
Abstract
Understanding the impact of multimorbidity on having less than 20 natural teeth is crucial for safeguarding the oral health of older adults with multimorbidity. This study aimed to analyze the association between multimorbidity and having less than 20 natural teeth in older Chinese adults. The data for this analysis were obtained from the Chinese Longitudinal Healthy Longevity Survey (CLHLS), which covers 23 provinces, municipalities, and autonomous regions throughout China. The survey includes information on dental health (such as dentition status), a variety of chronic conditions, and other sociological characteristics of older adults in China. Having less than 20 natural teeth was used as the dependent variable, with multimorbidity as the independent variable. A multivariable logistic regression model was applied to estimate the association between multimorbidity and having less than 20 natural teeth. A total of 3,640 older adults were included in the study, of whom 58.27% (2121) were identified as having less than 20 natural teeth. The results indicated that factors such as age, education level, exercise, ability to perform daily activities, frequency of brushing teeth, and BMI are associated with having less than 20 natural teeth. Additionally, compared with those without chronic disease, the odds ratio (OR) of having less than 20 natural teeth was 1.32 (95% CI: 1.10, 1.57) for older adults with only one chronic disease, and the OR for those with two or more chronic diseases was 1.418 (95% CI: 1.06, 1.89). This study highlights the importance of monitoring the oral health of older adults with multimorbidity and identifies an association between multimorbidity and having less than 20 natural teeth. Oral health care institutions should implement measures to support the development of more comprehensive public health policies.
Similar content being viewed by others


Introduction
Tooth loss is a significant public health issue influenced by various biological, behavioral, and socioeconomic factors. Among American older adults who underwent dental examinations between 2011 and 2016, 59.9% were found to have fewer than 20 natural teeth1. A survey in Japan revealed that only 28.5% of the older adults retained 20 or more natural teeth2. In Mexico, a study reported that 62.4% of the 2,098 participants had lost at least one tooth3, while another study found that 27% of the sample had no natural teeth remaining4.
The evidence indicates that missing or severely impaired dentition is a common condition. It reduces chewing capacity and hinders nutritional intake5, and impacts facial appearance, communication, social interaction, and mental health6. In 2019, the National Health Commission launched the ‘Healthy Oral Action Plan 2019–2025’, emphasizing the importance of oral health for older adults, particularly those with chronic illnesses, to improve their overall well-being.
Dental caries and periodontal disease are the primary causes of tooth loss. Caries often result from poor oral hygiene and high sugar intake, while periodontal disease involves gum inflammation that weakens the teeth’s supporting structures7,8,9. Tooth loss is also linked to risk factors such as smoking, inadequate oral hygiene, low socioeconomic status, and limited access to preventive dental care3,10,11,12,13,14. Socioeconomic and cultural factors further contribute to this issue, as older adults—particularly those with low income, low education, minority backgrounds, or living in rural areas—face higher risks of tooth loss11,12,14,15.
To better study such issues, ‘having less than 20 natural teeth’ has been established as a key standard for assessing oral health. This measure refers to individuals with fewer than 20 natural teeth remaining, based on the World Health Organization’s ‘8020 Plan’, which highlights the importance of retaining at least 20 teeth for maintaining proper chewing function and overall well-being16. The threshold of 20 natural teeth is useful for evaluating oral health and its impact on daily functioning17,18.
Recent clinical studies have increasingly highlighted a significant link between chronic diseases and having less than 20 natural teeth19. Chronic diseases can disrupt the oral microbiome and elevate systemic inflammatory factors, both of which contribute to periodontal disease—a key predictor of having less than 20 natural teeth20,21,22. Additionally, chronic diseases and having less than 20 natural teeth often share common risk factors, including smoking, excessive alcohol consumption, and poor dietary habits such as rich in sugary and processed foods16,23. For instance, smoking significantly impairs gum health and immune function, increasing the risk of having less than 20 natural teeth by more than four times24,25.
