects. Recent evidence suggests more modest effect sizes for PPIs in university settings, though these interventions remain effective for enhancing well-being and reducing depressive symptoms31.
These mixed findings underscore both the potential of PPIs for promoting mental health in academic settings and the need for further research on factors influencing their effectiveness. The variability in outcomes suggests that there may be unexplored mechanisms or contextual factors that moderate the impact of PPIs, particularly in diverse settings such as university environments. This variability also highlights the importance of investigating different approaches to enhance PPI effectiveness. Among these approaches, low intensity PPIs delivered through positive education have gained particular attention due to their potential for widespread implementation. In educational settings, low intensity interventions, also referred to as “small” interventions, typically involve workshop or class-based, group-oriented programs that last for approximately 8 sessions, each lasting one to two hours32. Some protocols also consider mixed teaching and service participation programmes, conducted once per week for less than 20 weeks, as low intensity interventions33. In this study, our programme was designed as an 8-week workshop for groups of participants, with each session lasting 1.5 h, aligning with these standards for small, low intensity interventions. Moreover, this format was chosen to fit within the academic schedules of the participating institutions.
Importantly, while systematic reviews have suggested that the effectiveness of PPIs can vary2,13,14, it is notable that even low intensity PPIs can yield small but significant improvements in well-being2. These effects, though modest, can be potentially valuable due to their wide dissemination and impact potential2,34,35.
Given the findings that low intensity PPIs not only offer the potential for significant effects but are also cost-effective and less burdensome, they suit university students with demanding schedules. One common method of delivering these interventions is through positive education in classroom and seminar formats, structured as short courses to seamlessly integrate into the academic environment4,10,14. Properly implemented positive education programs provide a highly practical, accessible, and widespread option for enhancing well-being among individuals needing to balance multiple commitments36,37,38.
Although research has demonstrated the effectiveness of positive education as a type of PPIs, its success varies significantly across different contexts and populations14,39. This variability underscores the necessity of identifying the key components that drive success in utilizing positive education for implementing low intensity PPIs. Despite this need, there is currently little conclusive understanding of the critical factors that could enhance the effectiveness of these interventions, indicating a promising area for further research.
One potential key consideration in designing effective low intensity PPIs within positive education is the multifaceted nature of well-being40. While many existing PPIs require substantial time investment—often entailing multiple weekly sessions—they typically focus on a single component such as gratitude or mindfulness; this approach may limit their comprehensive impact and result in varied effects on well-being5,18,41. Interestingly, despite similar time commitments, studies have indicated that time-intensive PPIs that cover multiple components may yield stronger effects in enhancing various aspects that contribute to overall well-being5.
This suggests that multifaceted PPIs may be more effective in enhancing well-being than those focusing on one specific topic, even if the time dedicated to each topic is reduced. Recent studies have further supported this notion, demonstrating that multicomponent PPIs can lead to significant improvements across various well-being domains30,42. Importantly, this advantage may extend beyond more time-intensive PPIs to low intensity, short-term positive education programmes. However, the potential of such multifaceted, short-term, positive education programmes has not been thoroughly explored, highlighting a notable gap in current research. Therefore, developing and empirically evaluating these time-efficient and broadly impactful programmes are essential to confirm their benefits and to tailor them to the practical needs of university students.
While multicomponent PPIs offer promising potential, their effectiveness might be further enhanced by incorporating elements that address broader aspects of students’ lives. One such element, which has received increasing attention in recent years, is civic engagement. The following section explores how civic engagement might complement and enhance the effects of multicomponent PPIs.
The role of civic engagement in PPIs
Civic engagement could be a key factor in enhancing the effectiveness of low intensity PPIs. Civic engagement involves efforts by individuals or groups to address community challenges, often nurtured through ambassador programs that equip participants to serve the public good43. Studies have indicated that participation in civic activities may satisfy key psychological needs identified in Self-Determination Theory (SDT) - namely autonomy, competence, and relatedness, which can potentially contribute to improved well-being44,45. This hints at the potential for civic engagement to be linked to the effectiveness of PPIs on well-being. However, the extent to which civic engagement might mediate or simply enhance the PPI and/or overall well-being remains unclear. Particularly, there is a lack of understanding about how civic engagement might interact with or potentially amplify the effects of other factors that contribute to well-being within the context of a multicomponent PPI.
While findings are not entirely consistent, cross-sectional research has indicated positive relationships between civic engagement and factors such as resilience and life satisfaction44,46, indicating potential pathways through which civic engagement could mediate the impact of PPI components —particularly resilience— on overall well-being. Furthermore, longitudinal studies have shown that civic engagement during adolescence and young adulthood predicts better psychological well-being and life satisfaction in later years47,48, suggesting a potential long-term benefit of incorporating civic engagement into PPIs. Theoretically, one possible interpretation could be through SDT, which posits that resilience—the ability to adapt to adversity—is strengthened when basic psychological needs are fulfilled. Civic engagement, by providing opportunities for autonomy, competence, and relatedness, might therefore act as a mediator, indirectly linking resilience to improved well-being. However, the specific mediating role of civic engagement within low intensity PPIs, particularly in a positive education setting, remains unexplored and has not been empirically tested. Investigating this gap could enhance our understanding of how civic engagement influences well-being within the framework of PPIs, thereby improving the design and execution of these interventions. Therefore, although the PPI used in our current study is multicomponent, our path analysis of the effects of civic engagement focused on resilience, as it represents a key mechanism by which civic engagement may affect overall well-being.
