
Abstract
Compound heat anomalies associated with humidity, such as compound hot-dry events and hot-wet events, pose greater health risks than single heat anomalies. Here, we utilize ambulance dispatch data along with air temperature and relative humidity to study human impacts on these events in China. We show that relying solely on temperature without considering humidity may underestimate the health risks of these events on populations. Over the past 40 years, anthropogenic activities have increased hot-dry events by 2.34 times and decreased hot-wet events by 0.63 times, especially in the Yangtze River region, compared to natural forcing. We also speculate that, in the future up to 2060, under the carbon-neutral scenario, the frequencies of high health-risk hot-dry events and hot-wet events caused by human activities can be reduced by one-half and over one-fifth, respectively, compared to the high-emissions scenario. These findings provide guidance for assessing health risks under global warming.
Similar content being viewed by others

Introduction
Compound heat events, encompassing both compound hot and dry events (CHDEs) and compound hot and wet events (CHWEs), have become increasingly frequent and intense in recent years, raising significant concerns due to their profound impacts on human health1,2. These events, characterized by concurrent extreme temperature (T) and humidity conditions, are closely linked to human activities, which have been altering the climate system rapidly3,4. Understanding the impact of these events necessitates a comprehensive investigation, particularly given the escalating exposure of human populations to such high health-risk compound events.
CHDEs, characterized by contiguous hot days without precipitation, can lead to increased demand for water and energy resources5,6. They also promote and intensify the formation of unfavorable urban climates by increasing allergens and particulate matter concentrations, posing serious threats to urban dwellers’ health7. Furthermore, such conditions are associated with a higher incidence of heat-related illnesses, cardiovascular and respiratory diseases, and other health impacts, particularly among vulnerable populations8. CHWEs, on the other hand, exacerbate human discomfort by increasing heat stress, which is intensified by high humidity9. These conditions foster the growth of mold and mildew, which can trigger respiratory problems such as asthma and allergies10,11. Additionally, stagnant water resulting from heavy rainfall can serve as breeding grounds for mosquitoes and other disease vectors, increasing the transmission of diseases like malaria, dengue fever, and Zika virus12,13,14. However, despite the identified health risks, traditional assessments of health relative risks (RR) have focused primarily on single T indices, overlooking the significant impact of relative humidity (RH). Both T and RH are critical meteorological factors influencing human heat-related health15, highlighting the need for a more integrated approach.
Previous research has detected a significant increase in the frequency of CHDEs and CHWEs under present and future climate conditions in many regions of the world16,17,18,19, including China20,21,22,23,24. Numerous studies confirm that anthropogenic activities, especially greenhouse gas emissions, urbanization, and industrialization, are the primary drivers of the increase in extreme T, extreme precipitation, and drought events on both regional and global scales23,25,26,27,28,29,30. Typically, studies compare observations with simulations [historical (ALL) and natural-only (NAT)] in pairs, assessing anthropogenic and natural factors31. This conventional approach involves evaluating whether there have been changes in the likelihood or intensity of climate events based on observations. It aligns these changes with the influence of human activities in models and calculates metrics such as ‘probability ratio (PR)’ and ‘fraction of attributable risk (FAR)'31,32,33. This method has proven successful in analyzing the contribution of human activities to extreme events, particularly in relation to T extremes governed by the thermodynamics of climate change19,34,35,36. However, the detection and attribution of compound hot events have been notably constrained, with a conspicuous absence of integration with health data. This limitation impedes the ability to establish meaningful connections between climatic factors and public health outcomes.
The critical need to study the impacts of CHDEs and CHWEs stems from their increasing prevalence and the severe health risks they pose. While existing research has identified the rising frequency of these compound events and attributed them to anthropogenic factors, there is a significant gap in understanding their direct impact on human health. This gap is particularly concerning given the distinct and severe health threats posed by CHDEs and CHWEs, such as heat-related illnesses, respiratory issues, and vector-borne diseases37,38. By utilizing health data along with T and RH data, this article aims to assess the impact of human activities on the variations of high health-risk compound T-RH events. In addition, it projects the changes in health-risk compound heat events under different future scenarios, including both carbon-neutral and high-emission situations, thereby assessing the health benefits of carbon neutrality.
Results
Observed changes in high health-risk CHDEs and CHWEs
In this study, we determined the threshold values for high health-risk CHDEs/CHWEs, which are illustrated in Fig. 1. The detailed methodology and the definition are described in the Materials and Methods.

Relative risk (RR) during CDHEs and CHWEs is defined by 200 combined types of T (50 to 100th percentile, with intervals of 5th) and RH combinations (0 to 100th percentile, with intervals of 5th) in China. The gray shading denotes combinations of T and RH where the RR exceeds 1.08. Orange/purple pentagrams represent the T and RH thresholds for high health-risk CHDEs/CHWEs. The orange/purple boxes represent the T and RH thresholds associated with high health-risk CHDEs/CHWEs.
