
Abstract
Environmental factors have known to cause lung cancer. However, the relationship between lung cancer and the environmental factors are not well explored or quantified. Using Zhejiang Province of China as a case study, the spatiotemporal distribution of lung cancer and associated environmental factors were investigated. The data of lung cancer were obtained from Zhejiang Cancer Registry Annual Report and China Cancer Registry Annual Report from 2000 to 2022. The environmental factors are derived from China County Statistical Yearbook and so on. The JoinPoint, SaTScan, spatial autocorrelation technologies and spatial regression models were used to investigate the spatiotemporal clustering, spatial distribution characteristics analysis and correlation of environmental factors of lung cancer. The incidences of lung cancer in Zhejiang Province increased over time, most incidences occurred in the north and became less so in the south of the province, showing a spatial aggregation distribution. The increase of urbanization rate has increased the incidence of lung cancer, and the proportion of environment-related lung adenocarcinoma has increased year by year. The spatial regression model showed that the incidence of lung cancer was negatively correlated with vegetation index, and positively correlated with annual average per capita GDP. There was spatial heterogeneity in the distribution of lung cancer incidence in Zhejiang Province, China, and the areas with high incidence were located in areas with high degree of industrialization and urbanization. Vegetation and urbanization rate have an impact on the incidence of lung cancer.
Similar content being viewed by others
Introduction
Lung cancer is one of the malignant tumors with the highest morbidity and mortality rates in the world, seriously endangering human health1. Global Cancer Epidemiology Statistics (GLOBOCAN) showed that in 2020, there were about 2.2 million new cases of lung cancer worldwide and about 1.8 million cases of lung cancer deaths, accounting for 11.4% and 18.0% of all new cases of malignant tumors and cancer-related deaths, respectively2,3. It is predicted that the annual number of lung cancer deaths worldwide will reach 3 million by 20354. As the country with the second largest population in the world, China faces unprecedented challenges in the prevention and treatment of lung cancer. Over the past 10 years, with the aging of the population and the popularization of lung cancer screening across the country, the incidence of lung cancer in the Chinese population has been on a slow rise3,5,6. GLOBOCAN showed that in 2022, there were about 871,000 new cases of lung cancer in China and about 767,000 cases of lung cancer death, accounting for 18.1% and 23.9% of all malignant tumor cases and cancer-related deaths, respectively7.
A large number of studies have confirmed that smoking is the main risk factor for lung cancer8,9. A study from the UK Biobank found that both intrauterine tobacco exposure and post-birth smoking increased the risk of lung cancer10. Chronic comorbidity is also a risk factor for lung cancer. He et al.11 and Choi et al.12 reported that patients with immune-related diseases had an increased risk of developing lung cancer. Wei et al.13found that a high neuroticism score was associated with an increased risk of lung cancer. Cowdery et al.14confirmed that depressive symptoms are a risk factor for lung cancer. Moreover, outdoor air pollution causes millions of deaths worldwide each year, of which more than 500,000 are due to lung cancer15. Indoor solid fuel16. and outdoor PM2.5 exposure17have also been shown to increase the risk of death from lung cancer. In addition, lack of physical activity and poor sleep18and an unhealthy diet19are also risk factors for lung cancer. Ji et al.20found that the inflammatory factor C-reactive protein was associated with an increased risk of lung cancer. The World Health Organization (WHO) estimates that non-smoking lung cancer patients account for 25% of all cases of lung cancer, ranking seventh among the causes of cancer-related death in the world21. Lung cancer is mainly divided into small cell lung cancer and non-small cell lung cancer; the latter mainly includes squamous cell carcinoma and adenocarcinoma. The occurrence of squamous cell carcinoma is closely related to smoking, and adenocarcinoma is mostly related to external factors such as gene mutation and environmental factors22,23,24. In the beginning of the 2000s, the proportion of adenocarcinoma in lung cancer in China was about 30%25. However, with the continuous advancement of urbanization and industrialization, the problem of environmental pollution has become increasingly prominent, and the impact of air pollution on the occurrence and development of lung cancer has become increasingly obvious, the incidence of adenocarcinoma has shown a significant upward trend26.
With the rapid advancement of urbanization, industrialization, and aging, the incidence of lung cancer remains high in Zhejiang Province. Since 2020, the incidence and mortality rate of lung cancer have been the first cancer spectrum in Zhejiang Province for 20 consecutive years27. However, Current research on the relationship between environmental factors and lung cancer is very limited. Identifying high-risk areas and potential causative factors for lung cancer is important to provide a basis for rational interventions and health service policies. Therefore, we collected data on the incidence and mortality of lung cancer in Zhejiang Province from 2000 to 2019, using spatial epidemiological methods, in order to provide scientific evidence for formulating rational intervention measures and health service policies.
Materials and methods
Data collection
The data of lung cancer in Zhejiang Province from 2000 to 2019 are derived from the Annual Report of Zhejiang Cancer Registry from 2000 to 2022 and the Annual report of China Cancer Registry.The PM2.5 data comes from 0.01°x 0.01° resolution PM2.5 data shared by the Atmospheric Composition Analysis Group at the University of Washington.