Chronic diseases often cluster, a phenomenon known as multimorbidity, which the World Health Organization defines as the presence of two or more chronic diseases that require medical management or impacting daily activities26,27,28,29. While existing research largely focuses on the relationship between high-prevalence conditions like hypertension, heart disease, and diabetes with having less than 20 natural teeth30,31,32,33, limited attention has been given to other chronic conditions such as lung disease, cataracts, Parkinson’s disease, and rheumatoid arthritis34,35,36,37,38,39,40,41,42. Furthermore, most studies focus on single diseases rather than the cumulative impact of multimorbidity on dysfunctional dentition. Therefore, from the perspective of multimorbidity, this study expands the scope of chronic disease and assesses the association between multimorbidity and having fewer than 20 natural teeth in a nationally representative sample of Chinese elderly people.
Objectives
This research aims to examine the relationship between multimorbidity and having less than 20 natural teeth among older adults aged 60 and above in China. We hypothesize that among Chinese older adults, there will be an association between multimorbidity and having less than 20 natural teeth. The study seeks to provide insights into the associations between multimorbidity and oral health, particularly highlighting the prevalence of dental issues among older individuals with multiple chronic conditions, and to underscore the importance of oral health prevention and protection in this population.
Method
All the data of the elderly in this study are derived from the CLHLS database. The Chinese Longitudinal Healthy Longevity Survey (CLHLS), organized by the Center for Healthy Aging and Development Studies, is a comprehensive longitudinal study spanning 23 provinces, municipalities, and autonomous regions across China. The sampling design of the CLHLS employs a multi-stage proportionate and targeted random sampling method43,44. To avoid deviation caused by age imbalance, we weighted the data by age. The CLHLS investigators conducted face-to-face interviews with older and middle-aged individuals to collect data. Data for the analysis were retrieved from the Chinese Longitudinal Healthy Longevity Survey (CLHLS,2017–2018), which included 15,874 individuals (≥ 50 years). In this study, all methods were performed in accordance with Declaration of Helsinki and Strengthening the Reporting of Observational studies in Epidemiology.
The inclusion criteria for the study sample were as follows: (1) older adults aged between 60 and 90 years; (2) no missing responses pertaining to the number of missing teeth; and (3) complete responses on the presence or absence of chronic diseases. The exclusion criteria are the presence of missing or incorrectly filled data for any of other related variables. Ultimately, a total of 3,640 valid participants were included in the study.
Assessment of having less than 20 natural teeth
The assessment of having less than 20 natural teeth was carried out by asking the question: “How many natural teeth do you currently have, excluding any dentures or artificial replacements?” As stipulated in the “8020 Plan” introduced by the World Health Organization in 2001, the possession of at least 20 natural teeth is deemed the minimum threshold for an individual to engage fully in social activities and maintain adequate chewing capability17. Furthermore, previous studies have consistently demonstrated that this metric possesses good reliability and validity16,19.
Assessment of multimorbidity
Multimorbidity was assessed through the inquiry, “Do you currently suffer from any of the following chronic diseases?” The diseases considered included chronic lung disease, tuberculosis, cataracts, glaucoma, gastrointestinal ulcers, Parkinson’s disease, rheumatism or rheumatoid arthritis, and chronic nephritis. Subsequently, the participants’ chronic disease status was categorized into three groups: (1) absence of any chronic disease, (2) presence of a single chronic disease, and (3) multimorbidity, defined as the coexistence of two or more chronic diseases. Notably, previous research has consistently demonstrated the reliability and validity of this assessment method45.
Covariates
Covariates were selected from the questionnaire that might be associated with having less than 20 natural teeth and multimorbidity, which were divided into sociodemographic characteristics and health behavior habits. Table 1 shows the specific variables.
Statistical analysis
The data were analyzed using the version of SPSS by IBM 25.0. Descriptive statistics were computed for demographic data using percentages and frequencies (n). In this study, having less than 20 natural teeth was taken as the dependent variable and multimorbidity as the independent variable. The chi-square test was employed to compare differences in the prevalence of having less than 20 natural teeth across demographic variables and multimorbidity status. Variables found to be significant in the chi-square test were subsequently included in the binary logistic regression model to identify influencing factors of having less than 20 natural teeth, which was coded as functional = 0 (reference group for univariate and multivariate analyses) and non-functional = 1. Adjusted odds ratios (ORs) and their corresponding 95% confidence intervals (CIs) derived from the logistic regression analysis were utilized to quantify the association between multimorbidity and having less than 20 natural teeth. Additionally, interaction terms between covariates were incorporated into the logistic regression model to test for potential interactions, with statistical significance for interactions set at p for interaction < 0.05. All interaction terms were included simultaneously in the original model to evaluate their combined effects comprehensively. The significance of each interaction term was determined using p-values obtained from the Wald test. The Hosmer-Lemeshow test was conducted to assess the fitness of the logistic regression model. Throughout the analysis, statistical significance was considered at p < 0.05, and p values were interpreted in a two-sided manner.