Using this high health-risk threshold, we evaluated the observational climatology and linear trends in the frequencies of high health-risk CHDEs and CHWEs days (Figs. 2, 3a, b). This analysis was conducted before assessing the detection and attribution of human activities’ contributions over China for the period 1979–2014, utilizing ERA5 data. This study primarily focuses on the warm season (May-September), as occurrences of CHDEs and CHWEs are nearly non-existent during the remaining months. In terms of the warm seasons, it is noteworthy that high-health-risk CHDEs and CHWEs exhibit distinct geographical and temporal patterns of prevalence. The highest occurrence of high health-risk CHDEs was observed in the northwestern region of China and the middle-lower reaches of the Yangtze River, with approximately 10–20 days of such events annually (Fig. 2a). On the other hand, the Qinghai-Tibet Plateau and Northeastern region witnessed the maximum frequency of high health-risk CHWEs, experiencing around 20–30 days of these events annually (Fig. 2d). It’s worth noting that these high-incidence areas also coincide with regions exhibiting rapid growth from 1979 to 2014 (Fig. 2b, e). In the analysis based on a monthly perspective, high health-risk CHDEs were predominantly observed in May and June, with subsequent occurrences in August, July, and September (Fig. 2c). Meanwhile, high health-risk CHWEs primarily occurred in July and August, followed by May, June, and September (Fig. 2f).

Spatial distribution of climatology (units: days) for the frequency of a high health-risk CHDEs and d high health-risk CHWEs during 1979−2022 based on ERA5. Linear trends (units: day/10a) for the frequency of b high health-risk CHDEs and e high health-risk CHWEs for (a, d) observations. The frequency of c high health-risk CHDEs and f high health-risk CHWEs across the Chinese region from May to September each year. The dotted area indicates that the linear trend is significant at the 95% confidence level.

a, b Time series of frequency for the observed (OBS; marked in black; 1979–2022; units: day), ALL simulated (red line; 1979–2014), and NAT simulated (blue line; 1979–2014) high health-risk a CHDEs and b CHWEs during the warm season (May to September) in China. The colored solid lines indicate the multi-model ensembles of the 10 models, and the corresponding shadings indicate the model spreads. c, d Original (bar) and GEV-fitted PDFs (solid line) of observations (gray bar and black line) and ALL simulations (pink bar and red line) and NAT simulations (light blue bar and blue line) for c high health-risk CHDEs and d high health-risk CHDEs. The purple dashed line represents the 80th percentile of the time series data for OBS.
The impact of human activities on high health-risk CHDEs and CHWEs
Nationwide impact
The simulated ensemble means 10 all-forcing (ALL and natural-only forcing NAT simulations using CMIP6 data show spatial correlation coefficients both exceeding 0.80 (Supplementary Fig. S4). Moreover, the correlation coefficients for the time series between the observed warm-season national averages from 1979 to 2014 with ALL’s are 0.65 for CHDEs and 0.72 for CHWEs, respectively (P < 0.01; see Fig. 3a, b). This indicates that ALL simulations reasonably well capture the variability of observed high health-risk CHDEs and CHWEs.
Figure 3c, d shows the GEV-fitted probability density functions (PDFs) of high health-risk CHDEs and CHWEs under different external forcings. We pooled all relevant data for each year (from May to September) to fit the GEV distribution, ensuring a comprehensive capture of extreme values associated with these events. PDFs of high health-risk CHDEs and high health-risk CHWEs exhibit similar distributions between model simulations and observations with p values of 0.46 and 0.41, respectively, according to the two-sample KS test. These results suggest that ALL simulations can be considered reliable for the attribution of the event. Here, this is exemplified by the occurrence corresponding to the 80th percentile of the time series for observations, which captures higher values in the time series, also applicable with the 90th, etc., for analyzing extreme years.
Results show that, for high health-risk CHDEs, the ALL simulations distributions show a relatively lower and wider shape and a shift to higher amounts as compared to the NAT simulations climate. This suggests a greater likelihood of CHDE occurrence in response to anthropogenic forcing. Specifically, the estimated occurrence probability increased from 9.2% [95% confidence interval (CI): 9.2–9.4%] in NAT simulations to 21.5% (95% CI: 21.4–21.7%) in ALL simulations, with a PR of 2.34 (95% CI: 2.28–2.36) and a FAR of 0.43 (95% CI: 0.42–0.44). This indicates that human activities have increased high health-risk CHDEs to ~2.34 times, with human activities contributing to about 43% of the occurrence of this event.
However, for high health-risk CHWEs, the distributions under ALL simulations indicate a shift towards lower values compared to the NAT simulations climate. This shift indicates that the high health-risk CHWEs event is less likely to occur with anthropogenic influence. Specifically, the estimated occurrence probability decreased from 12.8% (95% CI: 12.7–12.8%) in NAT simulations to 8.0% (95% CI: 7.9–8.2%) in ALL simulations, with a PR of 0.63 (95% CI: 0.62–0.65) and a FAR of −0.60 (95% CI: −0.55– −0.62). This indicates that human activities have decreased high health-risk CHWEs to approximately 0.63 times, with human activities contributing to about 60% of the occurrence of this event.