The vegetation index is from NASA
MOD13A3 set (https://search.earthdata.nasa.gov/search).Social and economic data come from Zhejiang Statistical Yearbook and China County Statistical Yearbook.
The three-year average values of GDP, per capita GDP, economic density, population density, total grain production in each county, number of industrial enterprises per km2,used as explanatory variables.
Statistical analysis
JoinPoint analysis
Modeling was performed by the grid search method (GSM), and the model was optimized by the Monte Carlo permutation test. The annual percent change (APC) and average annual percent change (AAPC) for lung cancer incidence and mortality were calculated28,29.
Spatiotemporal scan statistics
The incidence and mortality of lung cancer were detected by spatiotemporal clustering using spatiotemporal scanning statistics. Given that the minimum temporal resolution of the data was yearly, the scanning parameters were set as follows: the time range was 2014–2016, with the time window constrained to a 1-year interval in the analysis; the retrospective analysis adopted spatiotemporal scanning as the index; the statistical selection of discrete scanning was based on a Poisson model; the maximum spatial clustering size was limited to 50% of the potential risk population; and the Monte Carlo simulation was restricted to 999 times.
where n is the number of lung cancer and death cases in the scan window, N is the total number of lung cancer and death cases in the population, and E is the expected number of lung cancer and death cases under the null hypothesis. If the null hypothesis is true, I = 1 when the scan window has more lung cancer and death cases than expected; otherwise, I = 0.
Spatial autocorrelation analysis
Anselin’s local Moran’s I coefficient was used to detect the “hotspots” of tumor monitoring sites, so that the type of spatial clusters with high or low incidence of monitoring sites could be determined: The global Moran’s I coefficient (1) and the local Moran’s I coefficient (2) were calculated as follows:
where n is the number of geographical units, \(\:{w}_{ij}\) is the spatial weight coefficient of regions i and j, the conceptualization of the spatial relationship was based on inverse distance weights, \(\:{d}_{ij}\) is the distance between regions i and j, \(\:\delta\:\) is the bandwidth, \(\:{x}_{i}\) and \(\:{x}_{j}\) are the incidence or mortality of lung cancer in regions i and j, respectively, and \(\:\overline{x}\) is the average incidence or mortality of lung cancer in all geographical units.
Spatial regression analysis
Spatial regression analysis can fully consider the autocorrelation and heterogeneity of spatial data and can better utilize and analyze its spatial characteristics. The general form of the global regression model is as follows :30
Based on whether the residuals were independent and whether the Lagrange multiplier (LM) and the robust Lagrange multiplier (R-LM) were statistically significant and based on other indicators such as R2we evaluated the submodel’s Akaike information criterion (AIC), Schwarz criterion (SC), and maximum log-likelihood (LIK) to determine the type of submodel31,32.
Sensitive analyses
To further investigate the impact of different weighting methods on the spatial autocorrelation and spatial regression results of lung cancer incidence and mortality rates in this study, the following sensitivity analyses were conducted using R language, and the specific formulas are shown in the attachment:
-
(1)
Adjust the power parameter (Power = 1–3) and bandwidth (bandwidth = 100 km, 150 km) of the inverse distance weighting;
-
(2)
Construct a spatial weight matrix using the K-Nearest Neighbors (KNN) method. Based on the 14 study sites in this research, the approximate number of nearest neighbors (K) was calculated using the empirical formula, yielding K ≈ 3 or 4. Thus, results for K = 3 and K = 4 were compared;
-
(3)
Construct a spatial weight matrix using the Gaussian kernel density method, with bandwidths consistent with those of IDW (bandwidth = 100 km, 150 km).
-
(4)
Replace the aforementioned spatial weight matrices in the spatial regression analysis to evaluate their effects.
Results
Descriptive statistics of lung cancer
From 2000 to 2019, the total incidence of lung cancer in men, women, and both sexes in Zhejiang Province, China, showed an increasing trend; the total incidence of lung cancer increased 168% from 40.59 per 100,000 in 2000 to 108.75 per 100,000 in 2019. Among them, the incidence of lung cancer in males increased 110% from 59.00 per 100,000 in 2000 to 123.72 per 100,000 in 2019, and in females, it increased 340% from 21.34 per 100,000 in 2000 to 93.89 per 100,000 in 2019. The incidence in males was significantly higher than that in females. At the same time, from 2000 to 2019, the total lung cancer mortality rate of men, women, and both sexes in Zhejiang Province, China, also showed an increasing trend, with the total lung cancer mortality rate of men and women rising from 35.11 per 100,000 in 2000 to 52.31 per 100,000 in 2019. Among them, the total lung cancer mortality rate of men increased from 49.86 per 100,000 in 2000 to 75.68 per 100,000 in 2019, and in women, it increased from 19.67 per 100,000 in 2000 to 29.10 per 100,000 in 2019. The mortality rate was significantly higher for males than for females.
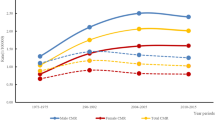
The main types of lung cancer in Zhejiang Province are adenocarcinoma, squamous cell carcinoma, and large cell lung carcinoma. Among them, lung adenocarcinoma ranks first, with its proportion rising year by year, from 43.52% in 2012 to 73.75% in 2019.