Results
Demographic characteristics of respondents
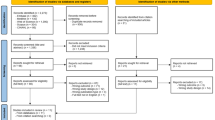
Figure 1 provides a detailed information of the inclusion and exclusion criteria that were used to screen 3,640 older persons who were eventually included in the research. 50.36% of participants were female, with an average age of 75 years. Most of the older adults (85.80%) had sufficient sources of income, and 80.47% of the adults regularly participated in annual physical examinations. Another 56.24% of the older adults have received nine-year compulsory education. In the present study, 58.27% of older adults experienced having less than 20 natural teeth.

Data Screening Flowchart.
Analysis of differences in having less than 20 natural teeth rates among older adults
The findings presented in Table 2 show that instead of ventilation condition, staple food, main taste preference, smoking, medical expenses in the past year, and annual physical examinations, other covariates may be associated with having less than 20 natural teeth in older adults.
After controlling for sociodemographic variables and health behaviors, Table 3 shows the association between multimorbidity and having less than 20 natural teeth. Compared with those without chronic disease, the odds ratio (OR) of having less than 20 natural teeth was 1.32 (95% CI: 1.10, 1.57) for older adults with only one chronic disease, and the OR for those with two or more chronic diseases was 1.418 (95% CI: 1.06, 1.89). Additionally, we identified several other factors linked to having less than 20 natural teeth, such as age, education level, ability to perform daily activities, frequency of vegetable intake, frequency of brushing teeth, toothache in the past six months, and BMI.
The Hosmer-Lemeshow test was conducted to assess the fitness of the logistic regression model. Since the significance level (p = 0.777) is greater than the commonly used significance level of 0.05, it indicates that there is no significant difference between the observed and predicted values.
The results in Fig. 2 showed that among the numerous factors included, only the interaction between frequency of brushing teeth and multimorbidity demonstrated a significant association(p for interaction < 0.05). This indicates that, at different frequency of brushing teeth, the impact of multimorbidity on tooth loss varies.

The Odds Ratios (95% Confidence Interval) of having less than 20 natural teeth among different demographic characteristics and multimorbidity groups of older adults in China. The horizontal line (X-axis) represents the 95% confidence interval of the OR value; The center vertical line (OR = 1) serves as a reference line perpendicular to the X-axis, indicating no effect; The small square is positioned at the OR value of the confidence interval.
Discussion
The results indicated that there was an association between multimorbidity and having less than 20 natural teeth among the older adults. Older adults with multimorbidity were found to have a higher prevalence of having less than 20 natural teeth compared to those without chronic diseases.
Having less than 20 natural teeth is a major public health issue influenced by biological, behavioral, and socioeconomic factors7, in addition to the two main causes of dental caries and periodontitis, we also found that common demographic characteristics and health behavior habits, such as gender, age, education level, and marital status, influence the rate of having less than 20 natural teeth among the older adults in this study. This is consistent with previous research findings46,47. Specifically, age is positively correlated with having less than 20 natural teeth, and this phenomenon increases steeply when the age reaches 70 years old48. Additionally, education level may have a significant impact on having less than 20 natural teeth in this study. We observed that older adults with no education are more likely to suffer from having less than 20 natural teeth compared to those with education. From a social perspective, higher education levels provide better access to resources and higher health awareness, influencing lifestyle and behavior49, meanwhile, older adults without education often lack knowledge about oral health and dental care, leading to poorer oral health and higher rates of having less than 20 natural teeth50. The findings demonstrate that older adults who engage in regular tooth brushing and physical exercise exhibit a significantly reduced risk of having less than 20 natural teeth. Notably, the frequency of brushing teeth serves as a significant moderating factor in the association between multimorbidity and having less than 20 natural teeth, suggesting that oral hygiene behaviors may play a buffering role in mitigating the adverse effects of systemic chronic diseases on oral health. Furthermore, the observed relationship implies that having less than 20 natural teeth is closely linked to individual activity levels. Collectively, these findings emphasizing that enhancing awareness of daily physical activities, structured exercise among older adults and improving their self-care capacity could reduce the risk of severe tooth loss in this population.