Research gaps and current study
Our critical examination of existing research has revealed several significant areas that warrant further investigations:
-
1.
The effectiveness of short-term, low intensity PPIs that incorporate multiple positive psychology topics in a university setting.
-
2.
The extent to which civic engagement mediates or enhances the PPI and/or overall well-being.
To address these gaps, the current study aims to examine the effectiveness of a short-term, low intensity PPI that incorporates multiple positive psychology topics (resilience, gratitude, growth mindset, stress coping and counseling skills) and civic engagement components in promoting well-being among university students, we hypothesize that:
-
1.
Participants in the multicomponent PPI group will demonstrate greater improvements in multiple factors contributing to well-being and overall well-being outcomes compared to a waitlist control group.
-
2.
Civic engagement will mediate the relationship between PPI components, resilience and well-being outcomes, strengthening the overall effect of the intervention.
-
3.
Civic engagement will enhance the well-being outcomes.
The current study aims to contribute to the research on accessible and effective interventions for promoting mental well-being among university students. Theoretically, this study could enhance our understanding of how different components of PPIs interact and how civic engagement may mediate their effects. Practically, our results could inform the development of more effective, efficient, and engaging interventions for university students, potentially leading to improved mental health outcomes at a population level. By recruiting participants from diverse Asia Pacific regions, our study provides a comprehensive evaluation of the intervention’s generalizability.
Results
To evaluate the effectiveness of the programme, we conducted Analyses of Covariance (ANCOVAs) to examine post-test score differences between the experimental and waitlist control groups, controlling for baseline measures and gender. The results are presented in Table 1. In our analyses, we report partial eta squared (η2p) as our primary effect size measure, with values of approximately 0.01, 0.06, and 0.14 representing small, medium, and large effects, respectively.
Components contributing to Well-being
The programme showed significant positive effects on several components contributing to well-being. Participants in the experimental group demonstrated significantly higher levels of growth mindset related to intelligence (F(1, 109) = 5.543, p = .020, η2p = 0.028), resilience (F(1, 109) = 5.644, p = .019, η2p = 0.027), and prosocialness (F(1, 109) = 7.086, p = .009, η2p = 0.039) compared to the control group.
Trends towards improvement were observed in counselling self-efficacy (F(1, 109) = 3.74, p = .056, η2p = 0.030) and growth mindset related to personality (F(1, 109) = 2.79, p = .098, η2p = 0.016), though they did not reach statistical significance. No significant difference was found for gratitude (F(1, 109) = 0.088, p = .768, η2p = 0.001).
Well-being outcomes
The programme had significant positive effects on several well-being outcomes. Experimental group participants reported significantly higher levels of positive emotions (F(1, 109) = 6.344, p = .013, η2p = 0.041) and general health (F(1, 109) = 8.777, p = .004, η2p = 0.049) compared to the control group. Moreover, the experimental group showed significantly lower insomnia severity (F(1, 109) = 3.97, p = .049, η2p = 0.024), indicating improved sleep quality.
For physiological symptoms (F(1, 109) = 2.091, p = .151, η2p = 0.018) and psychological symptoms (F(1, 109) = 2.087, p = .151, η2p = 0.011), the differences did not reach statistical significance, although trends toward improvement were observed.
Civic engagement
The programme demonstrated a significant positive effect on civic engagement behaviors. Participants in the experimental group reported significantly higher levels of civic engagement behaviors (F(1, 109) = 6.984, p = .009, η2p= 0.042) compared to the control group. A trend towards improvement in civic engagement attitudes was observed (F(1, 109) = 2.255, p = .136, η2p = 0.015), but this did not reach statistical significance.
Coping strategies
Regarding coping strategies, no statistically significant differences were found between the experimental and control groups. A trend towards improvement in problem-focused coping was noted (F(1, 109) = 2.752, p = .100, η2p = 0.016), whereas no significant differences were observed for emotion-focused coping (F(1, 109) = 0.744, p = .390, η2p = 0.005) or avoidant coping (F(1, 109) = 0.334, p = .564, η2p = 0.003).
An exploratory post hoc ANCOVA was conducted on variables that showed significant improvements in the experimental group to examine whether cultural background predicted post-test outcomes. After controlling for pre-test scores and gender, cultural background was not a significant predictor for any outcome, suggesting that cultural differences might have limited influence on intervention effects within our sample.
To assess the need for multilevel modeling, we calculated intraclass correlations (ICCs) for delivery method across all outcomes that showed significant effects. All ICCs were below 0.10, indicating limited between-group variability and supporting our decision to proceed with single-level models. We therefore proceeded with the simpler single-level models for all outcomes. Besides, we tested whether accounting for the nesting of participants within delivery methods improved model fit when predicting post-test scores while controlling for pre-test scores and gender. For each outcome variable, we compared a multilevel model (with random intercepts for delivery method) to a single-level model using ordinary least squares regression. In all cases, model comparisons indicated no significant difference in fit, suggesting that delivery method did not introduce meaningful variability.
As a validation of our results, we conducted the same ANCOVAs on a newly recruited participant sample (details in the Supplementary Information). The analysis showed that, with the exception of insomnia severity, all measures that were originally significant remained so, and several variables that showed only trend-level effects in the original data (counselling self-efficacy, growth mindset related to personality and civic engagement attitudes) now reached statistical significance in the expected direction, further supporting our initial findings. Notably, the supplementary sample differed from the main sample in cultural composition and delivery mode balance, yet we observed a highly consistent pattern of intervention effects. The observed similarity in results across both rounds may suggest that cultural variability may not have a strong impact on the intervention outcomes, though this remains a preliminary observation. While these findings provide some support for the potential applicability of the intervention across different contexts, we acknowledge that a fully balanced, stratified design would be needed to examine these influences more rigorously.
