
Abstract
Longevity research aims to extend the healthspan while minimizing the duration of disability and morbidity, known as the sickspan. Most longevity interventions in model organisms extend healthspan, but it is not known whether they compress sickspan relative to the lifespan. Here, we present a theory that predicts which interventions compress relative sickspan, based on the shape of the survival curve. Interventions such as caloric restriction that extend mean lifespan while preserving the shape of the survival curve, are predicted to extend the sickspan proportionally, without compressing it. Conversely, a subset of interventions that extend lifespan and steepen the shape of the survival curve are predicted to compress the relative sickspan. We explain this based on the saturating-removal mathematical model of aging, and present evidence from longitudinal health data in mice, Caenorhabditis elegans and Drosophila melanogaster. We apply this theory to identify potential interventions for compressing the sickspan in mice, and to combinations of longevity interventions. This approach offers potential strategies for compressing morbidity and extending healthspan.
Similar content being viewed by others

Introduction
The lifespan of an individual typically begins with a period of general health, called the healthspan, followed by a period of intermittent or continuous morbidity and disability called the sickspan1,2,3. The sickspan burdens human quality of life and is a growing driver of economic expenditure across societies4,5,6.
Understanding what sets lifespan, and how to extend it, is a central goal of longevity research. There are several possible scenarios of lifespan extension regarding sickspan4. In principle, a longevity intervention could expand morbidity, and in the extreme case extend the sickspan exclusively, which is clearly undesirable. Alternatively, both healthspan and sickspan could be simply “stretched” in proportion to lifespan. Finally, as proposed in the field of gerontology1,2,3, one could ideally aim to compress morbidity. Sickspan can be compressed either in absolute terms, as advanced by Fries7, or relative to lifespan8, as in the dynamic equilibrium concept by Manton in which both healthspan and lifespan are extended by similar absolute amounts9. It is generally thought that optimal aging trajectories should restrict morbidity to a brief period before death3,7.
Research has identified diverse interventions that can extend lifespan in model organisms including yeast, nematodes, flies and mice10,11,12,13,14. These include dietary restriction15,16, perturbations of the IGF1 pathway17, mTOR inhibition by drugs such as rapamycin18,19, senolytic treatments20,21,22, in vivo partial reprogramming23,24, and additional classes of drugs including antioxidants and diabetic drugs25.
These longevity interventions are developed to also delay morbidity in model organisms - the treated animals are usually reported to have better health parameters than equally aged untreated animals as measured at a single time point11. However, whether they compress the sickspan in absolute or relative terms has not generally been reported. Data from Caenorhabditis elegans suggests that many interventions that extend lifespan extend sickspan proportionally26,27, and thus do not compress morbidity in absolute or relative terms. A similar effect has been seen in medflies28. Notably, however, data from intervention studies that longitudinally follow health at many timepoints is rare, and thus the question of sickspan relative to lifespan is understudied.
It is thus of interest to identify which longevity interventions are likely to compress sickspan, and which instead have the unintended consequence of extending it. Identifying factors that affect the relative healthspan and sickspan in model organisms would improve our basic understanding of the biology of aging and age-related morbidity and inform the search for healthspan-extending therapies.
Here we present a theory that can predict which longevity interventions compress sickspan. The theory is based on the survival curve, the fraction of organisms that survive to a given age29. Many longevity interventions that extend median lifespan preserve the shape of this curve, a phenomenon called scaling26,30,31,32. We predict that such interventions extend sickspan proportionally. In contrast, a small number of interventions extend median lifespan and steepen the survival curve, making its shape more rectangular. We predict that these interventions compress the sickspan (with certain exceptions discussed below).
Here we show that this theory arises naturally from a recent mathematical model of aging called the saturating-removal model that was calibrated in mice, invertebrates and single celled organisms32,33,34,35. We provide evidence from nematode, fly and mice data that steepening interventions compress relative sickspan. We discuss specific mice longevity interventions that steepen the survival curve as candidate interventions to compress sickspan, and their potential mechanisms, and apply the theory to combinations of longevity interventions and to human data.
Results
The saturating-removal model links the shape of the survival curve with the parameter of damage dynamics
Longevity-enhancing interventions shift the survival curve to greater ages, increasing the median survival age t50 (Fig. 1a). They often preserve the curve shape, a phenomenon called scaling (Fig. 1b)26,30,31. Interventions are said to be scaling if their survival curves collapse onto the control survival curve when age is normalized by the median lifespan (Fig. 1b, upper panel; To test statistically for scaling of empirical survival curves throughout the present study, we use a version of Kolmogorov–Smirnov after rescaling by accelerated failure time model30,36, see “Methods”). Scaling interventions increase median and maximal lifespan by the same factor. Scaling was discovered by Stroustrup and colleagues in C. elegans30, and later described in budding yeast31.

a Survival curves describe the fraction of organisms surviving to each age; median age t50 is extended by longevity interventions. b Scaling is defined by survival curves collapsing on the same curve when time is re-normalized30. Steepening occurs when the intervention’s survival curve has higher steepness than control. c The saturating-removal model posits a damage X that drives aging whose production rate rises with age and whose removal rate saturates with damage, with noise. Simulations (black and blue lines) show stochastic trajectories of two individuals that cross the death threshold Xc at different times. d Effect of a twofold change in each model parameter on survival curve shape. e Effect of parameter changes on t50 and steepness defined as mean divided by standard deviation compared to baseline (control). Baseline parameters for mice are η = 2.3 × 10−4/day2, β = 0.15 /day, κ = 0.5, ε = 0.16/day, Xc = 1732.
For example, median C. elegans lifespan increases at low temperatures, but survival curves scale to a good approximation. Caloric restriction also extends lifespan15,16,37, as reviewed by Fontana, Partridge, and Longo16, but survival curves scale approximately.
Other interventions increase median lifespan but steepen the survival curve shape (Fig. 1b, lower panel)30,38. A useful metric for steepness is the mean lifespan divided by the standard deviation of lifespan29 (see Methods for details and Supplementary Information for alternative definitions of steepness).
Interventions that extend lifespan and scale the survival curve seem to stretch the time axis as if time is slowed down. They may therefore be considered intuitively to slow down the overall pace of aging. We hypothesize that they should accordingly slow down the processes responsible for age-related morbidity and functional decline. The result is a proportional scaling of the sickspan and healthspan. Relative sickspan, that is the sickspan divided by lifespan, should remain unchanged by the intervention.
To quantitatively test this intuition, we use the saturating-removal (SR) mathematical model for aging dynamics32,34,35 (Fig. 1c). The SR model describes the dynamics of damage that is posited to be causal for both morbidity and mortality. The SR model is a stochastic differential equation39 whose mathematical form was deduced from dynamic data on mouse senescent cells. Its predictions were tested experimentally in mice32 and in longitudinal damage measurements in microorganisms35. The model was further validated by comparison to quantitative datasets on age-related diseases in humans34, parabiosis in mice33, and midlife longevity interventions in Drosophila32.
The key simplifying assumption in the model is the existence of a driving damage denoted X which is upstream of morbidity and mortality. The model is agnostic to the exact nature of X and thus can apply to different organisms. The model is a stochastic differential equation for X that accounts for production, removal, and noise: dX/dt = production − removal + noise, whose equation is shown in Fig. 1c.
The driving damage X rises with age and fluctuates around this rising trend on a timescale that is fast compared to the lifespan. It is produced in the model by damage-producing units that are not removed and accumulate linearly with age (Fig. 1c). The rate of production is therefore proportional to age, namely production = ηt. The driving damage is removed by processes that saturate at high damage levels. This is modeled as Michaelis–Menten-like saturation, removal = βX/(κ + X), where β is the maximal removal rate and κ the halfway saturation point. The noise is modeled as white noise with amplitude ε (Fig. 1c)
Death is modeled to occur when driving damage X crosses a mortality threshold Xc. Simulating the model shows that each individual has a stochastic trajectory of damage X (Fig. 1c). Each individual therefore crosses the death threshold Xc at a different time. The risk of death in the model rises exponentially with age and slows at very old ages32—this is the Gompertz law found in many species, including humans. The survival curves are sigmoidal in shape (well-described by Weibull distributions) and resemble empirical survival curves32.