These findings highlight the contrasting effects of human activities on high health-risk CHDEs and CHWEs, particularly in the middle and lower reaches of the Yangtze River region, even for almost the entire warm season in China (Supplementary Fig. S5).
Regional variation impact
Furthermore, to be more specific, the impact of human activities varies across different regions and months (Figs. 4, 5). Due to the regional characteristics of thermal discomfort days over China, we divided China territory into eight sub-regions to study thermal discomfort (Fig. 4a), including Northwest China (NWC), North China (NC), Northeast China (NEC), Southwest China part1 (SWC1), Central China (CC), Eastern China (EC), Southwest China part2 (SWC2), and South China (SC). These sub-regions have been widely used in climate change studies over China21,22,27. The high health-risk CHDEs in the NWC exhibit a significant increase attributable to human activities, particularly during the period spanning May to August (Figs. 4a–d, 5a–d). This escalation reaches its zenith in the month of August (Figs. 4d, 5d). high health-risk CHDEs in the SWC2 show a noteworthy increase in May, followed by a substantial decline in June (Figs. 4a, b, 5a, b), highlighting an earlier onset of elevated risk compared to the following month. Due to human activities, the high health-risk CHWEs in the SWC1 experienced a notable reduction during the months of July to August (Figs. 4h, i, 5h, i). Conversely, in the eastern sector of SWC1, there was a significant escalation in high health-risk CHWEs observed from August to September (Figs. 4i, j, 5i, j). Additionally, the monthly performance highlights in the CC and EC regions during the period of July to August. There has been a notable increase in high health-risk CHDEs in the CC and EC regions (Figs. 4c, d, 5c, d), while concurrently witnessing a significant decrease in high health-risk CHWEs (Figs. 4h, i, 5h, i). This phenomenon underscores the contrasting impacts of human activities, particularly in the middle and lower reaches of the Yangtze River region.

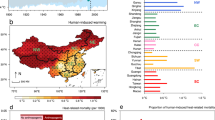
Spatial distribution of differences (units: day) between ALL simulations and NAT simulations from May to September for the regional average frequency of a–e high health-risk CHDEs (upper panels) and f–j high health-risk CHDEs (lower panels). The eight sub-regions over China are shown in a, including Northwest China (NWC), North China (NC), Northeast China (NEC), Southwest China part1 (SWC1), Central China (CC), Eastern China (EC), Southwest China part2 (SWC2), and South China (SC). Dots indicate regions where the difference is statistically significant at the 0.05 significance level.

The differences (units: day) between ALL simulations and NAT simulations from May to September for the regional average frequency of a–e high health-risk CHDEs (left panels) and f–j high health-risk CHDEs (right panels) over eight sub-regions during the period 1979−2014. The error bar represents the 95% CI. The black star denotes the differences above the 95% confidence level.
Future changes
We considered from 2021 to 2100 using the CMIP6 multi-model ensembles under three typical emissions scenarios (Fig. 6). The Shared Socioeconomic Pathway (SSP) 5–8.5 scenario signifies an exceptionally high greenhouse gas (GHG) emissions trajectory, serving as the upper limit among scenarios documented in the literature. The SSP-2-4.5 represents the intermediate GHG emissions scenario, reflecting the continuation of historical mitigation efforts39. The SSP-1-1.9 represents a scenario with very low GHG emissions and CO2 emissions declining to net zero around 2060, followed by net-negative CO2 emissions, which coincidently close to that in China’s carbon neutrality scheme2,40.

a The evolution of the occurrence frequencies (units: d/year) of high health-risk CHDEs and CHWEs using the CMIP6 multi-model ensembles under SSP-1-1.9, SSP-2-4.5, SSP-2-4.5nat, and SSP-5-8.5 scenarios from 2021 to 2100. b–d The bar plots in the panels depict the impacts of human activities on high health-risk CHDEs (red bars) and high health-risk CHWEs (green bars), respectively, across the eight sub-regions in China, spanning the near term (2021–2040), mid-term (2041–2060), and long-term (2081–2100). The impact of human activities is calculated by averaging regional differences under the SSP-2-4.5 scenario, as the corresponding SSP-2-4.5nat scenario stands as the sole option available on the official website. The solid red (green) lines represent the original values under three different scenarios, while the dashed red (green) lines represent the SSP-2.45nat scenario for the average regional occurrence of high health-risk CHDEs (high health-risk CHWEs). The shaded areas around the lines indicate a confidence level of 0.05 for each scenario. The symbols * represent statistical significance at levels of 0.05.
We estimate the future variation of time series during the warm season in China based on historical observation thresholds (Fig. 6a; for the spatial distribution, see Supplementary Fig. S6). In the future, up to 2060, under the SSP-1.19 scenario, high health-risk CHDEs and CHWEs increase to 1.41 and 1.71 times, respectively, compared to past climate conditions (the same goes for the following scenarios as well). Under SSP-2.45, these events are expected to rise to 1.92 and 2.03 times, while under SSP-5.85, they could soar to 3.05 and 2.13 times, respectively. Based on the results above, it can be concluded that in a carbon-neutral scenario, the frequencies of high health-risk CHDEs and CHWEs caused by human activities are reduced by one-half and one-fifth, respectively, compared to SSP-5.85.