Path analysis
Based on this framework, we conducted two moderated mediation analyses examining relationships between pre-post changes in resilience, civic engagement, and two well-being outcomes: positive emotions and general health. Thus, we prioritized positive emotions and general health as they align with emotional well-being, a key outcome suggested in SDT. Group assignment (experimental vs. control) served as a moderator for both models.
Result of positive emotions (PE)
Table 2 illustrated the result of positive emotions. The model explained a significant portion of the variance in PE change, R² = 0.29, F(5, 106) = 8.77, p < .001.
Group assignment significantly moderated two key pathways in the model: the relationship between civic engagement and PE (β = 0.406, SE = 0.138, p < .001), and the direct relationship between resilience and PE (β = -0.195, SE = 0.220, p = .036). The relationship between resilience and civic engagement was not significantly moderated by group assignment (β = 0.014, SE = 0.287, p = .884).
In the experimental condition, resilience positively predicted civic engagement (β = 0.343, SE = 0.152, p < .001). Civic engagement positively predicted PE (β = 0.375, SE = 0.069, p < .001). The direct effect of resilience on PE was not significant (β = 0.137, SE = 0.117, p = .139). However, the indirect effect of resilience on PE through civic engagement was significant and positive (β = 0.129, SE = 0.060, p = .007).
In the control condition, resilience marginally predicted civic engagement (β = 0.315, SE = 0.243, p = .052). Civic engagement negatively predicted PE (β = -0.364, SE = 0.069, p < .001). The direct effect of resilience on PE was strong and positive (β = 0.452, SE = 0.181, p < .001). The indirect effect was marginally significant and negative (β = -0.114, SE = 0.089, p = .071).
Result of general health (GHQ)
Table 3 illustrated the result of general health. The model explained a significant portion of the variance in GHQ change, R² = 0.24, F(5, 106) = 6.60, p < .001.
Group assignment significantly moderated two key pathways in the model: the relationship between civic engagement and GHQ (β = 0.209, SE = 0.080, p = .018), and the direct relationship between resilience and GHQ was marginally moderated (β = -0.185, SE = 0.127, p = .054). The relationship between resilience and civic engagement was not significantly moderated by group assignment (β = 0.014, SE = 0.287, p = .884).
In the experimental condition, resilience positively predicted civic engagement (β = 0.343, SE = 0.152, p < .001). Civic engagement positively predicted GHQ, though this effect was marginally significant (β = 0.162, SE = 0.040, p = .072). The direct effect of resilience on GHQ was significant (β = 0.278, SE = 0.068, p = .006). However, the indirect effect of resilience on GHQ through civic engagement was not significant (β = 0.055, SE = 0.023, p = .113).
In the control condition, resilience marginally predicted civic engagement (β = 0.315, SE = 0.243, p = .052). Civic engagement negatively predicted GHQ (β = -0.251, SE = 0.040, p = .003). The direct effect of resilience on GHQ was strong and positive (β = 0.617, SE = 0.104, p < .001). The indirect effect was not significant (β = -0.079, SE = 0.034, p = .106).
Discussion
This study addressed three key gaps in the literature on PPIs and civic engagement: (1) the effectiveness of short-term, low intensity multicomponent PPIs through positive education; (2) the role of civic engagement in enhancing PPI outcomes; and (3) the extent to which civic engagement mediates the association between PPI components and well-being. Our results demonstrated that an 8-session low intensity positive education programme significantly enhanced several but not all well-being components, outcomes, and civic engagement behaviors. Importantly, we found that civic engagement played a significant mediating role, with an indirect effect where an increase in resilience led to an increase in civic engagement, which then resulted in improved well-being in the intervention group. Conversely, in the control group, an increase in resilience also led to an increase in civic engagement, but this was unexpectedly associated with a decrease in well-being. These findings provide novel insights into the intricate dynamics between PPIs, civic engagement, and well-being.
Our 8-session intervention demonstrated statistically significant improvements across several domains contributing to well-being, including growth mindset related to intelligence, resilience, and prosocialness, as well as well-being outcomes including positive emotions, general health, and reduced insomnia severity. In contrast, improvements in counselling self-efficacy and growth mindset related to personality were observed only at a trend level (p = .056 and p = .098, respectively), and no significant difference was found for gratitude (p = .768). These results address our first research gap by providing empirical evidence for the effectiveness of short-term, low intensity multicomponent PPIs in a university setting. These findings align with recent meta-analyses on PPIs13,30, which have shown the potential effectiveness of such interventions, while extending this understanding to a brief, low intensity format.
The components showing improvements play crucial roles in overall well-being. Growth mindset fosters adaptability and learning21. Resilience aids in managing and handling stress, even when perceived stress levels may be high17. Prosocialness enhances social connections and support49. The improvements in positive emotions and general health directly contribute to subjective well-being, while reduced insomnia supports both physical and mental health50.
Theoretically, the effectiveness of multicomponent interventions aligns with the complex, multifaceted nature of well-being itself. Our multicomponent approach targets several elements simultaneously, potentially creating synergistic effects that enhance overall well-being more effectively than single-component interventions. Importantly, our study is among the first to suggest that this multicomponent approach can be effective even in a short-term, low intensity format. The effectiveness of this brief intervention may be explained by the broaden-and-build theory51, which suggests that positive experiences, even brief ones, can accumulate and lead to lasting changes in well-being52. This theory may help explain why our short-term, multicomponent intervention was able to produce significant effects, as several components could contribute to a cumulative positive impact5,30. Practically, our findings suggest that adopting a brief multicomponent intervention could be effective in yielding significant impacts on well-being, particularly valuable in contexts where time and resources are limited. For outcomes where only trend-level differences were observed, we interpret these findings cautiously and suggest that they warrant further investigations rather than serving as the primary basis for our conclusions.