Time trends in lung cancer
JoinPoint analysis showed that during 2000–2019, the incidence of lung cancer in Zhejiang Province has an inflection point in 2014, and the APC (95%CI) corresponding to the two intervals was APC2000 − 2014 = 3.72 (95%CI 2.95–4.50, P < 0.001) and APC2014 − 2019 = 10.16 (95%CI 6.31–14.16, P < 0.001), and global AAPC2000 − 2019 =5.38 (95%CI 4.33–6.44, P < 0.001) (Table 1). There was no inflection point in the incidence of lung cancer in males in Zhejiang Province from 2000 to 2019 (AAPC2000 − 2019 = 3.76, 95%CI 3.20–4.32, P < 0.001), with an average annual increase of 3.76%. From 2000 to 2019, the incidence of lung cancer in females in Zhejiang Province showed an inflection point in 2014, and the APC (95%CI) corresponding to the two intervals was APC2000 − 2014 = 5.45 (95%CI 4.34–6.57, P < 0.001) and APC2014 − 2019 = 16.76 (95%CI 11.01–22.81, P < 0.001), and global AAPC2000 − 2019 = 8.32 (95%CI 6.79–9.86, P < 0.001), with an average annual increase of 8.32% .
During 2000–2019, the mortality rate of lung cancer in Zhejiang Province showed three inflection point in 2003, 2006 and 2014, and the APC values corresponding to the three intervals were APC2000 − 2003 = 0.69 (95%CI −2.77 to 4.27, P = 0.667), APC2003 − 2006 = 7.58 (95%CI 0.32–15.37, P = 0.042), APC2006 − 2014 = 3.01 (95%CI 2.05–3.97, P < 0.001) and APC2014 − 2019 = − 1.45 (95%CI −2.97 to 0.11, P = 0.064). The global AAPC (AAPC2000 − 2019 = 2.15, 95%CI 0.96–3.36, P < 0.001) indicates that the average annual increase of lung cancer mortality in Zhejiang Province during 2000–2019 was 2.15%. The mortality rate of male lung cancer in Zhejiang Province from 2000 to 2019 showed an inflection point in 2010, with an average annual increase of 3.11%. The mortality rate of female lung cancer in Zhejiang Province from 2000 to 2019 showed three inflection point in 2002, 2006, and 2012, with an average annual increase of 2.36%.
Spatial scanning of lung cancer at tumor monitoring sites in Zhejiang Province
The SaTScan spatial analysis of the incidence of lung cancer in Zhejiang Province from 2014 to 2016 showed that one cluster with high incidence and one cluster with low incidence were found in the study area (Fig. 1). The primary cluster area with high incidence (LLR = 45.40, RR = 1.30, P < 0.001) was located in northern Zhejiang, covering Daishan, Cixi, Yinzhou, Shangyu, and Jiashan with a radius of 138.38 km. Among them, 1795 observed cases and 1457 expected cases were reported. The primary cluster area with low incidence (LLR = 33.58, RR = 0.70, P < 0.001) was located in southern Zhejiang, covering Lucheng and Xianju, with 503 observed cases and 700 expected cases (Table 2).

Spatial clustering map of lung cancer incidence in Zhejiang Province, China, from 2014 to 2016.
Spatial autocorrelation analysis
Spatial autocorrelation analysis of morbidity
Table 3 Showed the results of Moran’s I global spatial autocorrelation analysis. The average incidence of lung cancer in monitoring sites in Zhejiang Province, China, during 2014–2016 showed spatial autocorrelation (Moran’s I = 0.373, P = 0.013), indicating that the average incidence of lung cancer in the monitoring area was spatially positive. It was statistically significant in both males and females (male Moran’s I = 0.294, P = 0.026; female Moran’s I = 0.355, P = 0.008) .
Univariate LISA local spatial autocorrelation analysis: Local hotspots of the average incidence of lung cancer were observed from the the LISA results in Zhejiang Province, China, from 2014 to 2016. The overall average incidence was statistically significant at monitoring sites. The LISA results of the average incidence of male lung cancer were statistically significant at monitoring sites, and the LISA results of the average incidence of female lung cancer were statistically significant at monitoring sites. The average incidence of lung cancer showed two clusters, which were high-high and low-low. The high-high cluster of the incidences was located in Cixi, Shangyu of Shaoxing, Ningbo, and Daishan of Zhoushan, and the low-low cluster of which was located in Yongkang and Lucheng of Wenzhou. The average incidence of male lung cancer occurred at both high-high and low-low clusters, and the high-high cluster area was located in Jiaxing, Cixi, Shangyu of Shaoxing, and Ningbo. Whereas the low-low cluster area is located in Yongkang and Lucheng of Wenzhou. The average incidence of female lung cancer also showed high-high and low-low clusters. The high-high cluster of female lung cancer was located in Cixi, Ningbo, and Daishan of Zhoushan; and the low-low cluster of female lung cancer was located in Yongkang and Lucheng of Wenzhou.