A key feature of the SR model is its ability to provide scaling of survival curves32. Changes in the rate of damage production, namely the parameter η, shift median survival but preserve the shape of the curve (Fig. 1d), providing near-perfect scaling.
Changing any of the other model parameters, such as removal rate β, affects not only lifespan but also the shape of the survival curve (Fig. 1d). Increasing damage removal rate β shifts the survival curve to the right and steepens it. Increasing death threshold Xc mildly extends median lifespan and steepens the curve by preventing early deaths. Decreasing the noise amplitude ε causes a small increase in lifespan and a large increase in steepness—less noise leads to more deterministic death times. These effects are shown on a steepness-longevity plot in Fig. 1e, and separately for steepness and longevity in Supplementary Fig. 1.
The reason that these parameters all affect steepness is that the shape of the survival curve in the model is essentially determined by a single dimensionless parameter βXc/ε. Note that production rate η does not appear in this dimensionless group. It affects lifespan but not the shape of the curve and so changes in η preserve scaling.
Interventions that steepen the survival curve compress relative sickspan in the saturating-removal model
Our main interest in this study is sickspan. Hence, we add morbidity to the model in order to study sickspan and healthspan. Age-related morbidity is modeled to occur when X crosses a morbidity threshold Xd (Fig. 2a). This simple model captures the incidence of hundreds of age-related diseases in humans, as shown by Katzir et al.34. Each disease has its own threshold. Here we consider sickspan as an aggregate phenomenon that occurs when a threshold is crossed that is an average of the different disease thresholds weighted by their prevalence. The probability of crossing Xd rises exponentially with age until it slows at very old ages.

a Trajectories of damage X for two simulated individuals. Sickspan is the period after first crossing the disease threshold Xd and before crossing the death threshold Xc. b Simulation of untreated individuals and two treatments that extend median lifespan by the same amount: reduced production η by 46% or increased removal β by 90%. Simulations of 200 individuals are shown in two ways: left, ranked by lifespan versus age (survival curve); right, ranked by relative sickspan as function of fraction of life lived. Red indicates the sickspan, yellow indicates the healthspan and gray indicates death. c Absolute sickspan (intervention/control) as a function of median lifespan for changes in different model parameters. d Relative sickspan (sickspan/lifespan) as a function of model parameters. Baseline parameters are as in Fig. 1 with Xd = 12.
We thus consider here a definition of sickspan as a continuous end-of-life period that begins upon the first crossing of Xd. This aligns with current definitions in model organisms of an end-of-life period of morbidity when severe health deficits cross a threshold26,40,41,42. An alternative definition would allow for sickspan to be intermittent when X drops below Xd for sufficient time. Such a definition requires additional parameters and assumptions, and we leave it for future study.
We tested the effect of changing model parameters on the relative sickspan. We find that changes in production rate η that scale the survival curve also approximately scale the relative sickspan—and in fact slightly prolong it (Fig. 2b–d).
In contrast, sickspan is compressed by most longevity changes that steepen the survival curve. Increasing removal rate β compresses the relative sickspan (Fig. 2b–d), as does a reduction in noise ε or increasing both disease and death thresholds together (Fig. 2c, d). In these interventions, longevity is increased primarily by extending the healthspan.
There is one exception to the rule that interventions that steepen survival curves compress relative sickspan. This occurs when the death threshold Xc rises but the disease threshold Xd does not (Fig. 2c, d, green lines). This might apply to human data when medical care extends life in sick individuals, without affecting age of onset of sickspan. We discuss human mortality in the last section.
In summary, longevity interventions have differential effects on relative sickspan depending on which parameters they affect in the model. Changes in damage production rate η—the only changes that scale the survival curve—increase absolute sickspan and mildly increase relative sickspan. In contrast, interventions that extend lifespan and steepen the survival curve generally compress the relative sickspan. They extend lifespan primarily by extending healthspan.
Steepening interventions compress relative sickspan in invertebrates and mice
To test whether steepening of the survival curve indeed implies a compressed sickspan, we analyzed data from experiments which followed health longitudinally as organisms aged under different interventions. These experiments were performed in mice, Drosophila melanogaster and Caenorhabditis elegans. In all cases, we used the authors’ definition of sickspan.
Data on longitudinal health in mice is currently limited, although it is expected to be available from several ongoing experiments43,44,45. We analyzed data from Luciano et al.42 which followed mouse frailty index longitudinally in different longevity interventions. The experiment included dietary interventions (20% and 40% calorie restriction and two intermittent fasting schedules) in two strains (Diversity Outbred and C57BL/6). Sickspan was defined by the authors as periods of life with 4 or more age-related deficits in the mouse frailty index.
We evaluated the survival curve steepness relative to control for these experiments and compared it to the relative sickspan (mean absolute sickspan divided by mean lifespan, relative to control). Steepness was defined by removing the 10% shortest lifespans and computing the mean lifespan divided by the standard deviation of lifespans (inverse trimmed coefficient of variation, or iTCV, see Supplementary Information for an alternative definition of steepness)29. We calculate confidence intervals of both relative sickspan and steepness by bootstrap resampling of individuals.
We find that relative sickspan decreased with steepness as predicted (Fig. 3a and Supplementary Table 1). Scaling interventions (steepness intervention/control of 1) showed approximately scaled sickspan (Fig. 3a). These findings agree with the SR model predictions. The relationship is robust to the definition of sickspan (Supplementary Fig. 2), and the definition of steepness (Supplementary Figs. 3 and 4).

Mean absolute sickspan divided by mean lifespan relative to control is plotted versus steepness of survival curve relative to control. a Mice under dietary longevity interventions—caloric restriction and intermittent fasting—in two strains from Luciano et al.42. Sickspan was defined using mouse frailty index. See Supplementary Table 1 for intervention details. b Nutritional longevity interventions in two strains of D. melanogaster, where sickspan was defined by deficits in climbing, jumping and flying in response to a mechanical challenge. Data from Gaitanidis et al.40. See Supplementary Table 2 for intervention details. c Genetic longevity mutants in C. elegans, where sickspan was defined by loss of muscle power measured by piezoelectric challenge. Data from Statzer et al.26. See Supplementary Table 3 for strain details. d Genetic, dietary and environmental factors in C. elegans, where sickspan was measured by secession of spontaneous movements. Data from Stazer et al.26 and Oswal et al.41. See Supplementary Table 4 for strain and intervention details. From (a–d), each cross indicates an intervention cohort. Error bars represent mean +/− SEM, which are calculated using bootstrap resampling of individuals in each cohort. Dark blue and light blue represent linear trends of the data and their 95% confidence interval. The 95% slope confidence intervals are (−2.2, −0.9), (−2.5, −1.2), (−3.8, −0.2), (−1.2, −0.2) for (a–d), respectively. Source data are provided as a Source Data File.
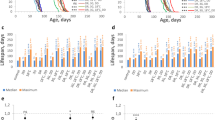
We next considered longitudinal experiments in fruit flies. Carey and colleagues pioneered the use of longitudinal life-history data such as fecundity and mortality to test evolutionary theories of aging46,47,48 using medflies (Ceratitis capitata). More recently, Gaitanidis et al.40 measured longitudinal healthspan data in Drosophila by quantifying age-related declines in motor functions. The authors assayed escape performance in response to gently banging food vials on the counter, i.e., “startle assays”. Each fly was scored for its jumping, climbing, and flying responses to generate a health score for each individual by summing the number of functional deficits. Sickspan was defined as the period where an individual has a score below a threshold value. The experiment was repeated for five dietary interventions (including protein restriction, superfood, and curcumin) in males and females in two fly strains with different lifespans (Lausanne, Oregon).
We computed the survival curve steepness relative to control for these experiments and compared it to the relative sickspan. Relative sickspan decreased with steepness, as predicted (Fig. 3b and Supplementary Table 2). Scaling interventions (steepness/control of 1) showed approximately scaled sickspan (Fig. 3b). These findings agree with the SR model predictions.