This study focuses on the association between multimorbidity and having less than 20 natural teeth among older adults. The results indicate that there is an association between multimorbidity and having less than 20 natural teeth in the older adult population. This result is consistent with the findings of Mohamed45. Older adults with two or more chronic diseases tend to have a higher prevalence of having less than 20 natural teeth compared to those without chronic diseases. Existing research shows that patients with multimorbidity often experience multi-organ involvement and greater systemic inflammatory responses, leading to the overexpression of inflammatory factors, which exacerbates periodontal infections and causes the condition of having less than 20 natural teeth51. Furthermore, scholars like Hayata et al. have found that pathogenic bacteria in the mouths of individuals with having less than 20 natural teeth can colonize the respiratory or digestive tract, contributing to the development of lung diseases such as chronic obstructive pulmonary disease, which indicates that there may be a potential bidirectional relationship between multimorbidity and having less than 20 natural teeth52. On the other hand, older adults with multimorbidity often require polypharmacy for treatment, and many medications, especially anticholinergics, antidepressants, and some bronchodilators, can induce dry mouth53. Dry mouth not only causes chewing and swallowing problems but also affects taste, speech, denture tolerance, and increases the risk of oral mucosal diseases and caries (tooth decay), leading to a higher risk of having less than 20 natural teeth54,55.
It is crucial to recognize the association between multimorbidity and having less than 20 natural teeth among older adults and consider the oral condition of patients when treating those with multiple chronic diseases. Currently, several states in the United States have successfully piloted integrated treatment programs for chronic diseases and oral health, promoting collaboration between various departments to deal with chronic diseases and oral health55. This association has not yet received much attention in China. However, with the progression of healthcare in China, oral health has been incorporated into the “China Health Action 2030” blueprint56, indicating a promising future where China will pay increasing attention to the oral health. Medical staff should offer oral health education specifically tailored for older adults with multimorbidity. Develop relevant public health prevention plans that address the relationship between multimorbidity and having less than 20 natural teeth, and provide optimal dental service conditions for older people living in economically disadvantaged and poorly educated areas, which can help reduce the risk of having less than 20 natural teeth14.
Strengths and limitations of the study
The advantage of this study lies in its focus on the relationship between multimorbidity and having less than 20 natural teeth among the older adults in China, while also expanding the scope of chronic diseases studied. Currently, most research concentrates on a few common chronic diseases such as hypertension and diabetes, with less attention given to other chronic conditions like cataracts and tuberculosis in relation to tooth loss. By broadening the range of chronic diseases under investigation, this study can more comprehensively explore the relationships between these diseases and having less than 20 natural teeth in the older adults, thereby providing a more complete scientific basis for future prevention and intervention measures.
However, this study also has certain limitations. First, it employs a cross-sectional design. Although our findings clearly indicate a relationship between the presence of multimorbidity and having less than 20 natural teeth, the study does not provide longitudinal observations on having less than 20 natural teeth, thus preventing the establishment of a temporal relationship and exploration of a definitive causal relationship between the two. In addition, since the study participants are older adults aged 60 and above, recalling past exposure history or medical history may lead to memory distortion or incomplete recollection due to the long passage of time, and there may be bias in self-perception when answering questionnaires in self-examination of disease. Furthermore, disease status was determined using a self-reported strategy, which poses a limitation regarding the accuracy of the data. Participant may have recall bias during the process of recall, resulting in self-reported underestimation or overestimation due to inaccurate or incomplete memory. This bias is particularly common in studies that rely on self-reported data, affecting the reach and generalizability of the study’s results.