Our study provides insights into the complex role of civic engagement in PPIs and its mechanisms in influencing well-being outcomes. The programme successfully promoted civic engagement behaviors, and our analyses revealed notable effects on well-being outcomes. Importantly, our moderated mediation models for both positive emotions and general health showed very similar trends and patterns. While civic engagement attitudes showed a trend towards improvement (p = .136), only civic engagement behaviors reached statistical significance, suggesting that additional research may help clarify the nuanced effects of different dimensions of civic engagement. Although not all measures reached significance, the overall pattern of results lends support to the mediating role of civic engagement in linking resilience to improved well-being. Moreover, these results were further validated by supplementary analyses from additional rounds of data collection involving both remote and face-to-face participants (see Supplementary Information for details, offering additional evidence for the observed intervention effects.
Our mediated moderation analyses demonstrated that the mediating effect of civic engagement on well-being could operate in opposite directions for the experimental and waitlist control groups. The experimental group demonstrated a positive correlation between higher levels of civic engagement and enhanced well-being outcomes. This finding is consistent with earlier studies that have identified beneficial connections between civic participation and overall well-being47,48. Specifically, we found that civic engagement mediated the relationship between resilience and well-being measures through a positive indirect path, supporting our hypothesis and aligning with SDT44, which posits that civic engagement activities may satisfy essential psychological requirements - namely autonomy, competence, and relatedness. These activities likely provided opportunities for participants to exercise choice (autonomy), develop skills (competence), and connect with others (relatedness), thereby contributing positively to their well-being.
In contrast, the waitlist control group exhibited an inconsistent relationship, where higher civic engagement could correspond with decreased well-being scores in certain situations. While unexpected, this result appears consistent with recent literature highlighting that civic engagement’s relationship with well-being can vary across contexts, depending on factors such as the type of civic activity, available resources, and circumstances of engagement53. This suggests that the relationship between civic engagement and well-being is complex and may be influenced by contextual factors beyond our current theoretical framework.
When considering interactional dynamics in our mediated moderation model, several potential explanations emerge for the differing roles of civic engagement across conditions. One possibility is that the intervention may have changed how civic engagement interacted with other psychological resources. For instance, in the control group, civic engagement might have competed with limited time and attentional resources that would otherwise support well-being. The negative relationship observed between civic engagement and positive emotions in the control group could reflect a resource allocation interaction, where increased civic activities without supportive structures diverted resources from activities that would otherwise boost positive emotions. Another interactional perspective is that the quality and meaning of civic engagement might differ based on broader psychological context. Our intervention provided frameworks for interpreting civic experiences as personally meaningful and growth-promoting, potentially transforming how these experiences interacted with resilience to influence well-being. These interactional dynamics suggest that the relationship between civic engagement and well-being involves complex conditional processes rather than simple direct effects.
While this finding warrants further investigations, it adds to growing evidence suggesting that civic engagement may have varied effects on well-being. Although this inconsistent or negative effect may seem unusual, it appears to align with mixed findings in the more recent literature. Specifically, this interpretation may be consistent with evidence that civic engagement with frequently encountered issues, such as environmental concerns, can increase stress and anxiety in individuals lacking adequate coping resources54.
Our study focused on university students, a group that typically has higher civic engagement levels developed in their early adulthood55. While past studies have shown positive effects of civic engagement on life outcomes for groups like at-risk youth56, our contrasting results suggest that the impact may vary significantly across populations. Given their typically higher civic engagement levels, university students might face unique challenges when further increasing their civic involvement. This increased sense of civic duty, without proper support, might inadvertently affect well-being negatively. Our findings highlight the potential need for tailored approaches to civic engagement interventions that consider the specific characteristics and contexts of different populations.
Future research could explore how the effects of civic engagement interventions differ across populations with different initial levels of civic engagement. This approach could provide deeper insights into the mechanisms of civic engagement in well-being interventions and help develop more effective, population-specific strategies.
The multicomponent nature of our intervention appears to have transformed the relationship between civic engagement and well-being in the experimental group. This supportive framework likely equipped participants with resources to manage stressors associated with civic involvement, enabling them to derive more positive experiences. This transformation aligns with research on the psychological benefits of helping others57, which may explain the positive effects of civic engagement in the experimental group.
Theoretically, this transformation could be explained by the interaction between various intervention components, allowing participants to reframe civic challenges as opportunities for growth. For instance, the growth mindset component, which showed significant improvement, may also help participants view civic engagement as a path for personal and societal development rather than a burden.
These findings offer preliminary insights into the potential role of civic engagement within well-being interventions for university students. The positive mediation effect observed in the experimental group aligns with existing literature, suggesting that a supportive, multicomponent framework may help students manage stressors and enhance overall well-being. On the other hand, the inconsistent association observed in the waitlist control group cautions us to consider the potential reduced or even adverse impact that may arise when civic engagement is insufficiently supported. While these insights are valuable, they also underscore the need for a more cautious interpretation and further rigorous testing to better understand the conditions under which civic engagement promotes—or detracts from—well-being. Future research should examine the contextual factors and challenges involved in implementing civic engagement initiatives to clarify its complex role.