We also considered two C. elegans studies. Statzer et al. used a piezoelectric system to measure muscle power cross-sectionally throughout the lifespan26 for five different longevity-affecting mutants: daf-2(e1368), daf-2(e1370), glp-1 and eat-2, and defined sickspan by the period of life when muscle power is below 50% of wild-type. Analysis of this data shows that relative sickspan decreases with steepness (Fig. 3c and Supplementary Table 3).
Another method to define healthspan used the period of spontaneous movements to define the healthspan41. This method was used by both Oswal et al.41 and Statzer et al.26, for several longevity interventions, including temperature, food deprivation, food inactivation by UV, daf-2 (e1368 & e1370), eat-2, glp-1 (both studies), nuo-6 (see Supplementary Table 4 for details of all the intervention and control cohorts). The analysis showed that relative sickspan defined by voluntary movement also decreased with survival curve steepness, as predicted (Fig. 3d). Scaling interventions scaled or slightly expanded relative sickspan.
We conclude that in invertebrates and mice, steepening interventions compress the relative sickspan, whereas scaling interventions approximately scale the sickspan.
Several interventions in mice are predicted to compress sickspan
Whereas longitudinal health data is currently rare, survival curve data of mice under longevity interventions is routinely reported in the literature49. We therefore asked which mouse interventions show scaled survival curves, and which steepen the survival curve36,38.
We explored the 42 nutritional and pharmacological interventions reported by the Interventions Testing Program (ITP)50 of the National Institute on Aging (NIA) (Fig. 4a, Supplementary Data 1, and Supplementary Figs. 5–7). The ITP experiments are standardized lifespan experiments done in three parallel sites with genetically heterogeneous mice and relatively large cohorts49. We also analyzed intervention experiments reported in 32 additional publications, including those with transgenic mice (Fig. 4b, Supplementary Data 2, and Supplementary Fig. 8).

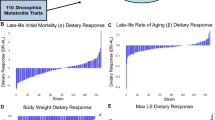
a Longevity and steepness relative to control in all interventions from the NIA Interventions Testing Program (ITP)50. Square and triangle symbols denote female and male mice, respectively. Large empty symbols indicate scaling, and large full symbols indicate non-scaling interventions (based on the AFT + KS30, see “Methods”). Small light symbols indicate interventions whose effects on the survival curve are not statistically significant (Hotelling’s t-squared test, α = 0.05 with Benjamini–Hochberg correction for multiple comparisons). Source data including longevity and steepness uncertainties, and statistical test results of on all NIA ITP interventions are provided as Supplementary Data 1. b Relative longevity and steepness of selected interventions from the literature outside of the ITP, including those based on transgenic mice. Due to the varying sample size and statistical power of the studies analyzed, only interventions that are without counterparts in ITP are shown. See Supplementary Fig. 8 and Supplementary Data 2 for all non-ITP interventions analyzed. Graphic symbols and legends are the same as those in (a). Round symbol denotes a study that only reported mixed sex cohorts. Effect sizes are not directly comparable between the shown interventions and those in NIA ITP because of the differences in controls. c–h Survival curves and rescaled survival curves of steepening interventions (red) and their respective control (black). c Senolytic treatment (genetic ablation of p16 expressing cells)22 in mice from both sexes starting at 12 months of age. d Transgenic VEGF female mice with mildly increased systemic VEGF level via induced production by hepatocytes59. e Acarbose (2500 ppm) in male mice starting at age of 8 months54. f Non-feminizing estradiol 17-α-estradiol (17a-E2) in male mice (14.4 ppm) starting from age of 16 months51. g Hypoglycemic and ketogenic agent 1,3-butanediol (BD) at 100,000 ppm in male mice starting at age of 6 months62. h Angiotensin-converting enzyme inhibitor Captopril (Capt) at 180 ppm in male mice starting from age of 5 months62.
Among the 65 interventions analyzed (42 in NIA ITP, 26 outside of NIA ITP) most did not show significant steepening effects—they showed approximate scaling according to bootstrapping tests (for AFT + KS test P values see Supplementary Data 1 and 2). Confidence intervals are shown in Supplementary Figs. 6 and 7. We identified several classes of interventions that showed significant lifespan increase with steepening survival curves (Fig. 4a, b, Supplementary Figs. 5, 6, and 8). The steepening intervention classes include senolytic treatment, several antioxidants, VEGF overexpression, and, in males only, 17α-estradiol51,52,53, ketogenic diet and hypoglycemic agents such as acarbose52,53,54 and canagliflozin55 (Fig. 4c–h).
In the ITP dataset, acarbose54 and 17α-estradiol51 showed a dose-dependent effect, with both lifespan and steepness increasing with dose. Additional interventions showed steepening with only mild lifespan extension, such as green tea extract (GTE) (females)56 and nordihydroguaiaretic acid (NDGA)57 (males) in the ITP data (Fig. 4a and Supplementary Fig. 9). The antioxidant taurine has a mild steepening effect (Supplementary Fig. 8). High dosage of rapamycin (42ppm in females) causes steepening but is different from other rapamycin data points which show approximate scaling (Fig. 4a and Supplementary Fig. 10).
Senolytic treatments showed life extension and steepening using a genetic approach to ablate cells that express p1622,58. Transgenic production of VEGF showed a 45% life extension and 148% increased steepness for females59 (Fig. 4b and Supplementary Fig. 8). Cyclic ketogenic diet in two separate studies60,61 (Supplementary Fig. 8 and Supplementary Data 2), and a ketogenic dietary supplement62 showed evidence of life extension and steepening for male mice.
The steepening interventions may constitute targets for future measurements of mice sickspan.
Combinations of steepening and scaling interventions show additive effects consistent with the SR model
One application of the present approach concerns combinations of interventions. Intuitively, interventions that affect different pathways, such as damage production and damage removal, should act independently on survival. The SR model helps analyze such interventions—for example, an intervention with scaling and an intervention with steepening are predicted to affect different pathways. Combining a perturbation that scales with one that steepens should therefore provide the best of both worlds—a steep survival curve in which lifespan is extended beyond either individual intervention. This prediction is supported by ITP data on a combination of acarbose (steepening in males) and rapamycin (scaling) administered at 9 months. Longevity was enhanced compared to acarbose or rapamycin alone, and steepness was comparable to the acarbose mono-treatment (Fig. 5). Simulations of the SR model calibrated to these interventions corroborate this phenomenon (Supplementary Fig. 11).

Change in longevity and steepness in the ITP data for acarbose (1000 ppm, starting at 8 months of age), rapamycin (14 ppm, starting at 9 months of age) and their combination (Rap 14.7 ppm + Ac 1000 ppm starting at 9 months of age). a Female mice, b male mice. Ellipses are +/− SEM confidence regions estimated by bootstrapping death times (see “Methods”). Dashed lines and ellipses are additive effects. Source data are provided as a Source Data file.
Steepening of human survival curves is largely due to reduction in extrinsic mortality
The present study primarily aims to understand lab organism data. Considerations in humans are far more complex as compared to model organisms with defined genetics living in controlled environments, because mortality and morbidity are affected by variations in lifestyle, genetics, environment, socioeconomic status and medical care. We therefore provide a tentative account of how the present considerations might apply to human data.
There has been a global trend of rectangularization of human survival curves in the past century7—in many countries, the median lifespan has increased and survival curve steepness has increased as well63 (Fig. 6a). There is a tight correlation between life expectancy and lifespan equality (a measure of steepness)64. There are also exceptions in certain countries in which lifespan variability has increased or remained constant in recent decades63.