In this study, we incorporated all interaction terms simultaneously into the logistic regression model to comprehensively assess potential interaction effects. While this approach allowed for straightforward evaluation of multiple interactions, it also increased the risk of multicollinearity, potentially leading to unstable coefficients and reduced interpretability. Moreover, the complexity of the model might have masked subtle interactions that could be better identified individually. Future research could adopt a stepwise approach to introduce interaction terms sequentially, minimizing multicollinearity and providing clearer insights into each interaction’s contribution.
In addition, the database used in this study employed an oversampling method, which may have introduced age distribution bias. Interaction analysis revealed a significant influence of age on the relationship between multimorbidity and having less than 20 natural teeth. However, this study did not further explore its specific mechanism, and we look forward to future research providing deeper insights into this aspect.
Conclusions
There is an association between multimorbidity and having less than 20 natural teeth in the older adults. Healthcare professionals should pay attention to the oral health of patients with multimorbidity while treating their chronic conditions and guide patients to use oral care resources appropriately in the early stages of their disease. This will help raise awareness of oral health care and enhance the prediction of risks related to having less than 20 natural teeth and chronic systemic diseases. The findings emphasize the relationship between the oral health of older adults and multimorbidity. Oral health institutions should implement measures to prevent older adults with multimorbidity from having less than 20 natural teeth and develop more comprehensive public health policies to ensure their oral health.
Data availability
This study is based on the dataset of the Longitudinal Healthy Longevity Survey (CLHLS) in China Longevity Region. The data utilized in this study is freely accessible on the Peking University Open Research Data Platform, accessible via the following https://doi.org/10.18170/DVN/WBO7LK.
Abbreviations
- CLHLS:
-
Chinese Longitudinal Healthy Longevity Survey
References
Parker, M. L. J. M. M. & Report, M. W. Prevalence of and changes in tooth loss among adults aged ≥ 50 years with selected chronic conditions—United States, 1999–2004 and 2011– 2020, 69. (2016).
Hayasaka, K. et al. Tooth loss and mortality in elderly Japanese adults: effect of oral care. Journal of the American Geriatrics Society. 61(5), 815–820 (2013).
Garcia Perez, A., Rodríguez González, K. G., Rodríguez Chávez, J. A. & Velázquez-Olmedo, L. B. Marginalization and tooth loss in older Mexican adults. Community Dent. Health. 40(4), 242–247 (2023).
Randolph, W. M., Ostir, G. V. & Markides, K. S. Prevalence of tooth loss and dental service use in older Mexican Americans. J. Am. Geriatr. Soc. 49(5), 585–589 (2001).
Adegboye, A. R. A., Twetman, S., Christensen, L. B. & Heitmann, B. L. Intake of dairy calcium and tooth loss among adult Danish men and women. Nutrition 28(7–8), 779–784 (2012).
Saintrain, M. V. L. & de Souza, E. H. A. J. G. Impact of tooth loss on the quality of life. 29(2), e632–e636 (2012).
Baelum, V., Helderman, W. V., Hugoson, A., Yee, R. & Fejerskov, O. A global perspective on changes in the burden of caries and periodontitis: implications for dentistry. J. Rehabil. 34(12), 872–906 (2007).
Oral health in America. : a report of the surgeon general. J. Calif. Dent. Assoc. 28(9), 685–695 (2000).
WHO. Sugars and Dental caries - Technical Information Note (WHO, 2017).
Shigli, K., Hebbal, M. & AngadiGS Relative contribution of caries and periodontal disease in adult tooth loss among patients reporting to the Institute of dental sciences, Belgaum, India. Gerodontology 26(3), 214–218 (2009).
de Abreu, M., Cruz, A. J. S., Borges-Oliveira, A. C., Martins, R. C. & Mattos, F. F. Perspectives on Social and Environmental Determinants of Oral Health. Int J Environ Res Public Health. 18(24), 13429, 1–15 (2021).
Roberto, L. L., Silveira, M. F., de Paula, A. M. B., Ferreira, E. F., Martins, A. M. E. B. L., Haikal, D. S. Contextual and individual determinants of tooth loss in adults: a multilevel study. BMC Oral Health. 20(1), 73 (2020).
