
Abstract
High ambient temperatures are associated with reduced sleep duration and quality, but effects on obstructive sleep apnea (OSA) severity are unknown. Here we quantify the effect of 24 h ambient temperature on nightly OSA severity in 116,620 users of a Food and Drug Administration-cleared nearable over 3.5 years. Wellbeing and productivity OSA burden for different levels of global warming were estimated. Globally, higher temperatures (99th vs. 25th; 27.3 vs. 6.4 °C) were associated with a 45% higher probability of having OSA on a given night (mean [95% confidence interval]; 1.45 [1.44, 1.47]). Warming-related increase in OSA prevalence in 2023 was estimated to be associated with a loss of 788,198 (489,226, 1,087,170) healthy life years (in 29 countries), and a workplace productivity loss of 30 (21 to 40) billion United States dollars. Scenarios with projected temperatures ≥1.8 °C above pre-industrial levels would incur a further 1.2 to 3-fold increase in OSA burden by 2100.
Similar content being viewed by others

Introduction
In 2023, mean temperature recordings in the northern hemisphere were the highest on record in over 2000 years1, with temperatures 2.07 °C warmer than the pre-industrial period ( ~ 1850-1900)1. Mean global temperature is projected to increase by 2.1 to 3.4 °C above pre-industrial levels by the end of the century, in the absence of additional reductions in greenhouse gas emissions2. High ambient temperatures have strong, well-established, negative effects on health3,4, including mental health outcomes5,6,7, reduced physical activity8, and ultimately, mortality9,10,11,12,13,14. High ambient temperatures are also associated with considerable reductions in sleep duration and quality15,16,17, including a near doubling of short sleep ( < 6 h) prevalence18. Sleep loss due to global warming in 2023 was recently estimated to incur a loss of 3.9 million years of life because of disability or death18.
Obstructive sleep apnea (OSA) is the most common sleep-related breathing disorder with an estimated global prevalence of nearly 1 billion adults19. OSA severity is typically quantified using the apnea-hypopnea index (AHI), a count of partial (hypopnea) or total (apnea) upper airway collapses per hour of sleep. Untreated OSA is associated with a wide range of adverse health outcomes20, road safety events21, and all-cause mortality20. Increased OSA severity also has a dose-response relationship with the incidence of co-morbid chronic conditions, such as hypertension and type-2 diabetes20. In addition, untreated OSA is associated with large decreases in workplace productivity and absenteeism. This is estimated to cost the Australian economy nearly 4 billion AUD22 and the US economy nearly $87 billion US per year23; while data for other countries is lacking.
Some studies have shown an association between outdoor ambient temperature and OSA severity24,25,26,27. A major limitation is that most prior studies are cross-sectional and use single-night estimates of AHI, therefore neglecting to account for the substantial night-to-night variability in AHI28,29,30. Furthermore, to the best of our knowledge, personal, and social burden of OSA due to increased temperatures, including changes in prevalence, wellbeing burden, and workplace productivity loss have not been quantified to date. Given the potential future impact that global warming is expected to have on OSA prevalence, better estimates of the subsequent burden are needed.
Accordingly, in this global study involving 116,620 users of a validated and Food and Drug Administration (FDA)-cleared nearable OSA monitor, we investigate the dose-response relationship between daily ambient temperature and nightly OSA status, using data from the fifth generation of European Reanalysis (ERA5) dataset31. We demonstrate that high-temperature days (99th percentile; 27.3 °C) increase the probability of OSA by 45% compared to low-temperature days (25th percentile; 6.4 °C). The effect size varies by country and is generally stronger in European countries. The increased prevalence of OSA attributed to global warming in 2023 is associated with a loss of over 780,000 healthy life years and 105 million workplace productivity days across 29 countries, resulting in an estimated economic cost of ~98 billion United States dollars. Projections estimate that a ≥ 1.8 °C increase in global ambient temperature above pre-industrial levels could double the burden, impacts, and costs of OSA by 2100.