a Survival curves and rescaled survival curves of cohorts of Swedish women born in 1820–1824 and 1890–1894. b Hazard curve (death rates by age) of Swedish women born in 1890–1894, and of SR model fitted to this cohort. The SR model parameters that correspond to the blue and orange hazard curves are η = 1.04 × 10−5/day2, β = 0.45 /day, κ = 0.50, ε = 0.48 /day, Xc = 19.932. The extrinsic hazard (additive Makeham term) in the orange curve is m = 0.0036 per year. c–e Mortality component trends of Swedish (Blue), Dutch (Red), French civilians (Green) and English & Welsh civilian (Red) cohorts born 1810–1900. For each 5-year-wide birth cohort, we estimate extrinsic hazard rates, Gompertz slopes and Gompertz intercepts from death rates from age 36 onward, using the Gamma–Gompertz-Makeham model68. In the SR model, the Gompertz slope can be approximated by ηXc/ε and intercept is proportional to eβXc/ε 32. The Gamma–Gompertz correction term s(t) is s(t) =ec/(ec-1 + ebt), where c is an additional parameter that ranges from 7.5 to 10, such that s(t) only comes into effect at old age. Mortality components estimates are presented as mean values +/− SE. The average (min-max) cohort sizes (N) in units of 100,000 for women and men, respectively, are 1.7 (1.2−2.5) and 1.6 (1.2–2.4) for Sweden, 11.0 (6.1–16.7) and 9.8 (5.8–15.5) for England & Wales, 13.7 (12.3–16.1) and 12.9 (7.1–15.9) for France, and 1.7 (1.1–3.2) and 1.7 (1.0–3.1) for Netherlands. Source data are provided as a Source Data file.
Relative sickspan has not been as extensively measured as lifespan, with data accumulating only recently. Available data indicates that relative sickspan since 1980 has compressed in some countries and has grown in others8,65.
We asked whether the rectangularization might be due to changes in SR model parameters, to test whether such changes might predict relative sickspan in each country. To do so, we analyzed human cohort mortality data from the Human Mortality Database (HMD)66. Human data shows a sizable extrinsic mortality that dominates mortality until age 30–40. To account for this, we fitted human hazard curves to the SR model with an added extrinsic mortality term (Fig. 6b). The fits are excellent (adjusted R2 = 0.9994, F-test P < 10−16, see Fig. 6b).
We find that the main driver for rectangularization of the survival curve in human data is the decline in extrinsic morality. Similar results are found when fitting human hazard to the Gamma–Gompertz–Makeham equation67,68—the age-independent extrinsic mortality (additive Makeham term) drops with cohort birth year (Fig. 6c), whereas the Gompertz slope and intercept remain relatively unchanged (Fig. 6d, e). The dominance of the drop in extrinsic mortality in human cohorts is consistent with previous studies7,9. This contrasts with model organism data analyzed above in Fig. 3. These animal cohorts were studied in controlled environments and extrinsic mortality is not the main determinant of their survival curve steepness.
In addition to changes in extrinsic mortality, there have been age-specific improvements in mortality rates. Until recent decades, this was primarily a reduction in young deaths (younger than median lifespan), and in the past few decades this shifted to a reduction in old deaths (older than median lifespan)69. These changes are likely to be due to public health and medical interventions, as well as changes in education, socioeconomic status and other factors70. Such age-specific changes confound an attempt to fit changes in SR model parameters to this human data. Thus, why some countries show a reduction in relative sickspan whereas others show an increase65 may not be directly linked to changes in SR model parameters.
Discussion
We present the hypothesis that longevity interventions that steepen survival curves compress relative sickspan. In contrast, interventions that scale the survival curve extend healthspan and sickspan proportionally as they extend lifespan, and thus do not compress relative sickspan. These effects hold in the saturating-removal mathematical model of aging, where interventions that affect damage production rate cause approximate scaling and mild extension of sickspan, whereas interventions that increase damage removal rate or thresholds cause steepening and compress sickspan. The hypothesis is validated in data from invertebrates and mice. We discuss interventions in mice which steepen the survival curve as candidates to compress relative sickspan. The theory also applies to combinations of steepening and scaling interventions that show additive effects.
One can intuitively argue for this hypothesis without need for a mathematical model. Many of the longevity interventions that scale the survival curve seem to generally slow the tempo of aging processes (e.g., temperature in invertebrates, dietary restriction). If one assumes that age-related morbidity originates from the same factors that drive aging and mortality, it makes sense that healthspan and sickspan should also scale by the same proportions as lifespan.
In contrast, longevity interventions that steepen the survival curve may be argued to affect processes of aging-related decline beyond its overall tempo. They make the mortality curve more rectangular and thus the time of death less variable between individuals. This can be considered to reduce the proportion of frail individuals that normally die at ages younger than the median lifespan. Steepening interventions seem to make the whole population more robust (longer lived) and at the same time more homogenous in terms of frailty. An extreme steepening means that almost all individuals reach the maximal lifespan. In humans, individuals close to the maximal lifespan often have a relatively short sickspan71,72. Thus, it is plausible that relative sickspan is shortened by steepening interventions.
To obtain a quantitative account of how survival curve steepness may result in compressed sickspan we used the saturating-removal (SR) model. This model was developed and calibrated based on data in mice and adjusted to human timescales32. The SR model assumes a form of damage X that drives morbidity and mortality, which rises with age in a fluctuating way. The model is agnostic to the nature of this damage, which could be different in different species. The model includes a production of driving damage X at a rate that rises linearly with age—corresponding to accumulation of damage-producing units that are not removed. It also assumes that removal of the driving damage X occurs by mechanisms that saturate at high damage.
The SR model was previously validated against patterns of aging from diverse studies. The model displays the Gompertz law of mortality in which hazard rises exponentially with age, as well as the late age slowdown of hazard, and explains the Weibull-like shape of mice survival curves32. The model quantitatively predicts the effect of mice parabiosis on senescent cell parameters33 in agreement with data. Parabiosis in the model is explained by the young mouse sharing removal capacity with the old mouse (e.g., immune cells). The SR model predicts the slowdown in senescent cell removal rate with age in agreement with mice experiments32. It also explains the rapid shifts between survival curves upon dietary midlife interventions in flies, and the change in hazard slope upon temperature changes32. The SR model was extended by Katzir et al. to explain in quantitative detail the exponential rise of human age-related disease incidence, as well as the incidence decline at very old ages. The extended model assumed two parameters for each disease—a disease threshold and a fraction of susceptible individuals—and provides excellent fits to the incidence curve of hundreds of age-related diseases from large medical record datasets34.
Here, we show that the SR model predicts that perturbations that increase the steepness of survival curves also compresses the sickspan, whereas any perturbation that scales the survival curve also approximately scales the sickspan (extending relative sickspan mildly). More specifically, changing the rate of production of the damage that drives aging leads to approximate scaling of mortality and morbidity. Changing other parameters, such as raising the specific removal rate of the driving damage, extends lifespan with survival curve steepening and compresses morbidity.
One exception is raising the death threshold without correspondingly raising the disease threshold. This steepens the survival curve, but increases relative sickspan, since individuals spend more time between the disease and death thresholds. As a thought experiment, consider artificial life extension by intensive care units—which can increase sickspan by delaying death. A steep survival curve in these situations can result by artificially keeping individuals alive to the same age. We assume that the longevity interventions in the controlled experiments in model organisms that we analyzed here do not cause such uncoordinated changes in death and disease thresholds. In humans, sex differences in the death and morbidity thresholds between females and males could explain the “health survival paradox”—that females have longer lifespans but expanded morbidity. This would occur if death threshold Xc is higher in females (and disease threshold Xd is either the same or lower in females).
Note that we consider survival curve steepness rather than the more commonly studied hazard (Gompertz) slope—the latter is not directly predictive of morbidity compression in our model. Hazard curves are the logarithmic derivative of the survival curves. For example, changes in damage production rate affect hazard slope but not survival steepness, and conversely changes in removal rate or extrinsic mortality do not affect hazard slope but do affect survival steepness. Changes in thresholds and noise affect both. Historically, hazard slope has not changed much in humans, whereas survival curves have steepened. Survival curves are also more robustly measured in experiments than hazard curves.
The SR model makes a major simplifying assumption—that a single damage variable X determines both morbidity and mortality. This provides quantitative predictions that can be tested against data, as in Figs. 3 and 6. Future work can explore more complex situations—for example that damage in each organ affects health differently from lifespan. In such a case there might be multiple qualitatively distinct damage variables rather than a single X. There is evidence that health and lifespan may have overlapping but distinct determinants, and that cognitive functions may have somewhat different aging patterns than other physiological functions34,41,73,74,75. Furthermore, on the population level, genetic and environmental heterogeneity can affect the onset of morbidity and complicate interpretation of the model. Extensions of the SR models can in principle address this complexity34.