Furthermore, our examination delved into the impact of human activities (Fig. 6b–d), with a specific focus on the SSP-2-4.5 scenario, as the corresponding SSP-2-4.5nat scenario stands as the sole option available on the official website. The influence of human activities (SSP-2-4.5 minus SSP-2-4.5nat), revealed a significant increase in high health-risk CHDEs during June in the NC region and July in the NWC region. Conversely, notable reductions in high health-risk CHWEs were observed predominantly in the SC region during June, extending to the EC and NEC regions in July and August. In the long term, as compared to the near and mid-term periods, the augmentation of high health-risk CHDEs in the NWC region, influenced by human activities, is expected to experience a delay until August. Simultaneously, the decline in high health-risk CHWEs in the SC region is expected to witness a contraction in timing, shortening from June-August to July-August. In summary, human activities are projected to reduce the occurrence of high health-risk CHWEs in eastern China in the future. Conversely, there is an increasing trend in the number of days with high health-risk CHDEs in the northwest and north China regions.
Additionally, we assess the projected number of emergency cases attributed to future high health-risk CHDEs and CHWEs. The results indicate that, compared to the past 30 years, the impact of high health-risk CHWEs and CHDEs on emergency cases in China will increase significantly in the future (Supplementary Fig. S7, 8). This impact, previously concentrated mainly in the southeastern regions, is projected to extend significantly to the northwestern regions. Furthermore, under high-emission climate scenarios, the severity of these impacts is expected to escalate.
Discussion and conclusions
In the conventional approach to studying compound events, meteorological thresholds have conventionally served as the primary basis. In our research, however, we introduce a unique perspective by incorporating emergency ambulance dispatch data into our threshold considerations—a distinctive feature that sets our research apart. High health-risk events occurred when T exceeded the 80th percentile, and RH fell below the 10th percentile (CHDEs), or when T surpassed the 90th percentile with RH above the 55th percentile (CDWEs). Utilizing the high health-risk threshold highlights that relying solely on T standards without considering RH may underestimate the health risks of compound extreme events on populations.
Unlike single-variable methods, our approach comprehensively considers multiple extreme drivers and their health impacts (ambulance dispatch data). By using probability statistic indicators based on joint distributions, we capture the dependency and interaction effects of CHDEs and CHWEs. This method is versatile and adaptable to China’s diverse climate, making it more practical than absolute thresholds. Our health-relevant thresholds for temperature and RH are consistent with previous studies, ensuring reliability and relevance41,42,43.
Examining the climatology and linear trends of high health-risk CHDEs and CHWEs in China from 1979 to 2014 using ERA5 data during the warm season, we observe distinct geographical patterns. The northwestern region and middle-lower reaches of the Yangtze River show the highest occurrence of high-health-risk CHDEs, while the Qinghai-Tibet Plateau and Northeastern region experience more high-health-risk CHWEs. Notably, these high-incidence areas align with regions of rapid growth. A monthly analysis reveals that high health-risk CHDEs peak in May and June, while high health-risk CHWEs are most prevalent in July and August. These findings highlight the contrasting effects of human activities on high health-risk CHDEs and CHWEs, particularly in the middle and lower reaches of the Yangtze River region. We speculate that these patterns may result from a combination of climate and weather patterns, rapid urbanization and land use changes, and natural climate variability such as ENSO and the East Asian Monsoon26,28,44,45.
Our study, based on CMIP6 data, reveals a robust spatial correlation (≥0.80) in simulated ensemble means. The observed warm-season national averages correlate well with simulations, indicating that the models accurately capture variability in high health-risk CHDEs and CHWEs. In a carbon-neutral scenario, the frequency of high health-risk CHDEs and CHWEs caused by human activities is reduced by one-half and one-fifth, respectively, compared to SSP-5.85. Human activities are projected to reduce the occurrence of high health-risk CHWEs in eastern China in the future. Conversely, there is an increasing trend in the number of days with high health-risk CHDEs in the northwest and north China regions.
In addition, defining extreme weather events and establishing appropriate impact-based thresholds is crucial. For instance, severe drought can cascade across multiple socio-environmental systems, such as wildfires46, water scarcity47, crop yield and livestock losses48, and conflicts49. The combined impact of co-occurring precipitation deficits and warm periods has been shown to reduce annual or decadal-scale runoff or river flow50,51,52.
Our study underscores the critical need for integrated approaches that consider both meteorological thresholds and health impacts, emphasizing the importance of tailored public health strategies and urban planning to mitigate the health risks associated with compound extreme events. However, this study selectively analyzes a few cities, which limits the generalizability of findings to other countries or regions due to variations in climate, social environments, and behavioral patterns. Caution is advised when extrapolating conclusions, such as health risks and meteorological thresholds, to different contexts43,53. Given the diverse mechanisms through which T impacts various diseases and populations, careful consideration is necessary when applying these thresholds or exposure characteristics to assess extreme T effects on other health outcomes (e.g., mortality, hospitalization risk)54,55.
