
Abstract
Taste and smell disorders (TSDs) can induce diminished interest in food, inadequate nutrient intake, and emotional irregularities, particularly among cancer patients. Previous research found that the main culprits of TSD development in cancer patients are cytotoxic drugs such as taxol, fluorouracil, cyclophosphamide, and anthracycline-based drugs. The advent of targeted drugs such as vascular endothelial growth factor receptor-tyrosine kinase inhibitors (VEGFR-TKIs) has significantly extended the survival time of cancer patients, and thus widely used in clinical practice. However, the association between the use of VEGFR-TKIs and the development of TSDs havs not been studied.The adverse event(AE) reports related to VEGFR-TKIs were downloaded from the FDA Adverse Event Reporting System (FAERS) database. Disproportionality analysis was conducted to assess the correlation between VEGFR-TKIs and TSDs. The Standardized Medical Dictionary for Regulatory Activities (MedDRA) Queries (SMQs) were used to analyze the AEs of TSDs. The study found a statistically significant correlation between the occurrence of TSDs and the use of VEGF-TKIs (cabozantinib, axitinib, pazopanib, sunitinib, nintedanib, and lenvatinib).However, the instructions for Nintedanib, Sorafenib and Lenvatinib were not mentioned. Capbottinib demonstrated the highest number of reports(1790 cases), also with the strongest association (ROR 95%CI-low = 16.51; PRR = 16.18; IC025 = 3.96) when analyzing the narrow SMQ of TSDs. Dysgeusia, taste disorder, and ageusia were the most commonly reported preferred terms (PTs) in VEGFR-TKI-related TSDs, accounting for more than 90% of the reported cases. Cabozantinib showed the highest number of reports and strongest correlation with ageusia, taste disorder, parosmia, and anosmia. The study found significant association between the reports of TSDs and the use of VEGFR-TKIs, indicating the monitoring of TSD development and appropriate management in clinical is necessary.
Similar content being viewed by others

Introduction
Tyrosine kinases represent a class of enzymes that catalyze the phosphorylation of tyrosine residues on various substrate proteins using ATP as a phosphate donor and play pivotal roles in mediating cellular growth, proliferation, and differentiation1. In recent years, there has been a steady increase in the development of drugs that serve as inhibitors of tyrosine kinases, which can effectively disrupt tyrosine kinase activity, thus curtailing cell proliferation2. In particular, vascular endothelial growth factor receptor tyrosine kinase inhibitors (VEGFR-TKIs) include a class of small-molecule drugs targeting VEGFR, by impeding the VEGF signaling pathway to curb vascular proliferation and angiogenesis. Several VEGFR-TKIs were approved by the United States Food and Drug Administration (FDA) for the favorable clinical efficacy in treating a spectrum of solid tumors, including regorafenib, cabozantinib, lenvatinib, axitinib, sunitinib, sorafenib, nintedanib, and pazopanib3. The commonly reported adverse events (AEs) of VEGFR-TKIs include diarrhea, fatigue, hand-foot skin syndrome (PPES), hypertension, hypothyroidism, bleeding, and so on4,5.
Taste and smell disorders (TSDs) are chemosensory disorders that can significantly affect the quality of life for the handicap of food enjoyment and nutrient intake. TSDs are often caused by some underlying diseases, such as diabetes, obesity, and oral diseases6. In cancer patients, TSDs have manifested during treatment with cytotoxic drugs such as paclitaxel, fluorouracil, cyclophosphamide, and anthracycline7. The drug labels of some VEGFR-TKIs have mentioned the AEs of taste, including axitinib, cabozantinib, pazopanib, regorafenib and sunitinib. A disproportionality analysis revealed a significant association between regorafenib and taste disorders8, another study showd taste disorders were reported in 55% of patients treated with regorafenib9. A research reported prevalence of protein kinase inhibitors-induced patient-reported taste alterations. Sunitinib showed a prevalence of patient-reported taste alterations varying from 18 to 63%, while sorafenib varied from 3 to 55%10. However, the AEs of smell have not been reported or documented in the label yet. Besides, we need more real-world statistics from large-scale users to thoroughly discuss the characteristics and the association of the drugs-related AEs. Therefore, the pharmacovigilance study aimed to analyze data from the US FDA Adverse Event Reporting System (FAERS) to identify possible association between VEGFR-TKIs use and the development of TSDs and provide a comprehensive overview of the clinical characteristics and prognosis.