Jimenez, M., Dietrich, T., Shih, M. C., Li, Y. & Joshipura, K. J. Racial/ethnic variations in associations between socioeconomic factors and tooth loss. Community Dent. Oral Epidemiol. 37(3), 267–275 (2009).
Lee, H., Kim, D., Jung, A., & Chae, W. (2022). Ethnicity, Social, and Clinical Risk Factors to Tooth Loss among Older Adults in the U.S., NHANES 2011-2018. International journal of environmental research and public health. 19(4), 2382 (2022).
Tôrres, L., Hilgert, J. B., Hugo, F. N., Sousa, M. & De Marchi, R. J. Predictors of tooth loss in Brazilian older adults: an 8-year follow-up. Gerodontology 40(2), 207–212 (2023).
Bomfim, R. A., Cascaes, A. M. & de Oliveira, C. Multimorbidity and tooth loss: the Brazilian National health survey, 2019. BMC Public. Health. 21(1), 8 (2021).
Petersen, P. E. & Kwan, S. The 7 < SUP > th WHO Global Conference on Health Promotion - towards integration of oral health (Nairobi, Kenya 2009). Community Dent Health 27(2), 129–136 (2010).
Yuan, J. Q. et al. Number of natural teeth, denture use and mortality in Chinese elderly: a population-based prospective cohort study. Bmc Oral Health. 20(1), 11 (2020).
Zhang, Y. Q., Leveille, S. G. & Shi, L. Multiple chronic diseases associated with tooth loss among the US adult population. Front. Big Data. 5, 10 (2022).
Graves, D. T., Corrêa, J. D. & Silva, T. A. The oral microbiota is modified by systemic diseases. Journal of Dental Research. 98, 148–156 (2019).
Falcao, A. & Bullón, P. A review of the influence of periodontal treatment in systemic diseases. Periodontol 2000. 79(1), 117–128 (2019).
Nibali, L. et al. Tooth loss in aggressive periodontitis: a systematic review. Journal of Dental Research. 92(10), 868–875 (2013).
Zhu, Y. & Hollis, J. H. Tooth loss and its association with dietary intake and diet quality in American adults. J. Dent. 42(11), 1428–1435 (2014).
Krall, E., Dawson-Hughes, B., Garvey, A. & Garcia, R. Smoking, smoking cessation, and tooth loss. Journal of Dental Researc. 76(10), 1653–1659 (1997).
Hanioka, T. et al. Causal assessment of smoking and tooth loss: A systematic review of observational studies. BMC Public. Health. 11, 10 (2011).
Wolff, J. L., Starfield, B. & Anderson, G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch. Intern. Med. 162(20), 2269–2276 (2002).
van den Akker, M., Buntinx, F., Metsemakers, J. F. M., Roos, S. & Knottnerus, J. A. Multimorbidity in general practice: prevalence, incidence, and determinants of co-occurring chronic and recurrent diseases. J. Clin. Epidemiol. 51(5), 367–375 (1998).
Vetrano, D. L. et al. Chronic diseases and geriatric syndromes: the different weight of comorbidity. Eur. J. Intern. Med. 27, 62–67 (2016).
Organization, W. H. Multimorbidity. (2016).
Shin, H. S. Association between the number of teeth and hypertension in a study based on 13,561 participants. J. Periodontol. 89(4), 397–406 (2018).
Raju, K., Taylor, G. W., Tahir, P. & Hyde, S. S. Association of tooth loss with morbidity and mortality by diabetes status in older adults: a systematic review. BMC Endocr. Disord. 21, 79 (2021).
Patel, M. H., Kumar, J. V. & Moss, M. E. Diabetes and tooth loss an analysis of data from the National health and nutrition examination survey, 2003–2004. J. Am. Dent. Assoc. 144(5), 478–485 (2013).
Okoro, C. A. et al. Tooth loss and heart disease: findings from the behavioral risk factor surveillance system. Am. J. Prev. Med. 29(5 Suppl 1), 50–56 (2005).
Dwibedi, N., Wiener, R. C., Findley, P. A., Shen, C. & Sambamoorthi, U. Asthma, chronic obstructive pulmonary disease, tooth loss, and edentulism among adults in the united States 2016 behavioral risk factor surveillance system survey. J. Am. Dent. Assoc. 151(10), 735 (2020).