The limitations of our research highlight areas for future investigations and expansion of this work. More comprehensive long-term assessments are needed to fully understand the durability of the intervention’s effects. Encouragingly, in part of our follow-up study after 6 months, we found that 93% of participants reported having helped someone in the community, indicating a potential lasting effect on civic engagement behaviors and a possible ripple effect of the programme. However, further investigations are still needed to confirm and extend these promising initial results.
While our waitlist control design allowed for practical implementation in educational settings, future studies might consider alternative control group designs (e.g., active control group design) to further validate the intervention effects.
While our current analysis employed established methods for pre-post intervention studies, we acknowledge several methodological considerations for future research. One important direction would be exploring the underlying structure of well-being components using structural equation modeling (SEM). The current lack of consensus regarding the structural model of well-being components presents both a challenge and an opportunity for future research to better understand how different aspects of well-being interact and influence each other in intervention contexts. Moreover, we recognize that applying SEM to analyze multiple outcomes simultaneously would ideally require a larger sample size than that available in our study—a limitation we plan to address in future investigations.
Additionally, while our study included participants from diverse Asia Pacific regions, we did not specifically test for cultural effects. Future studies interested in examining cultural differences could implement more advanced methods such as multilevel modeling with strategically stratified samples from different cultural backgrounds. This could provide valuable insights into how intervention effectiveness might vary across different cultural contexts and help develop more culturally-informed approaches to well-being interventions.
Although our design included participants from diverse backgrounds, we recognize that a fully stratified cross-cultural design was not implemented. Our supplementary round of data collection involved a different mix of cultural backgrounds and delivery modes, yet yielded comparable outcomes to the main study. The observed consistency may indicate that cultural variability did not strongly influence the intervention effects, but this interpretation remains tentative. While we did not adopt a multilevel modeling approach in the main analysis, we conducted post hoc comparisons between multilevel and single-level models and found no indication that accounting for delivery method as a grouping factor substantially improved model fit. As a form of preliminary validation, we also examined a supplementary group that had a different balance of Zoom and face-to-face delivery. The comparable outcome patterns between the two groups may suggest that delivery method did not have a strong influence on intervention effects. However, we acknowledge that this interpretation remains tentative. Future studies employing stratified sampling and multilevel modeling could more rigorously assess the potential influence of cultural background and delivery method on intervention outcomes.
Further research is needed to explore the mechanisms of civic engagement on different contributors of well-being in detail. While our results show mediation effects for resilience, future studies may explore if other factors are also mediated under different conditions.
Our study provides a foundation for developing evidence-based and efficient programmes that can make a meaningful difference in students’ lives, particularly in contexts where students face unique pressures and challenges. Ultimately, this research paves the way for more effective integration of positive psychology and civic engagement initiatives, potentially fostering both individual well-being and broader societal benefits.
Methods
Ethics statement
This study was approved by the Institutional Review Board of Lingnan University. All procedures were conducted in accordance with the Declaration of Helsinki and relevant institutional guidelines. All participants provided informed consent before participating in the study. Personal identifiable information was removed during data collection and analysis to ensure participant anonymity.
Participants
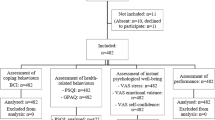
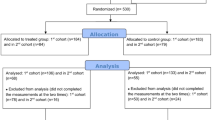
The study involved university students from various institutions. To ensure that our study was adequately powered to detect the hypothesized effects, we conducted an a priori power analysis prior to data collection. Based on prior literature, medium effect sizes for Cohen’s f are typically in the range of 0.25 to 0.30, and we conservatively adopted an estimated effect size of f = 0.27. Given our experimental and waitlist control group design, and setting the significance level at α = 0.05, we used the Python package statsmodels to compute the study’s power. The analysis indicated that a target sample size of approximately 110 participants was required. Recruitment was conducted via email and poster promotion, with participants given the opportunity to join the programme. A total of 112 participants (25 males and 87 females; M = 22.86, SD = 3.58) completed both pre- and post-intervention assessments. All participants were university students. Of these, 63 were local participants randomly assigned to either the experimental group (n = 30) who joined face-to-face sessions or the waitlist control group (n = 33) who did not attend any sessions. Additionally, 49 participants joined remotely from various locations and received the intervention, as logistical constraints prevented implementing a control condition across diverse international settings. The randomization of local participants was conducted using a computer-generated random number sequence. This hybrid approach allowed us to examine the programme’s effectiveness across diverse cultural contexts while providing flexibility in participation methods.
In addition to the primary data collection described above, supplementary data were collected over a three-month period using two distinct formats—one face-to-face and one online (via Zoom)—with the combined analysis of these rounds detailed in the Supplementary Methods, which served to validate the results obtained in the original design. This study aimed to provide a preliminary evaluation of the intervention’s applicability across a diverse student population by including participants from varied cultural backgrounds. However, due to practical constraints common in educational settings, we were not able to achieve a fully balanced or stratified sampling design. Recognizing the challenges of formal cultural stratification, to provide preliminary insights into cultural variability influence on the results, we recruited a supplementary round of data collection involving participants with a different composition of cultural backgrounds and a different balance of delivery modes (Zoom vs. face-to-face) compared to the main sample. The inclusion of this additional group allowed us to assess the consistency of intervention effects across varied participant compositions. Full details are reported in the Supplementary Information.