Methods
Data source
Data were obtained from the US Food and Drug Administration Public Data Open Project (Open FDA), which obtained raw data from the FAERS database. Data were extracted by OpenVigil2.1, an open pharmacovigilance data extraction, mining, and analysis tool specifically designed for the FAERS database. OpenVigil2.1 works only on cleaned FDA data, with most duplicates and reports with incomplete information removed.
In the FAERS database, AEs are classified using preferred terms (PTs) from the Medical Dictionary for Regulatory Activities (MedDRA) (version 25.0). A specific PT may be linked with multiple higher-level terms (HLTs), higher-level group terms (HLGTs), and system organ classes (SOCs). Additionally, PTs that indicate symptoms, signs, investigations, or diagnoses of potential significance are organized into Standardized MedDRA Queries (SMQs) to portray specific medical conditions. The research concentrated on the specific SMQ concerning TSDs, including 15 PTs (Table 1).
Data extraction
In the study, the data for each drug from the first quarter of 2006 to the third quarter of 2023 were collected for retrospective analysis in the FAERS database. VEGFR-TKI (axitinib, nintedanib, sorafenib, cabozantinib, regorafenib, pazopanib, sunitinib, and lenvatinib) were identified as primary or secondary suspects in the reports. Prior to analysis, duplicate entries with the same number were deleted and the same information, such as patient demographics, drugs, and AE, were merged, see Figure S1. The association between the narrow-SMQ and PTs of TSDs with VEGFR-TKIs was analyzed .
Data mining
A disproportionality analysis was performed using a case/non-case methodology. The Reporting Odds Ratio (ROR)11 and proportional reporting ratio (PRR)12, were calculated to identify potential reporting disproportionality signals in TSDs related to VEGFR-TKI. An exploratory disproportionality approach comparing ADRs related to VEGFR-TKI versus all other drugs (non-cases) reported in the FAERS database was conducted13. All TSDs with a significant ROR (lower limit of the 95% CI > 1 with at least 3 cases) were carefully considered unexpected if they were not reported in the FDA label at the time of the study. The Bayesian Information Component (IC)14, estimated as significant by the 95% credibility interval > 0 (IC025 > 0), which is more accurate with a low number of reports, was calculated to decrease the risk of detecting false signals15. The equations and criteria for the three algorithms are shown in Table 2.
Statistical analysis
Descriptive analysis was performed to summarize the clinical characteristics of TSDs-related individuals associated with VEGFR-TKIs. The continuous variables was presented as mean ± standard deviation (SD) and frequency variables was expressed as percentages. Pearson’s chi-squared or Fisher’s exact test was used to compare the intervention and hospitalization rates of different VEGFR-TKIs. All statistical analysis were performed with IBM SPSS Statistics (version 26). Results with a P value less than 0.05 were considered statistically significant.
Results
Descriptive analysis
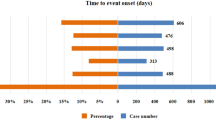
The clinical features of individuals with VEGFR-TKI-related TSDs are presented in Table 3; Fig. 1. The median age was 65.53 ± 10.68 years, with the exception of nintedanib, which was mostly administered for those in the age range of 70–79 years. Males were more likely to be affected by TSDs than females, except for Lenvatinib. The TSDs caused by VEGFR-TKIs were primarily observed in North America, accounting for 81.4% of cases. VEGFR-TKIs-related TSDs were first reported with sorafenib and sunitinib in 2006. Since the launch of cabozantinib in 2012, the reported amount of TSD-related cases had shown a consistent increase, with 1790 cases reported by the third quarter of 2023.

The reporting time of patients with VEGF-TKI related taste and smell disorders.
The indications of each VEGFR-TKIs vary, showing in Table 3. All VEGFR-TKIs were administered orally, and the dosage of most cases were in the range of recommended. Compared with other VEGFR-TKIs mentioned above, individuals taking sorafenib often showed a poorer prognosis, with higher hospitalization and mortality rates. Programmed cell death-1, levothyroxine sodium, and antihypertensive drugs, were the most often co-administered drugs.