Park, J. H., Lee, H., Kim, J. W. & Song, T. J. Better oral hygiene is associated with a reduced risk of cataract: A nationwide cohort study. Front. Med. 9, 8 (2023).
Huang, L. et al. The role of the microbiota in glaucoma. Molecular Aspects of Medicine. 94, 101221 (2023).
Boylan, M. R., Khalili, H., Huang, E. S. & Chan, A. T. A prospective study of periodontal disease and risk of gastric or duodenal ulcer in men. Gastroenterology 142(5), S85–S85 (2012).
Hanaoka, A. & Kashihara, K. Increased frequencies of caries, periodontal disease and tooth loss in patients with Parkinson’s disease. J. Clin. Neurosci. 16(10), 1279–1282 (2009).
Woo, H. G., Chang, Y., Lee, J. S. & Song, T. J. Association of Tooth Loss with New-Onset Parkinson’s Disease: A Nationwide Population-Based Cohort Study. Parkinsons Dis 2020:8. (2020).
Han, K. & Park, J. B. Tooth loss and risk of end-stage renal disease: A nationwide cohort study. J. Periodontol. 92(3), 371–377 (2021).
Ioannidou, E., Swede, H., Fares, G. & Himmelfarb, J. Tooth loss strongly associates with malnutrition in chronic kidney disease. J. Periodontol. 85(7), 899–907 (2014).
De Pablo, P., Dietrich, T. & McAlindon, T. E. Association of periodontal disease and tooth loss with rheumatoid arthritis in the US population. The Journal of Rheumatology. 35, 70–76 (2008).
Zeng, Y., Feng, Q. S., Hesketh, T., Christensen, K. & Vaupel, J. W. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: a cohort study. Lancet 389(10079), 1619–1629 (2017).
Zeng, Y. Towards deeper research and better policy for healthy aging --Using the unique data of Chinese longitudinal healthy longevity survey. China Economic J. 5(2–3), 131–149 (2012).
Hag Mohamed, S., & Sabbah, W. . Is tooth loss associated with multiple chronic conditions? Journal of the American Osteopathic Association. 81(6), 443–448 (2023).
Pitchika, V. et al. Factors influencing tooth loss in European populations. Journal of clinical periodontology. 49, 642–653 (2022).
Natto, Z. S., Aladmawy, M., Alasqah, M. & Papas, A. Factors contributing to tooth loss among the elderly: A cross sectional study. Singap. Dental J. 35, 17–22 (2014).
Kassebaum, N. J. et al. Global burden of severe tooth loss: A systematic review and Meta-analysis. J. Dent. Res. 93(7), 20–28 (2014).
Elani, H. W. et al. Social inequalities in tooth loss: A multinational comparison. Commun. Dent. Oral Epidemiol. 45(3), 266–274 (2017).
Fukuhara, S. et al. Association of education and depressive symptoms with tooth loss. J. Dent. Res. 100(4), 361–368 (2021).
Yarmohammadi, R., Mortazavi, H., Rahmani, A. & Rahmani, S. J. I. J. M. R. Tooth loss related to systemic diseases. 2(4), 331–337 (2015).
Hayata, M. et al. The periodontopathic bacterium Fusobacterium nucleatum induced Proinflammatory cytokine production by human respiratory epithelial cell lines and in the lower respiratory organs in mice. Cell. Physiol. Biochemistry: Int. J. Experimental Cell. Physiol. Biochem. Pharmacol. 53(1), 49–61 (2019).
Villa, A. et al. World workshop on oral medicine VI: a systematic review of medication-induced salivary gland dysfunction: prevalence, diagnosis, and treatment. Clin. Oral Investig. 19(7), 1563–1580 (2015).
Narhi, T. O. et al. 76-YEAR-OLD, 81-YEAR-OLD, AND 86-YEAR-OLD INHABITANTS IN HELSINKI, FINLAND. J. Dent. Res. 71(12), 1875–1880 (1992).
Linabarger, M., Brown, M. & Patel, N. A pilot study of integration of medical and dental care in 6 States. Prev. Chronic Dis. 18, 11 (2021).