Spatial autocorrelation analysis of mortality
Moran’s I global spatial autocorrelation analysis. showed that there was no spatial autocorrelation in the three-year overall mean lung cancer mortality at the monitoring sites during 2014–2016 (Moran’s I = 0.175, P = 0.091). After gender stratification, there was no spatial autocorrelation in the mean lung cancer mortality of males (Moran’s I = 0.133, P = 0.108). The mean mortality rate of female lung cancer was spatially positive (Moran’s I = 0.292, P = 0.026) (Table 4).
The LISA results of the average mortality of lung cancer in Zhejiang Province from 2014 to 2016 displayed local hotspots and clusters. The overall average mortality rate of lung cancer was statistically significant at monitoring points; the LISA result of the average mortality rate of male lung cancer was statistically significant at monitoring sites and was consistent with the distribution of the overall average incidence; the LISA result of the average mortality rate of female lung cancer was statistically significant at monitoring sites. The average mortality rate of lung cancer showed three clusters, which were high-high, high-low, and low-high. The high-high cluster was located in Cixi and Shangyu of Shaoxing, high-low cluster was located in Yongkang, and low-high cluster was located in Ningbo. The average mortality rate of male lung cancer showed three clusters, which were high-high, high-low, and low-high. The high-high cluster was located in Cixi and Shangyu of Shaoxing, high-low cluster was located in Yongkang, and low-high cluster was located in Ningbo. The average mortality rate of female lung cancer showed three clusters, high-high, low-high, and low-low. The high-high cluster was located in Cixi and Shangyu of Shaoxing, low-high cluster was located in Ningbo, and low-low cluster was located in Yongkang.
Spatial regression analysis
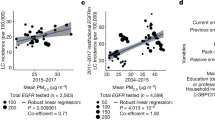
The spatial regression analysis showed that the average incidence of male lung cancer was negatively correlated with the number of beds in medical institutions per 10,000 people (β = −0.347, P = 0.021) and the number of doctors per 10,000 people (β = − 0.865, P = 0.018), with no correlation with the other variables (Table 5). The average mortality rate of male lung cancer was negatively correlated with the number of beds in medical institutions per 10,000 people (β = −0.238, P = 0.030) and the number of doctors per 10,000 people (β = − 0.596, P = 0.025) but was not correlated with the other variables (Table 6). The average incidence of female lung cancer was significantly correlated with NDVI (β = −163.485, P = 0.037) and GDP per capita (β = 4.002, P = 0.035), indicating that the average incidence of female lung cancer was negatively correlated with NDVI and positively correlated with annual average GDP per capita. The mortality of female lung cancer was significantly correlated with NDVI (β = − 58.979, P = 0.006), indicating that the mean mortality of female lung cancer was negatively correlated with NDVI. Total lung cancer incidence and mortality were not significantly associated with all included variables at the 0.05 level.
Sensitive analyses
The sensitivity analysis results of spatial autocorrelation show that. Among the results for men, When the IDW method has Power = 1 and Bandwidth = 100 km (Moran’s I = 0.439, P = 0.006), The KNN method shows stronger spatial autocorrelation when K = 4 (Moran’s I = 0.388, P < 0.001) and the Kernel method shows stronger spatial autocorrelation when Bandwidth = 100 km (Moran’s I = 0.456, P = 0.004). Among the outcomes for women, When the IDW method has Power = 3 and Bandwidth = 150 km (Moran’s I = 0.421, P = 0.004), The KNN method shows stronger spatial autocorrelation when K = 3 (Moran’s I = 0.379, P = 0.001) and the Kernel method shows stronger spatial autocorrelation when Bandwidth = 128.5835 km (Moran’s I = 0.360, P = 0.002). In the results of the total population, when the IDW method had Power = 3 and Bandwidth = 150 km (Moran’s I = 0.466, P = 0.003), The KNN method shows stronger spatial autocorrelation when K = 3 (Moran’s I = 0.435, P = 0.001) and the Kernel method shows stronger spatial autocorrelation when Bandwidth = 100 km (Moran’s I = 0.447, P = 0.003).
The same analysis was conducted on the mortality rate. It is observed that the construction methods of different spatial weight matrices have a certain influence on the spatial autocorrelation results of the incidence rate. In the results of men and the total population, The significance of the results of spatial autocorrelation is inconsistent. This might be because as the power increases, the distance attenuation effect intensifies, and the weights of distant neighbors are significantly weakened. Introducing more long-distance regions as neighbors may dilute the local spatial correlation. However, as the bandwidth further expands, some medium-distance similar regions may be included to restore some spatialautocorrelation. However, the results for women were relatively uniform, possibly because the spatial heterogeneity of lung cancer mortality rate among women was stronger, which was consistent with the original conclusion.
Discussion
At present, it is recognized that lung cancer is the number one malignant tumor threatening human health, with the highest incidence and mortality rates in the world, accounting for 21.3% of the global incidence of cancer33. The incidence of lung cancer in Zhejiang Province, China, showed a significant upward trend from 2000 to 201934,35,36, increasing from 40.59 per 100,000 in 2000 to 108.75 per 100,000 in 2019, and the incidence in males was significantly higher than that in females37,38. At the same time, the mortality rate of lung cancer in Zhejiang Province, China, rising from 35.11 per 100,000 in 2000 to 52.31 per 100,000 in 2019. The age-specific incidence and mortality of lung cancer are at a low level before the age of 40 and then increase rapidly. Morbidity and mortality peaked in patients aged over 80 years in both urban and rural areas39 and were higher in males than in females40. The effect of air pollution on the occurrence and development of lung cancer is becoming increasingly obvious. Studies have shown that the proportion of lung adenocarcinoma has increased year by year, while the proportion of lung squamous cell carcinoma has not changed significantly. According to WHO statistics, adenocarcinoma has been the most common histological type of lung cancer worldwide since 200441.