Bayesian and nonproportional analysis
From the initial marketing of VEGFR-TKI (2006) to the third quarter of 2023, a total of 13,105,775 cases were documented, including 63,956 cases of TSDs. The narrow SMQ of TSDs related to the VEGFR-TKIs were analyzed showing in Table 4. According to the algorithms, axitinib, nintedanib, cabozantinib, sunitinib, pazopanib, lenvatinib exhibited statistically significant in terms of ROR, PRR and information component (IC). Cabozantinib showed the highest number of cases reported (1790), also with the strongest association with TSDs(ROR 95%CI-low = 16.51; PRR = 16.18; IC025 = 3.96). Regorafenib was the least reported drugs, and there was no statistically difference comparerd with the reference group of the FAERS database for the development of TSDs.
Correlation between VEGF-TKIs and PTs included in the narrow SMQ of TSDs
We also conducted a analysis focused on VEGFR-TKIs with PTs including in the narrow SMQ of TSDs in Fig. 2. Dysgeusia, taste disorder, and ageusia were the most commonly reported preferred terms (PTs) in VEGFR-TKI-related TSDs, accounting for more than 90% of the reported cases. Cabozantinib showed the highest number of reports and strongest correlation with ageusia, taste disorder, parosmia, and anosmia. There was a strong correlation between axitinib, cabozantinib, nintedanib, pazopanib, sorafenib, sunitinib use and the reporting of dysgeusia, sunitinib showed the strongest correlation (ROR95% CI−low = 8.71, PRR = 9.22, IC025 = 3.04). Except for regorafenib, all other VEGFR-TKIs demonstrated statistically significant with ageusia,. Cabozantinib and sunitinib accounted for the largest proportion of cases (62.44%), also showed the highest correlation, with ROR values of 17.89 and 15.05, respectively. For taste disorders, axitinib, cabozantinib, nintedanib, pazopanib, sunitinib, and lenvatinib exhibited statistically correlation. Hypogeusia was significantly correlated with axitinib, cabozantinib, pazopanib, and sunitinib use, among which the correlation between hypogeusia and pazopanib, sunitinib use was higher, with ROR values of 11.10 and 12.41, respectively. .In addition, there were 63 parosmia-related cases, among which axitinib and cabozantinib was strongly correlated with the PT, with ROR values of 2.71 and 3.74, respectively. For anosmia, only cabozantinib showed statistically difference (ROR 95% CI-low = 1.30, PRR = 2.04, IC025 = 0.21).

The Correlation between VEGF-TKI and PTs included in the narrow SMQ of taste and smell disorders.
Discussion
The purpose of the study was to analyze the association between VEGFR-TKIs and the devolopment of TSDs and meanwhile provided a comprehensive overview of the clinical characteristics and prognosis of various drug interventions.To the best of our knowledge, it is first time to conduct such comprehensive analysis base on real-world clinical data to explore the association between TSDs and different VEGFR-TKIs. The study showed that there was statistically significant association between VEGFR-TKIs and the development of TSDs.
In the present study, we observed a gender-based predisposition towards the development of TSDs subsequent to VEGFR-TKIs administration, with males exhibiting a higher likelihood of TSD onset compared to females. This disparity may be correlated with detrimental lifestyle factors, as evidenced by research indicating that smoking and alcohol consumption can lead to the overstimulation of taste buds, a reduction in their sensory acuity, and the impairment of taste nerve conduction, ultimately resulting in gustatory dysfunction16,17,18. The age of the cases was mainly in the range of 60–69 years except for nintedanib, which was in 70–79 years. The reason may be explained by the indication of nintedanib19. Previous literature has indicated the onset age of idiopathic pulmonary fibrosis is often higher than that for renal cancer20,21. Furthermore, our analysis revealed that sorafenib was significantly associated with a poorer prognosis within the cohort of cases treated with VEGFR-TKIs. The association may be attributed to the population receiving sorafenib, as it is predominantly prescribed for hepatocellular carcinoma rather than renal carcinoma. Past studies have shown that liver cancer five year survival rate was significantly higher than that of kidney cancer22,23, which may account for the observed prognostic differences among individuals treated with sorafenib. These findings highlight the importance of considering gender, age and lifestyle factors in the context of VEGFR-TKI-related TSDs, as well as the prognostic implications in specific oncological populations.