In future research, a comprehensive evaluation of health impacts arising from compounded meteorological factors and extreme T exposure is imperative. Identifying high health-risk meteorological exposure patterns is essential for guiding the development of health meteorological services. Multi-center studies and investigations into T-related health impacts within various urban zones are warranted56. Strengthening research on the modifying effects of environmental and socioeconomic factors on T health effects is crucial. Elucidating the mechanistic pathways of T health impacts will aid in understanding regional high health-risk characteristics, facilitating the development of targeted regional prevention and control strategies.
Materials and methods
Ambulance dispatches data and health-risk assessment
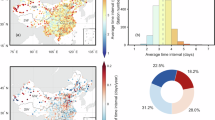
This study focuses on utilizing ambulance dispatch data as indicators of health outcomes. Ambulance dispatch data offer nearly real-time insights into incidences, which makes them faster and more accurate compared to weather warning systems based on mortality or hospital admission data. Hence, it’s important to understand the health risks associated with both T and RH. We analyzed the relationship between T and ambulance dispatches to identify T-RH combinations significantly associated with health impacts. Specifically, through regression analysis, we determined how ambulance dispatch rates vary under specific T and RH conditions, thereby identifying thresholds indicative of elevated health risks. Daily records of emergency ambulance dispatch in each city were obtained from the Ambulance Service Centers, which collect ambulance dispatch information for the whole city, covering the longest time span of 2013–2019. The population, number of emergency cases, and incidence rates for the 13 cities included in this study are detailed in Supplementary Table S1. Based on demographic data for the study period, the total population of the 13 cities is approximately 79.11 million people, with a total of 2.5 million emergency cases. The annual average number of emergency cases is 673,000, and the average incidence rate is 1302 cases per ten thousand people.
After accounting for long-term trends, seasonal variations, day-of-week effects, and holidays and adjusting for the combined influence of T and RH on health effects, we establish a correlation between daily mean T and ambulance dispatches. We utilize RR to quantify the health risk associated with T fluctuations. RR indicates the likelihood of an event occurring in one group (e.g., ambulance dispatches) compared to another group (e.g., average baseline), providing insights into T-related health hazards.
Observations and Simulations
We used daily T and RH observations from 1979 to 2022 obtained from the European Center for Medium-Range Weather Forecast (ECMWF). The ERA5 reanalysis provided hourly data at a 0.25° × 0.25° spatial resolution on a reduced Gaussian grid (https://www.ecmwf.int/en/forecasts/datasets/reanalysis-datasets/era5/). Here, RH serves as a consistent standard for comparing moisture levels across varied temperatures and locations, addressing the complexity of absolute humidity’s T dependence. Its widespread use facilitates practical applications and large-scale analyses, unlike the more intricate data acquisition and processing required for absolute humidity. Combining T and RH enhances assessments of health impacts, crucial for understanding thermal environments and nonlinear T-RH interactions. This approach, supported by relevant studies57, provides a robust framework for evaluating humidity’s effects on human health.
We employed historical simulations under ALL and NAT from 10 models taking part in the Detection and Attribution Model Intercomparison Project (DAMIP) in the Coupled Model Intercomparison Project Phase 6 (CMIP6; see Supplementary Table S2; https://aims2.llnl.gov/search/cmip6/)58. In this study, we only utilized future emission simulations known as the SSP-2.45, as it is the only source providing T and RH data for both ALL and NAT. We bilinearly interpolated all datasets to a 0.5° × 0.5° spatial resolution for analysis.
Attribution analysis
The anthropogenic impact is evaluated by comparing spatial and temporal changes in simulations that include and exclude anthropogenic forcings with those observed. In particular, if the evolving pattern of observations aligns with that of ALL simulations but contradicts that of NAT simulations, the observed changes can be attributed to anthropogenic forcings. The contribution of anthropogenic forcings to the probability can be quantified based on PR and FAR. The corresponding equations are expressed as
where \({P}_{{ALL}}\) and \({P}_{{NAT}}\) are the probability of CDHEs/CHWEs occurrences in the ALL and NAT simulations, respectively. Specifically, PR indicates changes in the probability of extreme events, and FAR quantifies the fraction attributable to anthropogenic forcing59. The 95% CI was obtained by using 1000 bootstrap resampling.
We specifically used the SSP-2-4.5 and SSP-2-4.5nat scenarios from the CMIP6 multi-model ensemble. The SSP-2-4.5 scenario includes both natural and anthropogenic forcings, while the SSP-2-4.5nat scenario includes only natural forcings. The contribution of human activities is then quantified by the difference in event occurrence probabilities between these two scenarios:
where \({P}_{{ANT}}\) represents the change in probability due to human activities. This method allows us to directly attribute changes in the frequency of high health-risk CHDEs and CHWEs to human activities. With the advantage of being simple and direct, making it particularly suitable for analyzing multi-model ensemble data and comparing different future scenarios.