Sun, X. Y., Bernabé, E., Liu, X. N., Zheng, S. G. & Gallagher, J. E. Meeting the oral health needs of 12-year-olds in China: human resources for oral health. BMC Public. Health. 17, 12 (2017).
Wang, D. et al. Association between marital relationship and Multimorbidity in middle-aged adults: a longitudinal study across the US, UK, Europe, and China. Maturitas 155, 32–39 (2022).
Thiam, S. et al. Impact Of Obstructive Lung Diseases (Asthma and COPD) due to indoor air pollution and poor room ventilation quality in Medina (Senegal). Journal of Toxicology and Health. 10, 1 (2023).
Li, H., Jia, P. & Fei, T. Associations between taste preferences and chronic diseases: a population-based exploratory study in China. Public. Health Nutr. 24(8), 2021–2032 (2021).
de Medeiros, T. C. C., Areas, E. S. A., Prates, R. C., Chapple, I. & Steffens, J. P. Association between tooth loss, chronic conditions, and common risk factors: results from the 2019 Brazilian health survey. J. Periodontol. 93(8), 1141–1149 (2022).
Shan, L., Wu, Q. & Li, Y. Demand and utilization of medical service, medical expenses and family economic risks among chronic disease patients with different medical insurance systems in China. Chin. J. Public. Health. 37(4), 608–614 (2021).
Pathak, R. et al. Should we abandon annual physical examination? - A meta-analysis of annual physical examination and all-cause mortality in adults based on observational studies. Prev. Med. 161, 107130 (2022).
Hirano, K., Shimbo, T., Komatsu, Y. & Kobayashi, D. Frequency of tooth brushing as a predictive factor for future kidney function decline. J. Nephrol. 35(1), 191–199 (2022).
Drumond, V. Z. et al. Tooth loss from the perspective of studies employing a life course approach: a systematic review. Health promotion international vol. 39, 5 (2024).
Acknowledgements
We thank all participants at the study sites for their cooperation. We wish to thank the reviewers for their insightful comments and suggestions.
Funding
This work was supported by the National Natural Science Foundation of China under Grant [number:72104098], Guangdong Basic and Applied Basic Research Foundation under Grant [number:2023A1515010902], Open Fund of Key Research Base of Philosophy and Social Science of Higher Education in Guangdong Province-Local Government Development Research Institute of Shantou University [number:07423002-07], Science and Technology Projects in Guangzhou [number:2025A04J4169], Scientific Research Project of School of Humanities in Harbin Medical University: Research on Training Pathways for Elderly Care Professionals Based on a Competency-Based Perspective [number:HMURW20210203], Basic Scientific Research Business Fee Project of Provincial Universities in Heilongjiang Province: The Evolutionary Trajectory of Digital Inclusion in the Elderly Population and the Construction of a Support System: A Care Ethics Perspective and Key Laboratory of Philosophy and Social Sciences of Colleges and Universities in Guangdong Province under Grant[number:2023WSYS005]. The sponsor had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
Yang Fu, Mei Yin, and Lei Shi conducted research; Wu Yi, Hui Liu Yue Qin, HaoRan Chen and Junling Ma wrote papers; Wu Yi, Hui Liu, Yue Qin, HaoRan Chen, Mei Yin, Lei Shi, and Yang Fu provided administrative, technical or material support and critically revised the important intellectual content of the manuscript; All the authors revised the final version of the manuscript, and Yang Fu, Mei Yin, and Lei Shi gave the final approval.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was approved by the ethics committees from both the Duke University Institutional Review Board (Protocol No. Pro00062871) and the Peking University Biomedical Ethics Committee (Approval No. IRB00001052-13074). The CLHLS database has not been clinically registered. All methods were performed in accordance with Declaration of Helsinki and Strengthening the Reporting of Observational studies in Epidemiology. Written informed consent was obtained from all participating individuals prior to their enrollment in the study.
Consent for publication
Not Applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wu, Y., Liu, H., Qin, Y. et al. Association between multimorbidity and having less than 20 natural teeth among Chinese older adults: a cross-sectional study. Sci Rep 15, 7865 (2025). https://doi.org/10.1038/s41598-025-92426-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-92426-6