Although smoking is one of the main risk factors for lung cancer2,42,43, in-depth studies have found that exposure to environmental tobacco smoke has gradually increased among non-smoking people (also known as passive smoking). The number of lung cancer cases in this group is increasing year by year15. According to estimates of the WHO, non-smoking lung cancer patients account for 25% of all lung cancer cases, ranking seventh in the cause of cancer-related death in the world21. In 2013, the WHO for the first time identified PM2.5 as carcinogenic and considered it as a common and major environmental carcinogen44. The damage to the lungs caused by air pollution cannot be underestimated, and any burning matter will produce particulate matter, including PM2.5. PM2.5 in the atmosphere can directly enter the lungs, causing damage45. The lungs play an important role in blood circulation. The blood obtains oxygen and expels carbon dioxide through the lungs, and PM2.5 is disseminated throughout the body along with the blood. The harmful substances attached to the surface of PM2.5, including some polycyclic aromatic hydrocarbons, are strong carcinogens. A cohort study by the American Cancer Society showed that the risk of death begins to increase if atmospheric concentrations of PM2.5 are greater than 10 µg/m3 for a long period of time. For every 10 µg/m3 increase in concentration, the overall risk of death increases by 4%, and the risk of death from lung cancer increases by 8%46 The Canadian Census Health and Environment Cohort (CanCHEC) study, in which subjects were followed-up with for 20 years and assigned to regions across Canada based on space weather classification types, found that exposure to PM2.5 was associated with an increased risk of lung cancer death47.
The spatial and temporal distribution characteristics and spatial variability of lung cancer incidence and mortality at the county (district) level in Zhejiang Province, China illustrated that the environmental factors such as smoking, PM2.5 and urban green covers affect the trend of lung cancer. Therefore, change of these environmental factors could potentially reduce the incidences of lung cancer although the effects of the disease can be complex. In these clusters, Hangzhou, Huzhou, Jiaxing, and Ningbo belong to the eastern region of Zhejiang Province, China. Research shows that the incidence and mortality of lung cancer in the eastern region are higher than those in the central and western regions48, and the economic development of the eastern region of Zhejiang Province is better than that of the central and western regions. The study found that the incidence and mortality of lung cancer were associated with socioeconomic status. Population aging, family income, and access to treatment and diagnosis are also reasons for the significant increase in lung cancer incidence26. Similarly, the imbalance in the level of economic development in different regions of Zhejiang Province may also lead to spatial differences in the incidence of lung cancer, and the eastern region is relatively developed economically. However, western Zhejiang is a low-incidence cluster, while eastern Zhejiang is a high-incidence cluster, which may be due to the stronger industrial foundation, higher urbanization level, and higher economic development in eastern Zhejiang. It may also be related to the high industrial infrastructure area near southern Jiangsu Province, China, and the frequent sandstorms. This indicates that the level of economic development and exposure to other risk factors also vary greatly within the same region. It may also be related to the large size of the elderly population, the high degree of aging, and the accelerated aging process37. While economically developed regions have better medical resources, better medical technology, and higher health literacy, they are also associated with more industrial pollution and exposure to risk factors. Lung cancer screening and the promotion of westernized diets may also play a role. Therefore, the areas with high lung cancer incidence and mortality rates are relatively developed.
Clusters with high lung cancer mortality rates basically coincide with clusters with high incidence rates, suggesting that China’s high incidence of lung cancer may be the biggest reason for its high mortality rates. The prognosis of lung cancer patients in China is poor, and the survival rate is lower than that in developed regions such as Europe and the United States. The main reason may be that the number of patients in the early clinical stage is small, the later stage of clinical diagnosis and treatment is not standardized, and the overall medical level of China still lags behind that of developed countries such as Europe and the United States. The population with the highest incidence of lung cancer is the elderly population, and with increasing age, the functions of the body’s vital organs, immunity, and other bodily functions weaken, so the probability of detection of malignant lung cancer tumors is relatively high and the survival rate of patients is low. Therefore, the coverage of early screening of lung cancer should be expanded, and the standardization and homogenization of clinical diagnosis and treatment of lung cancer should be promoted to reduce the mortality rate of lung cancer in China.
In 2019, The General Office of the State Council promulgated the “Healthy China Action - Cancer Prevention and Control Implementation Plan (2019–2020).” In 2021, The General Office of the State Council issued the Key Tasks for Deepening the Reform of the Medical and Health System, and the National Health Commission issued the Notice on Issuing the Action Plan for Improving the Quality of Cancer Diagnosis and Treatment. The introduction of the above-mentioned policies, regulations, and documents aims to improve cancer prevention and control and enhance the prevention service system. We should continue to promote the formulation and improvement of other relevant policies and regulations and conduct timely risk communication to the public to reduce the risk of lung cancer. Some scholars have proposed that the concept of “One Health” and public health service with multisectoral participation should be advocated to slow down and deal with the spread of various diseases in the Chinese population by mobilizing the full cooperation of various disciplines and departments49,50. In addition to health administrations and agencies, other sectors should also be involved in this action51.