Results
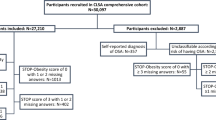
Data for final analysis was acquired from 116,620 regular users of the under-mattress OSA sensor, for a combined total of ~62 million nights. The most common reason for excluding participants (N = 8261, ~6.6%) was a lack of regular use of the device (see flow chart in Supplementary Fig. 1). Users were mainly middle-aged and predominantly male (22.7% female), with a median [IQR] of 509 [246, 787] sleep recordings per user (Table 1). The overall prevalence of moderate-to-severe (AHI ≥ 15 events/h) and severe OSA (AHI ≥ 30 events/h) was 25.4% and 8.9%, respectively. Users were located across most world regions (Fig. 1), including 41 countries with at least 100 users. OSA prevalence was between 15 and 32% depending on the country (Fig. 1), and demographics were consistent across countries (Table S1).

Country by country prevalence of moderate-to-severe obstructive sleep apnea (OSA) (blue) and severe OSA (dark blue) is highlighted in the bar chart. Source data are provided as a Source Data file.
Ambient temperature and OSA prevalence
There was a non-linear dose-response association between 24 h daily average ambient temperatures and the risk of having OSA on the following night (Fig. 2a). Globally, the probability of having OSA was 45% (risk ratio (RR) [95%CI]; 1.45 [1.44, 1.47]) higher during days with high temperatures (99th; 27.3 °C) vs. during days with lower temperatures (25th; 6.4 °C). Similarly, the probability of having severe OSA was 49% (1.49 [1.46, 1.52] higher in high vs. low temperature days. The probability of nightly OSA was higher at T99 in countries with lower gross domestic product (GDP) per capita (Fig. 2b). Out of the 41 studied countries, we found a significant association between ambient temperature and increased probability of nightly OSA in 29 countries (Fig. 2d). The effect size at T99 varied by country (Fig. 2c) and was generally stronger in European countries, with up to ~2.0 -fold increase in the probability of nightly OSA. Similar results were observed for the probability of nightly severe OSA (Table S1). The number of users was generally lower in countries where we did not find a significant association between temperature and OSA prevalence (Table S1). The association between ambient temperature and the probability of nightly OSA was stronger in males, users with higher body mass index (BMI), and among participants with usual sleep duration longer than 6 h (Supplementary Figs. 2 and 4). Age did not have a strong effect on the association between temperature and nightly OSA (Supplementary Figs. 2 and 3). Heterogeneity in country demographics (see Table S1), including mean age (p-value = 0.17), mean BMI (p-value = 0.57), and sex proportion (p-value = 0.68) was not associated with a differential effect in the association between ambient temperature and the probability of nightly OSA. The exposure-response curve between ambient temperature and the probability of nightly OSA remained largely similar in the sensitivity analyses, when minimum or maximum 24 h temperature were used as exposure variables (Supplementary Fig. 4). The exposure-response curve between ambient temperature and the probability of nightly OSA also remained similar when adjusting for particulate matter with aerodynamic diameter <10 µm (Supplementary Fig. 5), previously shown to be associated with increased OSA severity in some studies26. The association between temperature and nightly OSA was also not modified by air pollution levels (Supplementary Fig. 5). A total of 9.4% of nightly sleep recordings did not have an AHI measurement, as the AHI cannot be calculated for nights with a sleep duration of less than 5 h. There was a bias towards a lower effect size in the association between temperature and nightly OSA for participants with a higher amount of missing AHI data (see Supplementary Fig. 6). Given the association between high temperature and short sleep duration16,18, this may suggest that our estimates are conservative.

a Exposure-response curves between temperature and the risk ratio (RR) for nightly OSA (solid green) or nightly severe OSA (dashed purple). Shaded area represents 95%CI. Distribution of temperature (histogram) and temperature at the 99th percentile (T99; dashed black line) are also highlighted. b Subgroup analyses including the mean RR (and 95%CI) for nightly OSA at T99 based on the country of residence’s gross domestic product (GDP) per capita (tertiles – N, tertile 1 :40152; tertile 2: 37722; tertile3: 38468). c RR for nightly OSA at T99 by geographical ___location. d Country by country analysis with mean RR (and 95%CI) for nightly OSA at 99th vs. 25th percentile of temperature (brown indicates p-values < 0.05 and purple p-values > 0.05). Exact N and RR (95%CI) for each country is available in Table S1. Source data are provided as a Source Data file.