The definition of high health-risk CHDEs/CHWEs
Previous research has employed specific relative thresholds, such as the 10th and 90th percentiles (alternatively, 25th and 75th percentiles), to indicate the thresholds for compound events defined by the combination of T and RH60,61. However, these meteorological thresholds have not been explicitly linked to health-related outcomes.
Our study rigorously defines high health-risk thresholds, elaborated in Supplementary Fig. S1, featuring a comprehensive flowchart and detailed explanations. Moreover, we investigate the RR associated with ambulance dispatches during compound T and RH events in China, as depicted in Fig. 1. Sensitivity analyses to test the robustness of the identified temperature-humidity combinations are provided in Supplementary Table S3.
We delineate that high health-risk CHDEs occur when T is at or above the 80th percentile, coupled with RH at or below the 10th percentile. Conversely, high health-risk CDWEs occur when the T reaches or exceeds the 90th percentile, accompanied by RH at or above the 55th percentile, with a minimum of 70%. Our method considers multiple extreme drivers’ interactions and impacts on health outcomes, using ambulance dispatch data. We employ probability statistics to identify high health-risk compound events, favoring relative thresholds for their adaptability to China’s diverse climate. These thresholds are consistent with prior research suggesting that RH levels above the 55th percentile contribute to heightened health risks, particularly in terms of physiological survival thresholds, skin health, and perceived indoor air quality41. Additionally, low humidity environments indoors have been associated with exacerbating eczema symptoms and dry skin, while interventions to increase humidity show promise in improving skin barrier function42,43.
Moreover, our findings shed light on the discrepancy between previous studies and high health-risk thresholds, revealing a significant underestimation of the risk zones impacting human health in China (see Supplementary Figs. S2, 3 and Tables S4–7). For instance, there are more occurrences of CHDEs in the Northwest and the middle to lower reaches of the Yangtze River region in China, as well as more incidents of CHWEs in the Qinghai-Tibet Plateau and the Northeast region. Significantly, this indicates that, by utilizing the high health-risk threshold, it highlights that relying solely on T standards without considering RH may underestimate the health risks of compound extreme events on populations.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The climate model simulations are available via the Earth System Grid Federation archive of Coupled Model Intercomparison Project 6 data (https://esgf-index1.ceda.ac.uk/projects/esgf-ceda/). The ECMWF ERA5 reanalysis data set was downloaded from https://www.ecmwf.int/en/forecasts/datasets/reanalysis-datasets/era5. Daily records of emergency ambulance dispatch in each city were obtained from the Ambulance Service Centers, but restrictions apply to the availability of these data, which were used under license for the current study and so are not publicly available.
Code availability
All code used in this study is available upon request from the corresponding author.
References
Zscheischler, J. et al. Future climate risk from compound events. Nat. Clim. Change 8, 469–477 (2018).
IPCC. (2021). In V. Masson-Delmotte, P. Zhai, A. Pirani, S. L. Connors, C. Péan, S. Berger, et al. (Eds.), Climate change 2021: the physical science basis. Contribution of working group I to the sixth assessment report of the intergovernmental Panel on climate change. Cambridge University Press. In press. https://doi.org/10.1017/9781009157896.
Zscheischler, J. & Lehner, F. Attributing compound events to anthropogenic climate change. Bull. Am. Meteorol. Soc. 103, 936–953 (2022).
Zaitchik, B. F., Rodell, M., Biasutti, M. & Seneviratne, S. I. Wetting and drying trends under climate change. Nat. Water 1, 502–513 (2023).
Hao, Z., Hao, F., Singh, V. P. & Zhang, X. Statistical prediction of the severity of compound dry-hot events based on El Niño-Southern oscillation. J. Hydrol. 572, 243–250 (2019).
Wang, L., Xia, E., Wei, Z. & Wang, W. Exploring the driving forces on sustainable energy and water use in China. Environ. Sci. Pollut. Res. Int. 29, 7703–7720 (2022).
Ghanbari, M., Arabi, M., Georgescu, M. & Broadbent, A. M. The role of climate change and urban development on compound dry-hot extremes across US cities. Nat. Commun. 14, 3509 (2023).
Liu, J. et al. Heat exposure and cardiovascular health outcomes: a systematic review and meta-analysis. Lancet Planet. Health 6, 484–495 (2022).
Asseng, S., Spänkuch, D., Hernandez-Ochoa, I. M. & Laporta, J. The upper temperature thresholds of life. Lancet Planet. Health 5, 378–385 (2021).
Ahmed, T. & Wang, C. K. Black garlic and its bioactive compounds on human health diseases: a review. Molecules (Basel, Switz.) 26, 5028 (2021).
Guarnieri, G., Olivieri, B., Senna, G. & Vianello, A. Relative humidity and its impact on the immune system and infections. Int. J. Mol. Sci. 24, 9456 (2023).
Monintja, T. C. N., Arsin, A. A., Amiruddin, R. & Syafar, M. Analysis of temperature and humidity on dengue hemorrhagic fever in Manado municipality. Gac. Sanit. 35, 330–333 (2021).
Duque, C. et al. Impact of aerial humidity on seasonal malaria: an ecological study in Zambia. Malar. J. 21, 325 (2022).