Aging research has made progress in understanding molecular and cellular processes that contribute to aging. There is a need for theoretical frameworks to integrate these empirical findings76. The present framework offers a tool to interpret longevity interventions using the shape of the survival curve: Scaling points to effects on the production rate of the driving damage, whereas steepening or shallowing points to effects on the removal rate of the driving damage or its death threshold (not all damage removing mechanisms, but only those specific to the driving damage X). We next discuss how this approach points to specific factors as candidates for the driving damage.
Senolytics extend lifespan and steepen the survival curve, as noted by Kowald and Kirkwood58 who analyzed data from two types of senolytic drugs and from genetic ablation of p16-positive cells. In our analysis, the effect of senolytics resembles increasing removal rate β in the SR model. Thus, in mice, senescent cells (and more generally pro-inflammatory damaged cells) may play the role of the driving damage X in the SR model, as suggested by Karin et al.32.
An intriguing class of steepening interventions includes cyclic ketogenic diet60,61, the ketogenic agent 1,3-butanediol (BD) and the diabetes drugs acarbose54 and canagliflozin55. These interventions share a common mechanism: they all lower glucose spikes, the fraction of time where glucose is at high levels. The drug acarbose inhibits an enzyme that releases glucose from complex carbohydrates in the gut, and canagliflozin is an SGLT2 inhibitor that inhibits kidney glucose reabsorption. These interventions extend median lifespan in male but not female mice.
Glucose spikes are thought to primarily damage the vasculature. Damage to blood vessels is a major pathology in diabetes, causing cardiovascular and renal disease. Endothelial cells are damaged by high glucose in several ways including reactive oxygen species, glycation of proteins and activation of signaling pathways77. Intermittent high glucose causes senescence in endothelial cells78.
The vasculature-protecting mechanisms appear in our analysis to increase damage removal rate β. One interpretation is that damaged microvasculature reduces access of immune cells to the senescent and damaged cells in tissues. Interventions that protect microvasculature may thus enhance the ‘roads’ for immune clearance, and hence increase the removal rate β. This can contribute to their steepening effect on the survival curves.
The notion of vascular protection as a mechanism for the steepening interventions is consistent with a VEGF longevity intervention which increased mouse lifespan by 40% and, in females, steepens the survival curve59. VEGF promotes vascular repair and slows the age-related loss of microvasculature. Vasculature protection may also be relevant for captopril, a hypertension drug which increases steepness with a mild longevity gain in mice.
Non-feminizing estradiol, 17‐α‐estradiol, steepens survival curves and extends lifespan even when administered late in life in male mice79; it has no longevity effect in females. The longevity effects of this estradiol are reported to depend on testicular hormones. It is not clear how this estradiol ties into the mechanism of the other steepening interventions, although it is plausible that it has protective roles on tissues80,81.
Rapamycin treatment also extends mouse lifespan, even when started at middle age53,82,83,84,85, but does not generally steepen the survival curve except at the old-age tail of the survival curve (Supplementary Fig. 8). It may thus have a primary effect that scales survival, such as mTOR inhibition. Notably, one experiment with rapamycin at high dose shows a steepening effect in females, particularly on the part of the survival curve that corresponds to very old ages. It may thus have a secondary effect at high doses on older individuals.
Additional interventions that cause steepening but with milder longevity effects include antioxidants and anti-inflammatory agents (NDGA57, green tea extract56) (Supplementary Fig. 7). In the SR model, strong steepening with mild lifespan extension characterizes coordinated increases in the mortality and morbidity threshold Xc and Xd. One may hypothesize that these thresholds are affected by tolerance to inflammatory damage which is a major causal factor in aging86,87. Indeed, a major deleterious effect of senescent and damaged cells is secretion of inflammatory factors88.
Interventions that scale the survival curve are predicted not to compress sickspan—instead they are suggested to extend sickspan by the same proportion that they extend lifespan (or even to expand relative morbidity). These interventions include caloric restriction. Caloric restriction has pleiotropic effects beyond its effects on longevity such as reducing body weight, reducing fertility and enhancing frailty89.
It would be interesting to see whether emerging interventions such as in vivo partial epigenetic reprogramming scale or not. Data from preliminary studies does not show significant steepening23,24 (Supplementary Fig. 12), although further research is warranted.
Future work can further explore how the SR model relates to human mortality and sickspan. Rectangularization of the human survival curve over the past century is primarily due to reduction in extrinsic mortality rather than changes in intrinsic parameters. Old-age survival and morbidity in humans is impacted by heterogeneity of socioeconomic status90,91,92, lifestyle, genetics72, medical care and public health92. An important factor is emotional health—older cohorts appear to have high average well-being93, whereas social isolation in the old has major negative effects94. Such factors can complicate a direct comparison to the SR model.
We present a theory and evidence that longevity interventions that steepen the survival curve compress morbidity. Conversely, interventions that do not change the shape of the survival curve, namely interventions that show scaling, extend lifespan but do not compress morbidity. The theory is supported by data from model organisms and by mathematical modeling using the saturating-removal (SR) model of aging. The theory helps to interpret intervention mechanisms of action by means of survival curve shape—we discuss various interventions in mice that steepen survival curves, such as senolytics, ketogenic diet, acarbose and canagliflozin, and suggest their potential mechanisms of action. We apply this to combinations of interventions where steepening and scaling interventions have additive effects. This study provides insights into the relationship between survival curves, longevity interventions, and relative sickspan, contributing to our understanding of strategies to improve health in aging individuals.
Methods
Ethical regulations
This study involves neither new animal experiments nor human studies. It complies with all relevant ethical regulations.
Saturating-removal (SR) model simulations
We simulated the SR model using parameters reported in Karin et al.32. For mice, η = 2.3 × 10−4/day2, β = 0.15 /day, κ = 0.5, ε = 0.16 /day, Xc = 17. For humans, baseline parameters are η = 1.4 × 10−3/(day*year), β = 0.15 /day, κ = 0.5, ε = 0.16/day, Xc = 17. The sickspan threshold Xd was set to 12, which is at the lower end of the estimated thresholds for age-related diseases34. This results in a mean sickspan of 12.3 y, consistent with reported age achieved without major chronic diseases in the United States95. We simulated interventions by varying an individual parameter η, β, ε, or Xc, or by simultaneously changing Xc and Xd by the same factor. Simulation used Mathematica 14.0.
Survival and healthspan data
Individual-based longitudinal survival and health data are collected from refs. 40,41,42. The authors of ref. 40 provided the raw data (individual lifespans and healthspans of flies). Data from ref. 41 (individual lifespans and healthspans of worms measured by movement) and ref. 42 (longitudinal mice frailty index) was downloaded from Github https://github.com/nstroustrup/2022_hierarchical_process_model and figshare (https://doi.org/10.6084/m9.figshare.25125587) respectively. Survival and healthspan distributions from ref. 26 (worm cohort lifespan and healhspan measured by strength) were obtained by digitizing relevant figures using WebPlotDigitizer (https://apps.automeris.io/wpd/). In Fig. 3d one outlier datapoint was not shown: glp-1 in Oswal et al.41 (relative steepness 1.08 ± 0.11, relative sickspan 0.48 ± 0.05, Supplementary Table 4). This mutant was also tested in Statzer et al.26 and included in Fig. 3c, where a different sterile strain was used as control.
For experiments conducted by the ITP, we downloaded lifespans of individual mice from experimental and control cohorts (C2004–C2017) directly from the Mouse Phenome Database (https://phenome.jax.org/projects/ITP1, June 2023). Experiments with different drug concentrations and different initiation age and regimes of exposure are analyzed and reported separately as different interventions. ITP used UM-HET3 mice, a heterogenous stock produced by a four-way cross.
For mice experiments outside of ITP, we downloaded the PDFs of the relevant publications and used WebPlotDigitizer to digitize the survival curves. We also recorded the genetic background and the sample sizes of control and treated cohorts. From these survival curves, we inferred the times of death of individual mice constituting the data. We excluded publications using mice strains considered to be disease models that have specific deleterious genes. All but one study used inbred strains or hybrids involving two-way or three-way crosses among inbred strains.
Human hazard curves are downloaded from the Human Mortality Database66. Relevant health expectancy surveys are described in refs. 8,65 and digitized from refs. 96,97.