Wellbeing burden of warming-related increase in OSA prevalence
We use disability adjusted life years (DALYs), a standardized measure employed by the Global Burden of Disease (GBD)32 studies that captures the combined impact of illness, injury, and premature mortality, to quantify the wellbeing and societal burden due to increased prevalence of OSA from high temperatures. DALYs combines time lost due to premature death (years of life lost; YLL) and time lived with less than-optimal health (years lived with disability; YLD). The increased prevalence of OSA due to global warming was associated with a strong societal impact. For example, in the UK (London; Fig. 3a), we observed a ~ 0.7 °C temperature increase from 2000 to 2023, which corresponded with an additional ~150 million person-days with OSA in 2023 compared to 2000. The increase in OSA prevalence due to global warming was associated with a loss of 59,365 DALYs (uncertainty range: 36,975 to 81,755), including 58,341 YLDs (36,463 to 80,2189), and 1024 YLLs (512 to 1,536); 92% higher than in 2000 (Table S2). In the 29 countries where we found an association between OSA prevalence and ambient temperature (involving 1.02 billion people), temperature-related increase in OSA prevalence was associated with a loss of 788,198 (489,226 to 1,087,170) DALYs in 2023, including 27,180 (13,590 to 40,770) years of life lost. The economic cost of this wellbeing impact in 2023 was estimated to be ~68 billion USD (Table S2) in the 29 studied countries. These estimates were ~2-fold higher than in 2000.

Wellbeing burden of warming-related increase in moderate-to-severe OSA prevalence is exemplified for the UK (a–c and d) and globally (e–g). a Historical and projected temperatures for different climate scenarios from the Intergovernmental Panel on Climate Change (IPCC) were used to (b) derive the number of additional person-days with OSA due to temperature increases, which were subsequently used to calculate (c) years lived with disability (YLD) and (d) years of life lost (YLL). Baseline temperatures were based on the historical 1950-1990 data. The wellbeing and economic impact of the estimated temperature-related increase in OSA by 2100 for different climate scenarios from the IPCC were calculated for (e) YLL, (f) YLD, and (g) wellbeing economic cost, expressed as rate per 100,000 persons per year. The white line-marker represents current rates (as of 2023) of YLL, YLD, and economic cost. Shaded area in the YLD graph represents the yearly wellbeing burden associated with OSA based on Australian estimates22. USD US dollars, SSP Shared Socioeconomic Pathway. Source data are provided as a Source Data file.
We used the climate scenarios CMIP633 from the 2021 sixth assessment report of the IPCC2—termed the Shared Socioeconomic Pathway (SSP), to estimate future OSA burden for different levels of global warming. We downloaded daily temperatures from 2023 to 2100 projections for 4 SSPs (SSP126, SSP245, SSP370, SSP585), based on 27 climate models from multiple countries and climate modelling groups. In the 29 studied countries, a ~ 1.8°C increase in global ambient temperatures above pre-industrial levels (SSP126 by 2100) was associated with in a ~ 15% increase in wellbeing burden compared to 2023 estimates (Table S3). Scenarios with projected increased temperature higher than SSP126 were estimated to further increase the wellbeing burden by 10 to 30% by 2050, and 1.5 to 2.5-fold by 2100, depending on the country (Fig. 3b). Temperatures higher than 1.8 °C above pre-industrial levels were estimated to incur an additional 12 to 36 million YLDs, 0.5 to 1.3 million YLLs, and an associated cost of 1.0 −2.8 trillion USD, over the 2023 to 2100 period. Country by country rates of DALYs per 100,000, absolute number of YLLs, absolute numbers of YLDs, and associated economic cost persons under different scenarios in 2050 and 2100 are presented in Tables S3 to S6. Accounting for population forecast and a potential 30% increase in OSA prevalence by 2050 due to rise in obesity34 would further increase these estimates in most countries by 10 to 25%. Comparison of the main model estimates vs. the alternative scenario is available in Tables S7 and S8. Under these assumptions, any other scenario than SSP126 would be estimated to incur an additional 16.9 to 47.4 million DALYs lost over the 2023 to 2100 period.