Accoding to the latest FDA label, there was no records of the AEs of taste for nintedanib, sorafenib and lenvatinib, while the AEs of smell for all VEGFR-TKIs have not been documented. The study found potential safety signals between the SMQ of TSDs and nintedanib, sorafenib and lenvatinib. Among them, nintedanib demonstrated the highest association (PRR = 4.73, ROR = 4.82, IC = 2.23), and then lenvatinib (PRR = 2.53, ROR = 2.23, IC = 1.11), sorafenib followed (PRR = 1.40,ROR = 1.40,IC = 0.48). For the AEs of smell, cabozantinib showed strong correlation with hyposmia, anosmia and parosmia, axitinib was associated with hyposmia and parosmia, while pazopanib exhibited association with hyposmia.
The mechanism of VEGFR-TKI-related TSDs remain unclear. Oral toxicity, such as oral mucositis and xerostomia is likely to play an important role in taste alterations24. Oral mucositis will damage the epithelial cell membranes and leading to the formation of compounds causing off-flavour taste perceptions10. Xerostomia may hampers the solubilising of food particles and thus decreases the presentation of tastants to the taste receptors25. Taste receptor cells are epithelial cells located on the tongue and epiglottis. Renewal and reconstruction of taste receptor cells are essential to maintaining their functions and ensuring the long-term stability of the taste system26. VEGFR-TKIs may affect the differentiation and proliferation of epithelial cells by inhibiting angiogenesis, and can also affect the migration and proliferation of endothelial cells induced by oral mucosal epithelial cells27. VEGFR-TKIs may influence the reconstruction of taste bud cells by inhibiting the Wnt/β-catenin signaling pathway, of which VEGFR1 is a positive regulator28,29. Apart from angiogenic function, VEGF also acts as a neuronal survival factor, regulating the survival, migration, and proliferation of neurons and glial cells30. VEGF binds to neuropilin-1 (NRP1) in the facial branchiomotor (FBM) cell body and controls FBM migration. Smell epithelial cells play a central role in our olfactory system and are responsible for capturing and transmitting odor information31. Normally, these cells can repair themselves after injury, however, the repair capacity may be weakened as a result of disease or the use of drugs, leading to olfactory dysfunction32,33. The binding of VEGFR1 regulates olfactory bulb neurogenesis34,35. VEGFR-TKIs may inhibit the repair of olfactory epithelial cells after damage by interfering with angiogenesis36,37. And VEGFR-TKIs have multi-target properties, intervening in nerve repair and neuronal regeneration through multiple pathways, thereby affecting self-repair after weakened or damaged olfactory function38.
The study benefits from the analysis of real-world clinical data and data mining techniques, We identified a significant association between reports of TSDs and the use of VEGFR-TKIs, especially we firstly reported the AEs of smell disorders related with a few VEGFR-TKIs, such as cabozantinib, axitinib, nintedanib. However, we also realized there are several limitations. Firstly, our methods were unable to distinguish accurate data from false or inaccurately reported data. Secondly, while we were able to extract statistics from the basic case information, the accuracy of concomitant diseases and medication history was unclear, introducing potential confounding factors and uncertainties into the analysis. Thirdly, data mining using Bayesian and nonproportional analysis can only establish statistical association but not causal relationship between AEs and drugs. The lack of research on VEGFR-TKI-related TSDs makes it challenging to establish a definitive link between the drugs and AEs. Further clinical, anatomical, or imaging studies involving large-scale human populations are necessary to provide more comprehensive explanations.
Data availability
The data supporting the findings of this study were obtained from the following public database OpenVigil 2.1(https://openvigil.sourceforge.net/),[lUser: welcome; Password: world].
References
Mustonen, T. & Alitalo, K. Endothelial receptor tyrosine kinases involved in angiogenesis. J. Cell. Biol. 129 (4), 895–898 (1995).
Goel, S., Mani, S. & Perez-Soler, R. Tyrosine kinase inhibitors: A clinical perspective. Curr. Oncol. Rep. Jan. 4 (1), 9–19 (2002).
Hou, W. et al. Comparative evaluation of cardiovascular risks among nine FDA-approved VEGFR-TKIs in patients with solid tumors: A bayesian network analysis of randomized controlled trials. J. Cancer Res. Clin. Oncol. 147 (8), 2407–2420 (2021).