Steepness of survival curves
We define steepness as the mean divided by the standard deviation of lifespan. For empirical survival curves throughout the present study, we calculated steepness from the right-censored survival time data as follows: we removed the 10% shortest event times (censored or deaths) and then computed the ratio of the mean and standard deviation of event times, i.e., inverse trimmed coefficient of variation (iTCV). This definition of steepness is less sensitive to sampling errors than the inverse of relative IQR studied by Carnes et al.29 and provides similar results to inverse CV after trimming both the top 10% and bottom 10% of event times (Supplementary Information S4, Supplementary Fig. 3).
C. elegans data presents significant batch effects which can confound steepness estimates. We addressed this (Supplementary Fig. 4) by temporarily rescaling the death times of each batch before pooling the batches and calculating steepness, using the accelerated failure time (AFT) approach30 in the section below.
Statistical analysis of mice survival curves
To ascertain whether an intervention changes the shape of the survival curve, we follow Stroustrup et al.30 and use an accelerated failure time (AFT) approach with a Kolgomorov-Smirnov (KS) test modified to accommodate right-censored data98. The rescaling is based on the accelerated failure time model implemented using Python package lifelines (version 0.27.7). We use this test to classify treatments into scaling and non-scaling categories, by applying a threshold on the KS p value of 0.1 (Supplementary Fig. 6).
For Fig. 4a, b, we sought to identify interventions with a significant effect in terms of mean lifespan and steepness. For this purpose, we bootstrapped the death times with returns. For every mouse cohort (control and interventions per ITP site and sex), we resampled with returns the recorded death times and censorship status. We repeated this 200 times. Based on these bootstrapped samples, we estimated the joint distributions of median lifespan and steepness for both control μc = (ln(Lc), ln(Sc)) and intervention cohorts μi = (ln(Li), ln(Si)) by 2D normal distributions Nc(μc, σc) and Ni(μi, σi). We then tested the null hypothesis that the control and intervention groups have the same longevity and steepness (H0: Li/Lc = 1 and Si/Sc = 1). Because μi − μc ~ Ni(μi-μc, σi + σc), H0 is equivalent to a Mahalanobis distance between control group (ln(Lc), ln(Sc)) and intervention group (ln(Li), ln(Si)) of 0. Thus, for every intervention and its control, we calculated the p value that μi − μc = 0 using Hostelling’s t-squared statistic and Hotelling’s T-squared distribution with 2 dimensions and 198 degrees of freedom.
For intervention experiments conducted by ITP, we apply a p-value threshold adjusted for multiple comparisons using the Benjamini–Hochberg method. For an α level of 0.05, the adjusted p-value threshold is 0.0113. For intervention experiments conducted outside of ITP, due to the varying data quality and statistical power, we conducted Benjamini–Hochberg adjustment separately from those in ITP, resulting in an adjusted P-value threshold of 0.0214 (α = 0.05).
Statistical analysis of human mortality data
We downloaded human cohort mortality data from the Human Mortality Database66. We used the cohort death rate and exposure-to-risk data with 1 × 5 (age × year) intervals to estimate model parameters.
We estimated the extrinsic (Makeham) and age-related (Gamma–Gompertz) components of mortality for each cohort using the Gamma–Gompertz-Makeham model h(t) = m + a ec+bt/(ec-1 + ebt). We fitted the log-transformed age-specific death rates using NonlinearModelFit of Mathematica 14.0. We used the square root of death numbers as weights for each age group, to balance the strengths of evidence with residue minimization in the log hazard space. The goodness-of-fit is excellent for all countries and cohorts in Fig. 6c–e, with adjusted R2 > 0.995.
We identified SR model parameters that correspond to a given cohort by minimizing the residues in log hazard space, between Gamma–Gompertz hazards h(t) = a ec+bt/(ec-1 + ebt) of a given cohort, and hazards of simulated SR models. Like the fitting metric above, the residues were weighted according to the square root of death numbers. The simulation was done in Mathematica 14.0, implementing the Euler–Maruyama method with N = 5 104 simulated individuals.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
This study does not generate original primary data. All data supporting the findings described in this manuscript are available in the article and in the Supplementary Information and from the corresponding author upon request. The raw (individual-level longitudinal health) data for mice, flies and worms needed to reproduce both Fig. 3 and Supplementary Figs. 2–4 can be assessed at https://github.com/y1fanyang/compressMorbidity. The primary data from ref. 41 (worms movement) and ref. 42 (mice frailty index) can be downloaded from GitHub https://github.com/nstroustrup/2022_hierarchical_process_model and figshare (https://doi.org/10.6084/m9.figshare.25125587), respectively. The processed cohort-level intervention data behind Fig. 3 can be found as Supplementary Tables 1–4 and in the source data file. The primary NIA ITP survival times data needed to reproduce Figs. 4a, 5, and Supplementary Figs. 5–7, 9 and 10 can be downloaded from the Mouse Phenome Database https://phenome.jax.org/projects/ITP1. The processed intervention data for mice (Figs. 4 and 5 and Supplementary Figs. 5–8) analyzed with and without NIA ITP can be found as Supplementary Dataset 1 and 2, respectively. The human mortality data used in this study in Fig. 6, such as Exposure-to-risk and Death rates, are available Human Mortality Database https://www.mortality.org/, under pages for cohort data from individual countries. Source data are provided with this paper.
Code availability
The code needed to reproduce this study is available at https://github.com/y1fanyang/compressMorbidity99.
References
Olshansky, S. J., Rudberg, M. A., Carnes, B. A., Cassel, C. K. & Brody, J. A. Trading off longer life for worsening health: the expansion of morbidity hypothesis. J. Aging Health 3, 194–216 (1991).
Kirkland, J. L. & Peterson, C. Healthspan, translation, and new outcomes for animal studies of aging. J. Gerontol. A. Biol. Sci. Med. Sci. 64, 209–212 (2009).
Seals, D. R., Justice, J. N. & LaRocca, T. J. Physiological geroscience: targeting function to increase healthspan and achieve optimal longevity. J. Physiol. 594, 2001–2024 (2016).
Blagosklonny, M. V. How to save medicare: the anti-aging remedy. Aging 4, 547–552 (2012).
Goldman, D. P. et al. Substantial health and economic returns from delayed aging may warrant a new focus for medical research. Health Aff. 32, 1698–1705 (2013).
Harper, S. Economic and social implications of aging societies. Science 346, 587–591 (2014).
Fries, J. F. Aging, natural death, and the compression of morbidity. New Engl. J. Med. 303, 130–135 (1980).
Jagger, C. & Robine, J.-M. Healthy life expectancy. In International Handbook of Adult Mortality (eds Rogers, R. G. & Crimmins, E. M.) 551–568 (Springer Netherlands, 2011).
Manton, K. G. Changing concepts of morbidity and mortality in the elderly population. Milbank Mem. Fund. Q. Health Soc. 60, 183–244 (1982).
Longo, V. D. & Anderson, R. M. Nutrition, longevity and disease: from molecular mechanisms to interventions. Cell 185, 1455–1470 (2022).
Gonzalez-Freire, M. et al. The road ahead for health and lifespan interventions. Ageing Res. Rev. 59, 101037 (2020).
Wasko, B. M. & Kaeberlein, M. Yeast replicative aging: a paradigm for defining conserved longevity interventions. FEMS Yeast Res. 14, 148–159 (2014).
Maglioni, S., Arsalan, N. & Ventura, N. C. elegans screening strategies to identify pro-longevity interventions. Mech. Ageing Dev. 157, 60–69 (2016).
Tatar, M., Post, S. & Yu, K. Nutrient control of Drosophila longevity. Trends Endocrinol. Metab. 25, 509–517 (2014).
Weindruch, R., Walford, R. L., Fligiel, S. & Guthrie, D. The retardation of aging in mice by dietary restriction: longevity, cancer, immunity and lifetime energy intake. J. Nutr. 116, 641–654 (1986).
Fontana, L., Partridge, L. & Longo, V. D. Extending healthy life span—from yeast to humans. Science 328, 321–326 (2010).
Murphy, C. T. & Hu, P. J. in WormBook: The Online Review of C. elegans Biology (ed. The C. elegans Research Community) Ch. 177 (WormBook, 2018).