Programme design
The intervention consisted of 8 weekly sessions of positive education, with each session lasting 90 min. The programme was designed around the central theme of training wellness ambassadors, a key element in enhancing civic engagement among participants. This comprehensive curriculum covered multiple well-being topics including counselling skills, growth mindset, resilience, stress coping strategies, and gratitude, all of which were taught by expert professional psychologists.
The program design was grounded in positive psychology theory and research evidence discussed in our introduction. Each component was specifically chosen based on established research: counselling skills were included to enhance supportive communication28,29; growth mindset activities were based on developmental theories of intelligence and ability21,26; resilience training incorporated evidence-based adaptive coping frameworks17,24; stress coping strategies were derived from established stress management approaches27; and gratitude exercises were based on established gratitude interventions18,25. The wellness ambassador framework was informed by Self-Determination Theory44,45, integrating opportunities for autonomy (through project choice), competence (through skill development), and relatedness (through community engagement). This theoretical integration guided both the content and delivery methods of our multicomponent intervention.
Throughout the programme, participants were required to develop a proposal for promoting the well-being of a specific group in the community that needed support. This project-based approach aimed to practically apply the knowledge gained and further enhance civic engagement. The service proposals were evaluated by professional psychologists, ensuring high standards and practical viability.
The curriculum was structured to equip participants with both theoretical knowledge and practical skills necessary for their role as wellness ambassadors, a method for cultivating civic engagement as mentioned in the literature review. Counselling skills were incorporated as a crucial component to enhance participants’ ability to effectively support others in their communities. Upon satisfactory completion of the programme, participants were issued a certificate as certified wellness ambassadors, further motivating engagement and providing recognition of their acquired skills.
This multifaceted approach not only covered various aspects of well-being but also actively integrated civic engagement elements through the wellness ambassador theme and community-focused project work. The involvement of professional psychologists in both teaching and evaluation ensured the delivery of high-quality, evidence-based contents throughout the programme.
Procedure
The programme was delivered in a hybrid format, with speakers conducting sessions simultaneously for face-to-face and remote participants. Face-to-face participants in the experimental group attended the sessions, while those in the waitlist control group did not participate in any sessions. The waitlist control group was placed on a waitlist and offered the opportunity to participate in the programme after the study period, ensuring ethical considerations were met. Remote participants joined the same sessions online via Zoom, experiencing the programme content in real-time alongside their face-to-face peers. To ensure consistency in the learning experience, we used Zoom’s interactive functions for online participants, including real-time chat, breakout rooms, and other collaborative features.
Measures
We used a comprehensive battery of validated measures to assess various aspects of well-being, civic engagement, and related constructs. Table 4 presents an overview of the instruments used in this study.
Data Availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
World Health Organization. World Mental Health Report: Transforming Mental Health for all (World Health Organization, 2022).
Bolier, L. et al. Positive psychology interventions: A meta-analysis of randomized controlled studies. BMC Public. Health. 13, 119 (2013).
Maddux, J. E. Subjective well-being and Life Satisfaction: An introduction to conceptions, theories, and measures. in Subjective well-being and Life Satisfaction 3–31 (Routledge/Taylor & Francis Group, New York, NY, US, doi:https://doi.org/10.4324/9781351231879-1. (2018).
Shoshani, A. & Steinmetz, S. Positive psychology at school: A School-Based intervention to promote adolescents’ mental health and Well-Being. J. Happiness Stud. 15, 1289–1311 (2014).
Chilver, M. R. & Gatt, J. M. Six-Week online Multi-component positive psychology intervention improves subjective wellbeing in young adults. J. Happiness Stud. 23, 1267–1288 (2022).
Córdova Olivera, P. et al. Academic stress as a predictor of mental health in university students. Cogent Educ. 10, 2232686 (2023).
Shek, D. T. L., Dou, D. & Zhu, X. Prevalence and correlates of mental health of university students in Hong kong: what happened one year after the occurrence of COVID-19? Front Public. Health 10, (2022).
Lun, K. W. et al. Depression and anxiety among university students in Hong Kong. Hong Kong Med. J. 24, 466–472 (2018).
Chen, W. W. & Wong, Y. L. Chinese mindset: theories of intelligence, goal orientation and academic achievement in Hong Kong students. Educational Psychology (2015).
Seligman, M. E. P., Ernst, R. M., Gillham, J., Reivich, K. & Linkins, M. Positive education: positive psychology and classroom interventions. Oxf. Rev. Educ. 35, 293–311 (2009).
Seligman, M. E. P. & Csikszentmihalyi, M. Positive psychology: an introduction. Am. Psychol. 55, 5–14 (2000).
McTiernan, K., Gullon-Scott, F. & Dudley, R. Do positive psychology interventions impact on the subjective wellbeing and depression of clients?? A systematic methodological review. J. Contemp. Psychother. 52, 1–13 (2022).
Sin, N. L. & Lyubomirsky, S. Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: a practice-friendly meta-analysis. J. Clin. Psychol. 65, 467–487 (2009).
Waters, L. A. Review of School-Based positive psychology interventions. Australian Educational Dev. Psychol. 28, 75–90 (2011).
Cohn, M. A., Fredrickson, B. L., Brown, S. L., Mikels, J. A. & Conway, A. M. Happiness unpacked: Positive emotions increase life satisfaction by Building resilience. Emotion 9, 361–368 (2009).
DeRosier, M. E., Frank, E., Schwartz, V. & Leary, K. A. The potential role of resilience education for preventing mental health problems for college students. Psychiatric Annals. 43, 538–544 (2013).
Joyce, S. et al. Road to resilience: A systematic review and meta-analysis of resilience training programmes and interventions. BMJ Open. 8, e017858 (2018).