Liu, B. et al. Incidence and risk of hypertension associated with vascular endothelial growth factor receptor tyrosine kinase inhibitors in cancer patients: A comprehensive network meta-analysis of 72 randomized controlled trials involving 30013 patients. Oncotarget. 11 (41), 67661–67673 (2016).
Funakoshi, T., Latif, A. & Galsky, M. D. Safety and efficacy of addition of VEGFR and EGFR-family oral small-molecule tyrosine kinase inhibitors to cytotoxic chemotherapy in solid cancers: A systematic review and meta-analysis of randomized controlled trials. Cancer Treat. Rev. 40 (5), 636–647 (2014).
Amezaga, J. et al. Assessing taste and smell alterations in cancer patients undergoing chemotherapy according to treatment. Support. Care Cancer Off. J. Multinational Assoc. Support. Care Cancer 26 (12), 4077–4086 (2018).
Buttiron Webber, T., Briata, I. M., DeCensi, A., Cevasco, I. & Paleari, L. Taste and smell disorders in cancer treatment: Results from an integrative rapid systematic review. Int. J. Mol. Sci. 28 ;24(3). (2023).
Barbieri, M. A. et al. Neuropsychiatric adverse drug reactions with oral tyrosine kinase inhibitors in metastatic colorectal cancer: An analysis from the FDA adverse event reporting system. Front. Oncol. 13, 1268672 (2023). Published 2023 Oct 31.
van Elst, J. M. et al. Taste, smell and mouthfeel disturbances in patients with gastrointestinal stromal tumors treated with tyrosine-kinase inhibitors. Support. Care Cancer. 30 (3), 2307–2315 (2022).
van der Werf, A., Rovithi, M., Langius, J. A. E., de van der Schueren, M. A. E. & Verheul, H. M. W. Insight in taste alterations during treatment with protein kinase inhibitors. Eur. J. Cancer. 86, 125–134 (2017).
Sakaeda, T., Tamon, A., Kadoyama, K. & Okuno, Y. Data mining of the public version of the FDA adverse event reporting system. Int. J. Med. Sci. 10 (7), 796–803 (2013).
Slattery, J., Alvarez, Y. & Hidalgo, A. Choosing thresholds for statistical signal detection with the proportional reporting ratio. Drug Saf. 36 (8), 687–692 (2013).
Ji, L. H., Zhao, C. L., Wang, Y. Q. & Fu, Z. H. Bisphosphonates-related tendinopathies and ligament disorders: Cases analysis from the U.S. Food and Drug Administration adverse event reporting system. Bone 177, 116919 (2023).
Hauben, M. & Bate, A. Decision support methods for the detection of adverse events in post-marketing data. Drug Discov. Today. 14 (7–8), 343–357 (2009).
Harpaz, R. et al. Performance of pharmacovigilance signal-detection algorithms for the FDA adverse event reporting system. Clin. Pharmacol. Ther. 93 (6), 539–546 (2013).
Naimi, B. R. et al. Patient insights into the diagnosis of smell and taste disorders in the United States. Preprint medRxiv (2023). 2023.09.20.23295861.
Ajmani, G. S., Suh, H. H., Wroblewski, K. E. & Pinto, J. M. Smoking and olfactory dysfunction: A systematic literature review and meta-analysis. Laryngoscope 127 (8), 1753–1761 (2017).
Agarwal, K., Schaffe-Odeleye, T., Marzouk, M. & Joseph, P. V. Reduced bitter taste and enhanced appetitive odor identification in individuals at risk for alcohol use disorder: National Health and Nutrition Examination Survey (NHANES) 2013–2014. J Stud Alcohol Drugs.
Lamb, Y. N. & Nintedanib A review in Fibrotic interstitial lung diseases. Drugs Apr. 81 (5), 575–586 (2021).
Dudani, S. et al. Evaluation of clear cell, papillary, and chromophobe renal cell carcinoma metastasis sites and association with survival. JAMA Netw. Open. 4 (1), e2021869 (2021).
Zheng, Q. et al. Mortality and survival in idiopathic pulmonary fibrosis: A systematic review and meta-analysis. ERJ Open. Res. 8(1). (2022).