Edillo, F., Ymbong, R. R., Navarro, A. O., Cabahug, M. M. & Saavedra, K. Detecting the impacts of humidity, rainfall, temperature, and season on chikungunya, dengue and Zika viruses in Aedes albopictus mosquitoes from selected sites in Cebu city, Philippines. Virol. J. 21, 42 (2024).
Baldwin, J. W. et al. Humidity’s role in heat-related health outcomes: a heated debate. Environ. Health Perspect. 131, 55001 (2023).
Hao, Z. et al. A multivariate approach for statistical assessments of compound extremes. J. Hydrol. 565, 87–94 (2018).
McKinnon, K. A., Poppick, A. & Simpson, I. R. Hot extremes have become drier in the United States Southwest. Nat. Clim. Change 11, 598–604 (2021).
Yaddanapudi, R., Mishra, A., Huang, W. K. & Chowdhary, H. Compound wind and precipitation extremes in global coastal regions under climate change. Geophys. Res. Lett. 49, e2022GL098974 (2022).
Pan, R., Li W., Wang, Q., Ailyaer, A. Detectable anthropogenic intensification of the summer compound hot and dry events over global land areas. Earth’s Future 11 (2023).
Chen, L., Chen, X., Cheng, L., Zhou, P. & Liu, Z. Compound hot droughts over China: identification, risk patterns and variations. Atmos. Res. 277, 210–219 (2019).
Li, Y., Ding, Y. & Li, W. Observed trends in various aspects of compound heat waves across China from 1961 to 2015. J. Meteorol. Res. 31, 455–467 (2017).
Chen, Y., Liao, Z., Shi, Y., Tian, Y. & Zhai, P. Detectable increases in sequential flood-heatwave events across china during 1961-2018. Geophys. Res. Lett. 48, e2021GL092549 (2021).
Yu, Y. et al. Compound climate extremes in China: trends, causes, and projections. Atmos. Res. 286, 106675 (2023).
Zhao, L. et al. Human activity and simultaneous high-pressure anomalies influence the long-duration cold events of winter in China. Clim. Dyn. 61, 2765–2781 (2023).
Martius, O., Pfahl, S. & Chevalier, C. A global quantification of compound precipitation and wind extremes. Geophys. Res. Lett. 43, 7709–7717 (2016).
Su, Q. & Dong, B. Recent decadal changes in heat waves over china: drivers and mechanisms. J. Clim. 32, 4215–4234 (2018).
Du, J., Wang, K. & Cui, B. Attribution of the extreme drought-related risk of wildfires in spring 2019 over Southwest China. Bull. Am. Meteorol. Soc. 102, 83–90 (2021).
Ma, F. C. & Yuan, X. More persistent summer compound hot extremes caused by global urbanization. Geophys. Res. Lett. 48, e2021GL093721 (2021).
Wang, J. et al. Anthropogenic emissions and urbanization increase risk of compound hot extremes in cities. Nat. Clim. Change 11, 1084–1089 (2021).
Li, W. et al. Anthropogenic impact on the severity of compound extreme high temperature and drought/rain events in China. npj Clim. Atmos. Sci. 6, 1–13 (2023).
Stott, P. A. et al. Attribution of extreme weather and climate-related events. WIREs Clim. Change 7, 23–41 (2016).
King, A. D., van Oldenborgh, G. J., Karoly, D. J., Lewis, S. C. & Cullen, H. Attribution of the record high Central England temperature of 2014 to anthropogenic influences. Environ. Res. Lett. 10, 054002 (2015).
Sun, Q. H., Miao, C. Y., AghaKouchak, A. & Duan, Q. Y. Unraveling anthropogenic influence on the changing risk of heat waves in China. Geophys. Res. Lett. 44, 5078–5085 (2017).
Trenberth, K., Fasullo, J. & Shepherd, T. Attribution of climate extreme events. Nat. Clim. Change 5, 725–730 (2015).
Chiang, F., Greve, P., Mazdiyasni, O., Wada, Y., & Aghakouchak, A. A multivariate conditional probability ratio framework for the detection and attribution of compound climate extremes. Geophys. Res. Lett. 48, (2021).
Qian, C., Ye, Y., Bevacqua, E. & Zscheischler, J. Human influences on spatially compounding flooding and heatwave events in China and future increasing risks. Weather Clim. Extremes 42, 100616 (2023).
Smith, K. R. et al. The last Summer Olympics? Climate change, health and work outdoors. Lancet 388, 642–644 (2016).
Lenton, T. M. et al. Quantifying the human cost of global warming. Nat. Sustain. 6, 1237–1247 (2023).
Fricko, O. et al. The marker quantification of the shared socioeconomic pathway 2: a middle-of-the-road scenario for the 21st century. Glob. Environ. Change 42, 251–267 (2017).
Li, L. et al. Mitigation of China’s carbon neutrality to global warming. Nat. Commun. 13, 5315 (2022).
Fang, W. et al. The joint and interaction effect of high temperature and humidity on mortality in China. Environ. Int. 171, 107669 (2023).