Emmons, R. A. & Mishra, A. Why gratitude enhances well-being: What we know, what we need to know. Designing Posit. Psychology: Tak. Stock Mov. Forw. 248, 262 (2011).
Jackowska, M., Brown, J., Ronaldson, A. & Steptoe, A. The impact of a brief gratitude intervention on subjective well-being, biology and sleep. J. Health Psychol. 21, 2207–2217 (2016).
Aditomo, A. Students’ response to academic setback: growth mindset as a buffer against demotivation. Int. J. Educational Psychol. 4, 198–222 (2015).
Dweck, C. & Yeager, D. A growth mindset about intelligence. Handbook Wise Interventions: How Social Psychol. Can. Help People Change 9–35 (2020).
Ortiz Alvarado, N. B., Rodríguez Ontiveros, M. & Ayala Gaytán, E. A. Do mindsets shape students’ Well-Being and performance?? J. Psychol. 153, 843–859 (2019).
Milas, G. et al. The impact of stress and coping strategies on life satisfaction in a National sample of adolescents: A structural equation modelling approach. Stress Health. 37, 1026–1034 (2021).
Fletcher, D. & Sarkar, M. Psychological resilience: A review and critique of definitions, concepts, and theory. Eur. Psychol. 18, 12–23 (2013).
Wood, A. M., Froh, J. J. & Geraghty, A. W. Gratitude and well-being: A review and theoretical integration. Clin. Psychol. Rev. 30, 890–905 (2010).
Yeager, D. S. & Dweck, C. S. Mindsets that promote resilience: when students believe that personal characteristics can be developed. Educational Psychol. 47, 302–314 (2012).
Taylor, S. E., Stanton, A. L. & Coping Resources Coping processes, and mental health. Ann. Rev. Clin. Psychol. 3, 377–401 (2007).
Hill, C. E. Helping Skills: Facilitating Exploration, Insight, and Action, 5th Ed. xviii, 485American Psychological Association, Washington, DC, US, (2020). https://doi.org/10.1037/0000147-000
Martin, D. G. & Johnson, E. A. Counseling and Therapy Skills: Fifth Edition (Waveland, 2024).
Hendriks, T., Schotanus-Dijkstra, M., Hassankhan, A., de Jong, J. & Bohlmeijer, E. The efficacy of Multi-component positive psychology interventions: A systematic review and Meta-analysis of randomized controlled trials. J. Happiness Stud. 21, 357–390 (2020).
White, C. A., Uttl, B. & Holder, M. D. Meta-analyses of positive psychology interventions: the effects are much smaller than previously reported. PLoS One. 14, e0216588 (2019).
Yeager, D. S. & Walton, G. M. Social-Psychological interventions in education: they’re not magic. Rev. Educ. Res. 81, 267–301 (2011).
D’Elia, L. et al. A longitudinal study of the Teacch program in different settings: the potential benefits of low intensity intervention in preschool children with autism spectrum disorder. J. Autism Dev. Disord. 44, 615–626 (2014).
Huppert, F. A. A new approach to reducing disorder and improving Well-Being. Perspect. Psychol. Sci. 4, 108–111 (2009).
Wuthrich, V. M. et al. Efficacy of low intensity interventions for geriatric depression and anxiety – A systematic review and meta-analysis. J. Affect. Disord. 344, 592–599 (2024).
Auerbach, R. P. et al. Mental disorders among college students in the world health organization world mental health surveys. Psychol. Med. 46, 2955–2970 (2016).
Auerbach, R. P. et al. WHO world mental health surveys international college student project: prevalence and distribution of mental disorders. J. Abnorm. Psychol. 127, 623 (2018).
Sahu, P. Closure of Universities Due to Coronavirus Disease 2019 (COVID-19): Impact on Education and Mental Health of Students and Academic Staff. Cureus 12, (2020).
Prati, G., Mazzoni, D., Guarino, A., Albanesi, C. & Cicognani, E. Evaluation of an active citizenship intervention based on Youth-Led participatory action research. Health Educ. Behav. 47, 894–904 (2020).
Diener, E., Napa Scollon, C. & Lucas, R. E. The evolving concept of subjective Well-Being: the multifaceted nature of happiness. in Assessing Well-Being (ed Diener, E.) vol. 39 67–100 (Springer Netherlands, Dordrecht, (2009).
Komase, Y. et al. Effects of gratitude intervention on mental health and well-being among workers: A systematic review. J. Occup. Health. 63, e12290 (2021).
Gander, F., Proyer, R. T. & Ruch, W. Positive psychology interventions addressing pleasure, engagement, meaning, positive relationships, and accomplishment increase Well-Being and ameliorate depressive symptoms: A randomized, Placebo-Controlled online study. Front. Psychol. 7, 686 (2016).
Boyd, K. D. & Brackmann, S. Promoting civic engagement to educate institutionally for personal and social responsibility. New. Dir. Student Serv. https://doi.org/10.1002/ss.20021 (2012).
Wray-Lake, L., DeHaan, C. R., Shubert, J. & Ryan, R. M. Examining links from civic engagement to daily well-being from a self-determination theory perspective. J. Posit. Psychol. 14, 166–177 (2019).
Yeung, J. W. K., Zhang, Z. & Kim, T. Y. Volunteering and health benefits in general adults: cumulative effects and forms. BMC Public. Health. 18, 8 (2017).
Mužík, M., Šerek, J. & Juhová, D. S. The effect of civic engagement on different dimensions of Well-Being in youth: A scoping review. Adolesc. Res. Rev. https://doi.org/10.1007/s40894-024-00239-x (2024).