Lamming, D. W., Ye, L., Sabatini, D. M. & Baur, J. A. Rapalogs and mTOR inhibitors as anti-aging therapeutics. J. Clin. Investig. 123, 980–989 (2013).
Mannick, J. B. & Lamming, D. W. Targeting the biology of aging with mTOR inhibitors. Nat. Aging 3, 642–660 (2023).
Yousefzadeh, M. J. et al. Fisetin is a senotherapeutic that extends health and lifespan. EBioMedicine 36, 18–28 (2018).
Xu, M. et al. Senolytics improve physical function and increase lifespan in old age. Nat. Med. 24, 1246–1256 (2018).
Baker, D. J. et al. Naturally occurring p16Ink4a-positive cells shorten healthy lifespan. Nature 530, 184–189 (2016).
Ocampo, A. et al. In vivo amelioration of age-associated hallmarks by partial reprogramming. Cell 167, 1719–1733.e12 (2016).
Macip, C. C. et al. Gene therapy mediated partial reprogramming extends lifespan and reverses age-related changes in aged mice. Cell. Reprogram. 26, 24–32 (2024).
Macchiarini, F., Miller, R. A., Strong, R., Rosenthal, N. & Harrison, D. E. Chapter 10—NIA interventions testing program: a collaborative approach for investigating interventions to promote healthy aging. In Handbook of the Biology of Aging, Ninth Edition (eds Musi, N. & Hornsby, P. J.) 219–235 (Academic Press, 2021).
Statzer, C., Reichert, P., Dual, J. & Ewald, C. Y. Longevity interventions temporally scale healthspan in Caenorhabditis elegans. iScience 25, 103983 (2022).
Hahm, J.-H. et al. C. elegans maximum velocity correlates with healthspan and is maintained in worms with an insulin receptor mutation. Nat. Commun. 6, 8919 (2015).
Papadopoulos, N. T. et al. Dietary effects on sex-specific health dynamics of medfly: support for the dynamic equilibrium model of aging. Exp. Gerontol. 46, 1026–1030 (2011).
Carnes, B. A., Holden, L. R., Olshansky, S. J., Witten, M. T. & Siegel, J. S. Mortality partitions and their relevance to research on senescence. Biogerontology 7, 183–198 (2006).
Stroustrup, N. et al. The temporal scaling of Caenorhabditis elegans ageing. Nature 530, 103–107 (2016).
Liu, P. & Acar, M. The generational scalability of single-cell replicative aging. Sci. Adv. 4, eaao4666 (2018).
Karin, O., Agrawal, A., Porat, Z., Krizhanovsky, V. & Alon, U. Senescent cell turnover slows with age providing an explanation for the Gompertz law. Nat. Commun. 10, 5495 (2019).
Karin, O. & Alon, U. Senescent cell accumulation mechanisms inferred from parabiosis. GeroScience 43, 329–341 (2021).
Katzir, I. et al. Senescent cells and the incidence of age-related diseases. Aging Cell 20, e13314 (2021).
Yang, Y. et al. Damage dynamics and the role of chance in the timing of E. coli cell death. Nat. Commun. 14, 2209 (2023).
Swindell, W. R. Accelerated failure time models provide a useful statistical framework for aging research. Exp. Gerontol. 44, 190–200 (2009).
Liang, Y. et al. Calorie restriction is the most reasonable anti-ageing intervention: a meta-analysis of survival curves. Sci. Rep. 8, 5779 (2018).
Hughes, B. G. & Hekimi, S. Different mechanisms of longevity in long-lived mouse and Caenorhabditis elegans mutants revealed by statistical analysis of mortality rates. Genetics 204, 905–920 (2016).
Yashin, A. I., Iachine, I. A. & Begun, A. S. Mortality modeling: a review. Math. Popul. Stud. 8, 305–332 (2000).
Gaitanidis, A. et al. Longitudinal assessment of health-span and pre-death morbidity in wild type Drosophila. Aging 11, 1850–1873 (2019).
Oswal, N., Martin, O. M. F., Stroustrup, S., Bruckner, M. A. M. & Stroustrup, N. A hierarchical process model links behavioral aging and lifespan in C. elegans. PLoS Comput. Biol. 18, e1010415 (2022).
Luciano, A. et al. Longitudinal fragility phenotyping contributes to the prediction of lifespan and age-associated morbidity in C57BL/6 and diversity outbred mice. GeroScience 46, 4937–4954 (2024).
Kane, A. E. et al. Impact of longevity interventions on a validated mouse clinical frailty index. J. Gerontol. A. Biol. Sci. Med. Sci. 71, 333–339 (2016).
Xie, K. et al. Deep phenotyping and lifetime trajectories reveal limited effects of longevity regulators on the aging process in C57BL/6J mice. Nat. Commun. 13, 6830 (2022).
Ruby, J. G. et al. An automated, home-cage, video monitoring-based mouse frailty index detects age-associated morbidity in C57BL/6 and diversity outbred mice. J. Gerontol. A. Biol. Sci. Med. Sci. 78, 762–770 (2023).
Carey, J. R., Liedo, P., MÜller, H.-G., Wang, J.-L. & Vaupel, J. W. A simple graphical technique for displaying individual fertility data and cohort survival: case study of 1000 Mediterranean Fruit Fly females. Funct. Ecol. 12, 359–363 (1998).
Carey, J. R. et al. Life history response of Mediterranean fruit flies to dietary restriction. Aging Cell 1, 140–148 (2002).
Carey, J. R. et al. Stochastic dietary restriction using a Markov-chain feeding protocol elicits complex, life history response in medflies. Aging Cell 4, 31–39 (2005).
Spiridonova, O., Kriukov, D., Nemirovich-Danchenko, N. & Peshkin, L. On standardization of controls in lifespan studies. Aging 16, 3047–3055 (2024).
Nadon, N. L., Strong, R., Miller, R. A. & Harrison, D. E. NIA interventions testing program: investigating putative aging intervention agents in a genetically heterogeneous mouse model. eBioMedicine 21, 3–4 (2017).
Harrison, D. E. et al. 17-a-estradiol late in life extends lifespan in aging UM-HET3 male mice; nicotinamide riboside and three other drugs do not affect lifespan in either sex. Aging Cell 20, e13328 (2021).
Harrison, D. E. et al. Acarbose, 17-α-estradiol, and nordihydroguaiaretic acid extend mouse lifespan preferentially in males. Aging Cell 13, 273–282 (2014).
Strong, R. et al. Longer lifespan in male mice treated with a weakly estrogenic agonist, an antioxidant, an α-glucosidase inhibitor or a Nrf2-inducer. Aging Cell 15, 872–884 (2016).
Harrison, D. E. et al. Acarbose improves health and lifespan in aging HET3 mice. Aging Cell 18, e12898 (2019).
Miller, R. A. et al. Canagliflozin extends life span in genetically heterogeneous male but not female mice. JCI Insight 5, e140019 (2020).
Strong, R. et al. Evaluation of resveratrol, green tea extract, curcumin, oxaloacetic acid, and medium-chain triglyceride oil on life span of genetically heterogeneous mice. J. Gerontol. A. Biol. Sci. Med. Sci. 68, 6–16 (2013).
Strong, R. et al. Nordihydroguaiaretic acid and aspirin increase lifespan of genetically heterogeneous male mice. Aging Cell 7, 641–650 (2008).
Kowald, A. & Kirkwood, T. B. L. Senolytics and the compression of late-life mortality. Exp. Gerontol. 155, 111588 (2021).
Grunewald, M. et al. Counteracting age-related VEGF signaling insufficiency promotes healthy aging and extends life span. Science 373, eabc8479 (2021).
Roberts, M. N. et al. A ketogenic diet extends longevity and healthspan in adult mice. Cell Metab. 26, 539–546.e5 (2017).
Newman, J. C. et al. Ketogenic diet reduces midlife mortality and improves memory in aging mice. Cell Metab. 26, 547–557.e8 (2017).
Strong, R. et al. Lifespan benefits for the combination of rapamycin plus acarbose and for captopril in genetically heterogeneous mice. Aging Cell 21, e13724 (2022).