In China, as the pressure of lung cancer prevention and follow-up is concentrated in community health service centers, the prevention and control of lung cancer are highly emphasized in the healthcare system. In terms of healthcare services, such as health education, different sectors can provide services for different groups. For example, social organizations can participate in publicity, actively carry out various forms of publicity and education, and popularize scientific knowledge of air pollution prevention and control. Moreover, multisectoral participation can promote intersectoral cooperation, thereby improving the efficiency of lung cancer prevention and control. The detection and screening of lung cancer patients require large human, financial, and material investments, which cannot be fully guaranteed in the short term if only relying on the actions of health administration departments and institutions. On the contrary, if the National Development and Reform Commission and the financial sector fully play their roles within their respective areas of responsibility and form a cooperative model, they can ensure the timeliness of the input of resources and enable healthcare institutions to carry out screening services more effectively.
Conclusions
The spatial distribution of lung cancer in Zhejiang Province, China, showed significant spatial heterogeneity, and the high-risk clusters of lung cancer incidence and mortality were located in the northeast of Zhejiang Province, China, with a high urbanization rate. Vegetation and urbanization rate have significant effects on the incidence of lung cancer. In the context of accelerated aging, industrialization, and urbanization, lung cancer will still be highly prevalent, and all localities need to formulate prevention and control programs according to local conditions, increase and expand lung cancer screening, and strengthen environmental governance.
Limitations
First, in the present study, we only obtained environmental factors and socioeconomic data at the macro level, which cannot fully represent individual exposure levels, which may affect the results of this study to some extent. Second, cancer is a chronic disease, caused by a variety of factors acting on the human body. There is an incubation period and there are various factors affecting the disease that have not been considered. Third, for the multicollinearity of variables, we analyzed the relationship between lung cancer and environmental factors one by one through a spatial regression model, emphasizing the random association between each factor and lung cancer. Finally, data collection and verification at the national data center are time consuming, and cancer reports usually have a certain delay. In subsequent studies, we will further expand the time and space to provide a more detailed theoretical basis for lung cancer research.
Data availability
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation. Data is provided within the manuscript or supplementary information files.
References
Xiao, J. & Zheng, Y. The global prevalence and prevention progress of lung cancer. China Oncol. 30(10), 721–725. https://doi.org/10.19401/j.cnki.1007-3639.2020.10.001 (2020).
International Agency for Research on Cancer. World cancer report: cancer research for cancer prevention. (2020). https://publications.iarc.fr/586 Accessed 10 July 2021.
Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca-a Cancer J. Clin. 71(3), 209–249. https://doi.org/10.3322/caac.21660 (2021).
Didkowska, J., Wojciechowska, U., Manczuk, M. & Lobaszewski, J. Lung cancer epidemiology: contemporary and future challenges worldwide. Ann. Transl. Med. 4 (8), 150. https://doi.org/10.21037/atm.2016.03.11 (2016).
Zhang, S. et al. Cancer incidence and mortality in china, 2015. J. Natl. Cancer Cent. 1(1), 2–11. https://doi.org/10.1016/j.jncc.2020.12.001 (2021).
Cao, W., Chen, H., Yu, Y., Li, N. & Chen, W. Q. Changing profiles of cancer burden worldwide and in china: A secondary analysis of the global cancer statistics 2020. Chin. Med. J. (Engl) 134(7), 783–791. https://doi.org/10.1097/cm9.0000000000001474 (2021).
Xia, C. et al. Cancer statistics in China and united states, 2022: profiles, trends, and determinants. Chin. Med. J. (Engl) 135(5), 584–590. https://doi.org/10.1097/cm9.0000000000002108 (2022).
Siegel, R. L., Miller, K. D. & Jemal, A. Cancer statistics, 2017. CA Cancer J. Clin. 67(1), 7–30. https://doi.org/10.3322/caac.21387 (2017).
Torre, L. A. et al. Global cancer statistics, 2012. CA Cancer J. Clin. 65(2), 87–108. https://doi.org/10.3322/caac.21262 (2015).
He, H. et al. In utero and childhood/adolescence exposure to tobacco smoke, genetic risk, and lung Cancer incidence and mortality in adulthood. Am. J. Respir Crit. Care Med. 207(2), 173–182. https://doi.org/10.1164/rccm.202112-2758OC (2023).
He, M. et al. Immune-mediated diseases associated with cancer risks. JAMA Oncol. 8(2), 209–219. https://doi.org/10.1001/jamaoncol.2021.5680 (2022).
Choi, H. et al. Non-Cystic fibrosis bronchiectasis increases the risk of lung cancer independent of smoking status. Ann. Am. Thorac. Soc. 19(9), 1551–1560. https://doi.org/10.1513/AnnalsATS.202111-1257OC (2022).