Ballard, P. J., Hoyt, L. T. & Pachucki, M. C. Impacts of adolescent and young adult civic engagement on health and socioeconomic status in adulthood. Child. Dev. 90, 1138–1154 (2019).
Wray-Lake, L., Shubert, J., Lin, L. & Starr, L. R. Examining associations between civic engagement and depressive symptoms from adolescence to young adulthood in a National U.S. Sample. Appl. Dev. Sci. 23, 119–131 (2019).
Caprara, G. V., Steca, P., Zelli, A. & Capanna, C. A new scale for measuring adults’ prosocialness. Eur. J. Psychol. Assess. 21, 77–89 (2005).
Pilcher, J. J., Ginter, D. R. & Sadowsky, B. Sleep quality versus sleep quantity: Relationships between sleep and measures of health, well-being and sleepiness in college students. J. Psychosom. Res. 42, 583–596 (1997).
Fredrickson, B. L. The role of positive emotions in positive psychology: the broaden-and-build theory of positive emotions. Am. Psychol. 56, 218–226 (2001).
Conway, A. M., Tugade, M. M., Catalino, L. I. & Fredrickson, B. L. The Broaden-and-Build Theory of Positive Emotions: Form, Function, and Mechanisms. in Oxford Handbook of Happiness (eds. Boniwell, I., David, S. A. & Ayers, A. C.) 0Oxford University Press, (2013). https://doi.org/10.1093/oxfordhb/9780199557257.013.0003
Fenn, N. et al. A qualitative investigation of civic engagement and Well-Being among Non-College-Bound young adults. Youth 4, 905–930 (2024).
Anneser, E., Levine, P., Lane, K. J. & Corlin, L. Climate stress and anxiety, environmental context, and civic engagement: A nationally representative study. J. Environ. Psychol. 93, 102220 (2024).
Finlay, A., Wray-Lake, L. & Flanagan, C. Civic engagement during the transition to adulthood: Developmental opportunities and social policies at a critical juncture. in Handbook of research on civic engagement in youth 277–305 (John Wiley & Sons, Inc., Hoboken, NJ, US, (2010). https://doi.org/10.1002/9780470767603.ch11
Chan, W. Y., Ou, S. R. & Reynolds, A. Adolescent civic engagement and adult outcomes: an examination among urban Racial minorities. J. Youth Adolesc. 43, 1829–1843 (2014).
Weinstein, N. & Ryan, R. M. When helping helps: autonomous motivation for prosocial behavior and its influence on well-being for the helper and recipient. J. Personal. Soc. Psychol. 98, 222–244 (2010).
McCullough, M. E., Emmons, R. A. & Tsang, J. A. The grateful disposition: A conceptual and empirical topography. J. Personal. Soc. Psychol. 82, 112–127 (2002).
Melchert, T. P., Hays, V. L., Wiljanen, L. M. & Kolocek, A. K. Testing models of counselor development with a measure of counseling self-efficacy. J. Couns. Dev. 74, 640–644 (1996).
Doolittle, A. & Faul, A. C. Civic engagement scale: A validation study. SAGE Open 3, (2013).
Siu, O., Spector, P. E., Cooper, C. L. & Lu, C. Work stress, self-efficacy, Chinese work values, and work well-being in Hong Kong and Beijing. Int. J. Stress Manage. 12, 274–288 (2005).
Siu, O. L., Cheung, F. & Lui, S. Linking positive emotions to work well-being and turnover intention among Hong Kong Police officers: the role of psychological capital. J. Happiness Studies: Interdisciplinary Forum Subjective Well-Being. 16, 367–380 (2015).
Goldberg, D. A User’s Guide To the General Health Questionnaire (NFER-NELSON, 1988).
Dweck, C. S. Mindset: The New Psychology of Success. x, 276Random House, New York, NY, US, (2006).
Siu, O. L. et al. A study of resiliency among Chinese health care workers: capacity to Cope with workplace stress. J. Res. Pers. 43, 770–776 (2009).
Carver, C. S. You want to measure coping but your protocol’s too long: consider the brief COPE. Int. J. Behav. Med. 4, 92–100 (1997).
Morin, C. M., Belleville, G., Bélanger, L. & Ivers, H. The insomnia severity index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 34, 601–608 (2011).
Acknowledgements
We would like to thank Jenny Wong for her support with data collection, logistics, data processing, and for contributing to the initial drafting of this manuscript. We also extend our gratitude to Leiyi Rao (Luna), Xiaonai Li, and Cheuk Hei Wong (Tony) for their support with data collection, logistics, data processing, and for providing valuable insights during the preparation of this manuscript.
Funding
This work was supported by Wofoo Social Enterprise for the Wofoo Joseph Lee Consulting and Counselling Psychology Research Centre at Lingnan University and by The University Grants Committee of Hong Kong under the Research Matching Grant Scheme [Cycle 1, 2019].
Author information
Authors and Affiliations
Contributions
T.Y.N. performed conceptualization, data curation, formal analysis, investigation, methodology, and wrote the original draft. T.K.N. contributed to conceptualization and methodology. O.L.S. contributed to conceptualization, funding acquisition, investigation, project administration, and supervision. All authors reviewed and edited the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ng, T.Y., Ng, T.K. & Siu, O.L. Enhancing mental well-being in university students through multicomponent low intensity positive education and the mediating role of civic engagement. Sci Rep 15, 20871 (2025). https://doi.org/10.1038/s41598-025-05960-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-05960-8