Wilmoth, J. R. & Horiuchi, S. Rectangularization revisited: variability of age at death within human populations. Demography 36, 475–495 (1999).
Aburto, J. M., Villavicencio, F., Basellini, U., Kjærgaard, S. & Vaupel, J. W. Dynamics of life expectancy and life span equality. Proc. Natl. Acad. Sci. USA 117, 5250–5259 (2020).
Robine, J.-M., Jagger, C., Crimmins, E. M., Saito, Y. & Van Oyen, H. Trends in Health Expectancies. In International Handbook of Health Expectancies (eds Jagger, C. et al.) 19–34 (Springer International Publishing, Cham, 2020).
HMD. Human Mortality Database. Max Planck Institute for Demographic Research (Germany), University of California, Berkeley (USA), and French Institute for Demographic Studies (France). www.mortality.org (2024).
Makeham, W. M. On the law of mortality and the construction of annuity tables. Assur. Mag. J. Inst. Actuar. 8, 301–310 (1860).
Yang, Y. et al. Temporal scaling of aging as an adaptive strategy of Escherichia coli. Sci. Adv. 5, eaaw2069 (2019).
Vaupel, J. W. Biodemography of human ageing. Nature 464, 536–542 (2010).
Zhang, Y.-B. et al. Associations of healthy lifestyle and socioeconomic status with mortality and incident cardiovascular disease: two prospective cohort studies. BMJ 373, n604 (2021).
Andersen, S. L., Sebastiani, P., Dworkis, D. A., Feldman, L. & Perls, T. T. Health span approximates life span among many supercentenarians: compression of morbidity at the approximate limit of life span. J. Gerontol. Ser. A 67A, 395–405 (2012).
Ismail, K. et al. Compression of morbidity is observed across cohorts with exceptional longevity. J. Am. Geriatr. Soc. 64, 1583–1591 (2016).
Tang, B. et al. Longitudinal associations between use of antihypertensive, antidiabetic, and lipid-lowering medications and biological aging. GeroScience 45, 2065–2078 (2023).
Prattichizzo, F. et al. Organ-specific biological clocks: ageotyping for personalized anti-aging medicine. Ageing Res. Rev. 96, 102253 (2024).
Goeminne, L. J. E. et al. Plasma-based organ-specific aging and mortality models unveil diseases as accelerated aging of organismal systems. Cell Metab. 37, 205–222.e6 (2025).
Cohen, A. A. et al. A complex systems approach to aging biology. Nat. Aging 2, 580–591 (2022).
Campos, C. Chronic hyperglycemia and glucose toxicity: pathology and clinical sequelae. Postgrad. Med. 124, 90–97 (2012).
Maeda, M., Hayashi, T., Mizuno, N., Hattori, Y. & Kuzuya, M. Intermittent high glucose implements stress-induced senescence in human vascular endothelial cells: role of superoxide production by NADPH oxidase. PLoS ONE 10, e0123169 (2015).
Mann, S. N. et al. Health benefits attributed to 17α-estradiol, a lifespan-extending compound, are mediated through estrogen receptor α. eLife 9, e59616 (2020).
Dykens, J. A., Moos, W. H. & Howell, N. Development of 17α-estradiol as a neuroprotective therapeutic agent: rationale and results from a phase I clinical study. Ann. N. Y. Acad. Sci. 1052, 116–135 (2005).
Stout, M. B. et al. 17α-Estradiol alleviates age-related metabolic and inflammatory dysfunction in male mice without inducing feminization. J. Gerontol. Ser. A 72, 3–15 (2017).
Harrison, D. E. et al. Rapamycin fed late in life extends lifespan in genetically heterogeneous mice. Nature 460, 392–395 (2009).
Miller, R. A. et al. Rapamycin, but not resveratrol or simvastatin, extends life span of genetically heterogeneous mice. J. Gerontol. Ser. A 66A, 191–201 (2011).
Wilkinson, J. E. et al. Rapamycin slows aging in mice. Aging Cell 11, 675–682 (2012).
Strong, R. et al. Rapamycin-mediated mouse lifespan extension: late-life dosage regimes with sex-specific effects. Aging Cell 19, e13269 (2020).
Wikby, A. et al. The immune risk phenotype is associated with IL-6 in the terminal decline stage: findings from the Swedish NONA immune longitudinal study of very late life functioning. Mech. Ageing Dev. 127, 695–704 (2006).
Franceschi, C., Garagnani, P., Parini, P., Giuliani, C. & Santoro, A. Inflammaging: a new immune–metabolic viewpoint for age-related diseases. Nat. Rev. Endocrinol. 14, 576–590 (2018).
Coppé, J.-P., Desprez, P.-Y., Krtolica, A. & Campisi, J. The senescence-associated secretory phenotype: the dark side of tumor suppression. Annu. Rev. Pathol. 5, 99–118 (2010).
Westendorp, R. G. & Kirkwood, T. B. Human longevity at the cost of reproductive success. Nature 396, 743–746 (1998).
Marmot, M. G. et al. Health inequalities among British civil servants: the Whitehall II study. Lancet 337, 1387–1393 (1991).
Anderson, R. T., Sorlie, P., Backlund, E., Johnson, N. & Kaplan, G. A. Mortality effects of community socioeconomic status. Epidemiology 8, 42–47 (1997).
Stringhini, S. et al. Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: a multicohort study and meta-analysis of 1·7 million men and women. Lancet 389, 1229–1237 (2017).
Carstensen, L. L. et al. Emotional experience improves with age: evidence based on over 10 years of experience sampling. Psychol. Aging 26, 21–33 (2011).
Tomaka, J., Thompson, S. & Palacios, R. The relation of social isolation, loneliness, and social support to disease outcomes among the elderly. J. Aging Health 18, 359–384 (2006).
Nyberg, S. T. et al. Association of healthy lifestyle with years lived without major chronic diseases. JAMA Intern. Med. 180, 760–768 (2020).
Doblhammer, G. & Kytir, J. Compression or expansion of morbidity? Trends in healthy-life expectancy in the elderly Austrian population between 1978 and 1998. Soc. Sci. Med. 52, 385–391 (2001).
Jagger, C. et al. A comparison of health expectancies over two decades in England: results of the Cognitive Function and Ageing Study I and II. Lancet 387, 779–786 (2016).
Fleming, T. R., O’Fallon, J. R., O’Brien, P. C. & Harrington, D. P. Modified Kolmogorov-Smirnov test procedures with application to arbitrarily right-censored data. Biometrics 36, 607–625 (1980).
Yang, Y. et al. Compression of morbidity by interventions that steepen the survival curve. Github https://doi.org/10.5281/zenodo.14737548 (2025).
Acknowledgements
The authors thank Christos Consoulas, Jeong-Hoon Hahm for sharing original data on Drosophila sickspan and worms’ maximal velocity, respectively, and Nicholas Stroustrup for general discussion and for sharing shortened twilight data in worms. The authors thank Richard Miller for providing feedback and discussions on mice survival curves. The authors also thank Nir Barzilai, Pinchas Cohen, Valery Krizhanovsky, Coleen Murphy, Collin Ewald, Jan Gruber, Sara Hägg and Vadim Gladyshev for general discussion and feedback. The authors also thank Glen Pridham for numerous help on methodology and understanding mice and human frailty; and David S. Glass, Elizabeth Vaisbourd, Alon Bar, and Tomer Milo for editing help. Received funding from European Research Council (ERC) grant agreement No 856487 (UA).
Author information
Authors and Affiliations
Contributions
Conceptualization: Y.Y., D.F.J., and U.A.; methodology: Y.Y., A.M., N.R., and U.A.; data gathering and curation: Y.Y., A.M., and T.L.; computational investigation: Y.Y., A.M., B.S., N.R., and U.A.; statistical analysis: Y.Y., A.M., and T.L.; visualization: Y.Y. and U.A.; writing—original draft: Y.Y. and U.A.; writing—review and editing: Y.Y. and U.A.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Jay Olshansky and the other anonymous reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yang, Y., Mayo, A., Levy, T. et al. Compression of morbidity by interventions that steepen the survival curve. Nat Commun 16, 3340 (2025). https://doi.org/10.1038/s41467-025-57807-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41467-025-57807-5