Goad, N. & Gawkrodger, D. J. Ambient humidity and the skin: the impact of air humidity in healthy and diseased states. J. Eur. Acad. Dermatol. Venereol. 30, 1285–1294 (2016).
Wolkoff, P. Indoor air humidity, air quality, and health - an overview. Int. J. Hyg. Environ. Health 221, 376–390 (2018).
Wang, J., Feng, J., Yan, Z. & Chen, Y. Future risks of unprecedented compound heat waves over three vast urban agglomerations in China. Earth’s. Future 8, e2020EF001716 (2020).
Wang, B. et al. Spatiotemporal trends of extreme temperature events along the qinghai-tibet plateau transportation corridor from 1981 to 2019 based on estimated near-surface air temperature. J. Geophys. Res.: Atmos. 128, e2023JD039040 (2023).
Mukherjee, S., Mishra, A. K., Mann, M. E. & Raymond, C. Anthropogenic warming and population growth may double US heat stress by the late 21st century. Earth’s. Future 9, e2020EF001886 (2021).
Veettil, A. V. & Mishra, A. K. Water security assessment using blue and green water footprint concepts. J. Hydrol. 542, 589–602 (2016).
Feng, S., Hao, Z., Zhang, X. & Hao, F. Changes in climate-crop yield relationships affect risks of crop yield reduction. Agric. For. Meteorol. 304, 108401 (2021).
García-Herrera, R., Díaz, J., Trigo, R. M., Luterbacher, J. & Fischer, E. M. A review of the european summer heat wave of 2003. Crit. Rev. Environ. Sci. Technol. 40, 267–306 (2010).
Brunner, M. I., Swain, D. L., Gilleland, E. & Wood, A. W. Increasing importance of temperature as a contributor to the spatial extent of streamflow drought. Environ. Res. Lett. 16, 024038 (2020).
Hettiarachchi, S., Wasko, C. & Sharma, A. Do longer dry spells associated with warmer years compound the stress on global water resources? Earth’s. Future 10, e2021EF002392 (2022).
Mastrotheodoros, T. et al. More green and less blue water in the Alps during warmer summers. Nat. Clim. Change 10, 155–161 (2020).
Issa, M. A. et al. A heat-health watch and warning system with extended season and evolving thresholds. BMC Public Health 21, 1479 (2021).
Yang, Z., Wang, Q. & Liu, P. Extreme temperature and mortality: evidence from China. Int. J. Biometeorol. 63, 29–50 (2019).
Ebi, K. L. et al. Hot weather and heat extremes: health risks. Lancet (Lond., Engl.) 398, 698–708 (2021).
Yang, J. et al. Projecting heat-related excess mortality under climate change scenarios in China. Nat. Commun. 12, 1039 (2021).
Bourdin, S., Kluft, L. & Stevens, B. Dependence of climate sensitivity on the given distribution of relative humidity. Geophys. Res. Lett. 48, e2021GL092462 (2021).
O’Neill, B. C. et al. The scenario model intercomparison project (ScenarioMIP) for CMIP6. Geosci. Model Dev. 9, 3461–3482 (2016).
Fischer, E. M. & Knutti, R. Anthropogenic contribution to global occurrence of heavy-precipitation and high-temperature extremes. Nat. Clim. Change 5, 560–564 (2015).
Peng, T. et al. Changes in temperature‐precipitation compound extreme events in China during the past 119 years. Earth Space Sci. 10, e2022EA002777 (2023).
Lin, X., Wang, Y., & Song, L. (2024). Urbanization amplified compound hot extremes over the three major urban agglomerations in China. Geophys. Res. Lett. 51 (2024).
Acknowledgements
We thank the reviewers and editor for their insightful remarks. The authors thank ECMWF for providing ERA5 reanalysis and the Chinese Ambulance Service Centers for providing ambulance dispatch information. This research was funded by the National Natural Science Foundation of China (42075040), Research Fund (2024ZZ004) of Tsinghua University Vanke School of Public Health, the National Key Research and Development Program of China (2018YFA0606200), Guangdong Major Project of Basic and Applied Basic Research (2020B0301030004), the Strategic Priority Research Program of the Chinese Academy of Sciences (XDA23090102) and the Postgraduate Research & Practice Innovation Program of Jiangsu Province (KYCX24_1420).
Author information
Authors and Affiliations
Contributions
H.Y., L.Z., X.S., and C.H. conceived and designed the study. H.Y. and L.Z. performed the analysis, drew all figures, and wrote the first draft of the paper. Y.H. and W.D. processed the data. X.S., J.W., Y.H., J.L., and Z.X. provided suggestions and discussed the results.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Communications Earth & Environment thanks the anonymous reviewers for their contribution to the peer review of this work. Primary Handling Editor: Alireza Bahadori. A peer review file is available
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yao, H., Zhao, L., He, Y. et al. Changes caused by human activities in the high health-risk hot-dry and hot-wet events in China. Commun Earth Environ 5, 464 (2024). https://doi.org/10.1038/s43247-024-01625-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s43247-024-01625-y