Yilma, M. et al. Survival outcomes among patients with Hepatocellular Carcinoma in a large Integrated US Health System. JAMA Netw. Open. 7 (9), e2435066 (2024).
Rose, T. L. & Kim, W. Y. Renal cell carcinoma: A review. JAMA 332 (12), 1001–1010 (2024).
Boers-Doets, C. B. et al. Oral adverse events associated with tyrosine kinase and mammalian target of rapamycin inhibitors in renal cell carcinoma: A structured literature review. Oncologist 17 (1), 135–144 (2012).
Epstein, J. B. & Barasch, A. Taste disorders in cancer patients: Pathogenesis, and approach to assessment and management. Oral Oncol. 46 (2), 77–81 (2010).
Zheng, X. et al. [Development and homeostasis of taste buds in mammals]. Hua Xi Kou Qiang Yi Xue Za Zhi = Huaxi Kouqiang Yixue Zazhi = West. China J. Stomatol. 1 (5), 552–558 (2018).
Kanayama, S. et al. Analysis of soluble vascular endothelial growth factor receptor-1 secreted from cultured corneal and oral mucosal epithelial cell sheets in vitro. Br. J. Ophthalmol.. 93 (2), 263–267 (2009).
Katoh, Y. & Katoh, M. Comparative integromics on VEGF family members. Int. J. Oncol. 28 (6), 1585–1589 (2006).
Naik, S., Dothager, R. S., Marasa, J., Lewis, C. L. & Piwnica-Worms, D. Vascular endothelial growth factor Receptor-1 is synthetic Lethal to aberrant beta-catenin activation in Colon cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 15 (24), 7529–7537 (2009).
Carmeliet, P. & Ruiz de Almodovar, C. VEGF ligands and receptors: Implications in neurodevelopment and neurodegeneration. Cell. Mol. Life Sci. CMLS. 70 (10), 1763–1778 (2013).
Wang, H., Deng, L. & Qin, X. [Development of an olfactory epithelial organoid culture system based on small molecule screening]. Sheng Wu gong. Cheng Xue bao = Chin. J. Biotechnol.. 25 (1), 318–336 (2023).
Wu, A. P. & Davidson, T. Posttraumatic anosmia secondary to central nervous system injury. Am. J. Rhinol. 22 (6), 606–607 (2008).
Schiffman, S. S. Taste and smell losses in normal aging and disease. Jama 22–29 (16), 1357–1362 (1997).
Jin, K. et al. Vascular endothelial growth factor (VEGF) stimulates neurogenesis in vitro and in vivo. Proc. Natl. Acad. Sci. U. S. A. 3 (18), 11946–11950 (2002).
Wittko, I. M. et al. VEGFR-1 regulates adult olfactory bulb neurogenesis and migration of neural progenitors in the rostral migratory stream in vivo. J. Neurosci. Off. J. Soc. Neurosci.. 8 (27), 8704–8714 (2009).
Mohapel, P., Frielingsdorf, H., Haggblad, J., Zachrisson, O. & Brundin, P. Platelet-derived growth factor (PDGF-BB) and brain-derived neurotrophic factor (BDNF) induce striatal neurogenesis in adult rats with 6-hydroxydopamine lesions. Neuroscience 132 (3), 767–776 (2005).
Beecher, K., Hafner, L. M., Ekberg, J., St John, J. A. & Chehrehasa, F. Combined VEGF/PDGF improves olfactory regeneration after unilateral bulbectomy in mice. Neural Regen. Res. 13 (10), 1820–1826 (2018).
Beites, C. L., Kawauchi, S., Crocker, C. E. & Calof, A. L. Identification and molecular regulation of neural stem cells in the olfactory epithelium. Exp. Cell. Res. 306 (2), 309–316 (2005).
Author information
Authors and Affiliations
Contributions
Zhonghua Fu: Conceptualization, Methodology, Software, Writing-Original draft preparation. Chonglong Zhao, Yaqin Wang, and Lei Zhang Visualization, Investigation, Software. Lei Wang: Data curation, Writing-Reviewing and Editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Fu, Zh., Zhao, C., Wang, Y. et al. Pharmacovigilance imbalance analysis of VEGFR-TKI-related taste and smell disorders. Sci Rep 15, 3118 (2025). https://doi.org/10.1038/s41598-025-87678-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-87678-1