Wei, X. et al. Association between neuroticism and risk of lung cancer: results from observational and Mendelian randomization analyses. Front. Oncol. 12, 836159. https://doi.org/10.3389/fonc.2022.836159 (2022).
Cowdery, S. P. et al. Depressive symptomology and cancer incidence in men and women: longitudinal evidence from the HUNT study. J. Affect. Disord. 316, 1–9. https://doi.org/10.1016/j.jad.2022.08.002 (2022).
Medicalxpress Report: progress in global cancer fight is not only possible, but achievable. https://medicalxpress.com/news/2019-10-global-cancer.html (2019). Accessed 15 February 2021.
Cheng, E. S. et al. Solid fuel, secondhand smoke, and lung cancer mortality: A prospective cohort of 323,794 Chinese Never-Smokers. Am. J. Respir Crit. Care Med. 206(9), 1153–1162. https://doi.org/10.1164/rccm.202201-0114OC (2022).
Wang, X. et al. Histological types of lung cancer attributable to fine particulate, smoking, and genetic susceptibility. Sci. Total Environ. 858(Pt 2), 159890. https://doi.org/10.1016/j.scitotenv.2022.159890 (2023).
Huang, B. H. et al. Sleep and physical activity in relation to all-cause, cardiovascular disease and cancer mortality risk. Br. J. Sports Med. 56(13), 718–724. https://doi.org/10.1136/bjsports-2021-104046 (2022).
Heath, A. K. et al. Diet-wide association study of 92 foods and nutrients and lung cancer risk in the European prospective investigation into cancer and nutrition study and the Netherlands cohort study. Int. J. Cancer 151(11), 1935–1946. https://doi.org/10.1002/ijc.34211 (2022).
Ji, M. et al. Circulating C-reactive protein increases lung cancer risk: results from a prospective cohort of UK biobank. Int. J. Cancer 150(1), 47–55. https://doi.org/10.1002/ijc.33780 (2022).
Thun, M. J. et al. Lung cancer occurrence in never-smokers: An analysis of 13 cohorts and 22 cancer registry studies. PLoS Med. 5(9), e185. https://doi.org/10.1371/journal.pmed.0050185 (2008).
Ringer, G., Smith, M., Engel, A. M., Hendy, M. P. & Lang, J. Influence of sex on lung cancer histology, stage, and survival in a Midwestern United States tumor registry. Clin. Lung Cancer 7(3), 180–182. https://doi.org/10.3816/CLC.2005.n.033 (2005).
Zhi, X. et al. Increased lung cancer mortality rates in the Chinese population from 1973–1975 to 2004–2005: An adverse health effect from exposure to smoking. Cancer 121, 3107–3112. https://doi.org/10.1002/cncr.29603 (2015).
Kinoshita, F. L., Ito, Y. & Nakayama, T. Trends in lung cancer incidence rates by histological type in 1975–2008: A population-based study in Osaka, Japan. J. Epidemiol. 26(11), 579–586. https://doi.org/10.2188/jea.JE20150257 (2016).
Zhejiang Cancer Hospital. The proportion of environment-related lung adenocarcinoma increased by 10% in 20 years. https://m.jianke.com/nrzl/3818871.html (2017). Accessed 02 March 2017.
Han, R., Zheng, R., Zhang, S., Wu, M. & Chen, W. Trend analyses on the differences of lung cancer incidence between gender, area and average age in China during 1989–2008. Chin. J. Lung Cancer 16(9), 445–451. https://doi.org/10.3779/j.issn.1009-3419.2013.09.02 (2013).
Hangzhounet The latest statistics of 14.25 million residents in Zhejiang Province that year died of lung cancer as high as 7857 deaths for 20 consecutive years to top the list of cancer spectrum. (2017). https://baijiahao.baidu.com/s?id=1697513356532143552&wfr=spider&for=pc Accessed 20 May 2021.
Kim, H. J., Fay, M. P., Feuer, E. J. & Midthune, D. N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 19(3), 335–351 (2000).
Kulldorff, M., Heffernan, R., Hartman, J., Assuncao, R. & Mostashari, F. A space-time permutation scan statistic for disease outbreak detection. PLoS Med. 2(3), e59. https://doi.org/10.1371/journal.pmed.0020059 (2005).
Born, B. & Breitung, J. Simple regression-based tests for spatial dependence. Economet. J. 14(2), 330–342. https://doi.org/10.1111/j.1368-423X.2010.00338.x (2011).
Anselin, L. Exploring Spatial data with geodatm: A workbook. USA: Cent. Spatially Integr. Soc. Sci. 198–199. (2005).
Schwartz, G. G. & Hanchette, C. L. UV, latitude, and Spatial trends in prostate cancer mortality: All sunlight is not the same (United States). Cancer Causes Control 17(8), 1091–1101. https://doi.org/10.1007/s10552-006-0050-6 (2006).
Jemal, A. et al. Global cancer statistics. CA Cancer J. Clin. 61(2), 69–90. https://doi.org/10.3322/caac.20107 (2011).
Chen, W. et al. Trend analysis and projection of cancer incidence in China between 1989 and 2008. Chin. J. Oncol. 34(7), 517–524. https://doi.org/10.3760/cma.j.issn.0253-3766.2012.07.010 (2012).
Zeng, H. et al. Trend analysis of cancer mortality in China between 1989 and 2008. Chin. J. Oncol. 34(7), 525–531. https://doi.org/10.3760/cma.j.issn.0253-3766.2012.07.011 (2012).
Xin, W., Huang, L. & Yan, Y. Analysis for the time trends of lung cancer epidemic and disease burden in china, 2005–2013. Chin. J. Cancer Prev. Treat. 26(15), 1059–1065. https://doi.org/10.16073/j.cnki.cjcpt.2019.15.001 (2019).
Zhang, S. et al. Trend analysis on incidence and age at diagnosis for lung cancer in cancer registration areas of china, 2000–2014. Chin. J. Prev. Med. 52(6), 579–585. https://doi.org/10.3760/cma.j.issn.0253-9624.2018.06.005 (2018).
Liang, W. et al. Analysis of trend on mortality of lung cancer and cause-eliminated life expectancy from 1987 to 2017 in Harbin. China Cancer 29(9), 689–694. https://doi.org/10.11735/j.issn.1004-0242.2020.09.A009 (2020).
Manisalidis, I., Stavropoulou, E., Stavropoulos, A. & Bezirtzoglou, E. Environmental and health impacts of air pollution: A review. Front. Public. Health 8, 14. https://doi.org/10.3389/fpubh.2020.00014 (2020).
Wang, Z. & Zheng, Y. Lung cancer worldwide and in China from 1990 to 2020: prevalence and prevention measures. J. Diagn. Concepts Pract. 22(01), 1–7. https://doi.org/10.16150/j.1671-2870.2023.01.001 (2023).
Lortet-Tieulent, J. et al. International trends in lung cancer incidence by histological subtype: Adenocarcinoma stabilizing in men but still increasing in women. Lung Cancer 84(1), 13–22. https://doi.org/10.1016/j.lungcan.2014.01.009 (2014).
Gao, D. & Wang, J. Current status of research on risk factors of lung cancer. Chin. J. Cancer Prev. Treat. 26(21), 1657–1662. https://doi.org/10.16073/j.cnki.cjcpt.2019.21.15 (2019).
Wang, M. et al. Trends in smoking prevalence and implication for chronic diseases in china: Serial national cross-sectional surveys from 2003 to 2013. Lancet Respir Med. 7 (1), 35–45. https://doi.org/10.1016/S2213-2600(18)30432-6 (2019).
International Agency for Research on Cancer. Air pollution and cancer. https://publications.iarc.fr/Book-And-Report-Series/Iarc-Scientific-Publications/Air-Pollution-And-Cancer-2013 (2013). Accessed 05 October 2020.
Guo, H. et al. Trends of cancer incidence among Chinese older adults from 2005 to 2016: A log-linear regression and age-period-cohort analysis. Front. Public. Health. 10, 1023276. https://doi.org/10.3389/fpubh.2022.1023276 (2022).
Pope, C. A. et al. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 287(9), 1132–1141. https://doi.org/10.1001/jama.287.9.1132 (2022).
Cakmak, S. et al. Associations between long-term PM(2.5) and ozone exposure and mortality in the Canadian census health and environment cohort (CANCHEC), by spatial synoptic classification zone. Environ. Int. 111, 200–211. https://doi.org/10.1016/j.envint.2017.11.030 (2018).
Sun, K. et al. Report of cancer incidence and mortality in different areas of china, 2015. China Cancer 28(1), 1–11. https://doi.org/10.11735/j.issn.1004-0242.2019.01.A001 (2019).
Long, Q. et al. Multi-source financing for tuberculosis treatment in china: key issues and challenges. Infect. Dis. Poverty 10(1), 17. https://doi.org/10.1186/s40249-021-00809-4 (2021).
Lonnroth, K. et al. Towards tuberculosis elimination: An action framework for low-incidence countries. Eur. Respir J. 45(4), 928–952. https://doi.org/10.1183/09031936.00214014 (2015).
Holveck, J. C. et al. Prevention, control, and elimination of neglected diseases in the americas: Pathways to integrated, inter-programmatic, inter-sectoral action for health and development. BMC Public. Health 7, 6. https://doi.org/10.1186/1471-2458-7-6 (2007).
Acknowledgements
We want to acknowledge all the investigators for their contributions in the process of collecting data.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Soft Science Project of Ministry of Science and Technology (2011GXQ4D050 and 2007GXS3D086), National Social Science Foundation (07BSH035).
Author information
Authors and Affiliations
Contributions
H.X. conceptualized and designed this study. H.H. and G.L. developed methodologies for data collection and analysis. Y.G. and M.Z. participated in data collection and analysis. Y.G. and H.L. participated in writing and editing. All authors were subsequently involved in critically revising the manuscript. All authors have approved the final version of the manuscript to be published and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
Conflict of InterestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Gao, Y., Zhang, M., Liu, G. et al. Historical data analysis and future prediction of lung cancer in Zhejiang province, China. Sci Rep 15, 21813 (2025). https://doi.org/10.1038/s41598-025-07200-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-07200-5