Workplace productivity burden of warming-related increase in OSA prevalence
OSA has a considerable impact on productivity and is associated with increased likelihood of absenteeism and presenteeism (being at work but not functioning at full capacity)22,35. The calculated increase in OSA prevalence from global warming is estimated to incur additional productivity losses (Fig. 4). In 2023, for the 29 studied countries, the increase in OSA prevalence due to higher temperatures was associated with an additional 80 million presenteeism days (59 to 101 million) and an additional 25 million absenteeism days (12 to 38 million). The total economic cost of this loss of labor was 30 (21 to 40) billion USD. Globally, the rate of labor loss in 2023 was 8.4 (5.7 to 11.1) million USD per 100,000 persons and was double the rate of labor loss of 2000 (4.0 [2.7 to 5.2] million USD; see Table S7).

Calculated labor loss (in USD) for different climate scenarios from the Intergovernmental Panel on Climate Change (IPCC) (top) with different levels of future global warming over the 29 studied countries per (a) 100,000 people (mean and 95%CI across countries); (b) year. Cumulative sum of (c) absenteeism days, (d) presenteeism days, and (e) associated economic cost for different climate scenarios over the 2023–2100 period. Rates of (f) absenteeism (g) presenteeism, and (h) labor loss in 2100 per 100,000 people under different climate scenarios for the 29 studied countries. USD: US dollars; SSP: Shared Socioeconomic Pathway. Source data are provided as a Source Data file.
Scenarios with projected increased temperatures higher than 1.8 °C (SSP126) above pre-industrial levels are expected to increase labor loss by 10 to 25% by 2050, and 1.3- to 2.2-fold by 2100, depending on the country (Fig. 4; Tables S10, S11). These scenarios are projected to incur an additional cost of 0.9 to 2.0 trillion USD in labor loss over the 2023 to 2100 period (Fig. 4). In 2100, the labor loss rates per year for different climate models in the 29 studied countries are projected to be 37 billion (10.0 million per 100,000 - SSP126), 50 billion (13.3 million per 100,000 - SSP245), 69 billion (18.4 million per 100,000 - SSP370) and 84 billion (22.8 million per 100,000 - SSP545), see Tables S10 and S11. Country by country rates and absolute numbers of labor loss for different climate scenarios in 2050 and 2100 are presented in Tables S10 and S11.
Discussion
High ambient temperatures (99th vs. 25th; 27.3 vs. 6.4 °C) are associated with a ~ 45% increase in the probability of having OSA on a given night, globally. The increase in OSA prevalence in 2023 due to global warming was associated with a loss of 788,198 (489,226 to 1,087,170) healthy life years, and a productivity loss of ~105 million days from impaired workplace attendance in the 29 studied countries. In 2023 alone, the estimated total economic cost associated with the warming-related increase in OSA prevalence was ~98 billion USD, including 68 (34 to 102) billion USD from additional wellbeing burden and 30 (21 to 40) billion USD from workplace productivity loss.
Modelled temperatures consistent with the continuation of government climate change policies implemented by 2020 are projected to lead to global warming of 2.1 to 3.4 °C by 21002,36. The health and economic impact of these estimates would be consequential, and the increase in OSA prevalence due to rising temperatures in such scenario may double the overall OSA burden. Indeed, rates of DALYs, without considering temperature, for OSA in 2019 in Australia were already ~200 to 260 DALYs per 100,00022. Estimated 2100 rates of DALYs observed for most countries under SSP245 ( ~ 2.8 °C degrees of warming) were also around 150 to 300 DALYs per 100,000 people depending on the country, which would approximately double the current OSA burden. A previous, not yet peer reviewed, study also estimated a 122 billion USD wellbeing cost due to warming-related increase in short sleep prevalence18. Together, these studies highlight the economic burden associated with sleep-related inadequacy from rising temperatures. In addition, these estimates contribute to the growing body of evidence that investment to limit global warming would be a cost-effective strategy to prevent climate-related sleep impairment and its consequences37,38.
The sample used in this study likely under-represents lower socioeconomic groups, given that all participants owned a consumer-grade sleep tracking device, and most participants resided in highly developed countries. Hence, participants may have also had access to more favorable sleeping environments and heat stress-mitigation strategies such as air conditioning, which are less readily available in lower socioeconomic populations39. There are large global inequalities in availability of population sleep health data—with only 22% WHO member states (mostly highly developed) having published population data in sleep duration40. Similarly, published global estimates of OSA prevalence are derived from population studies in mostly high socio-economic countries19. Our study is also biased towards higher socioeconomic countries and highlights the urgent need for global strategies to collect appropriate sleep and temperature data worldwide40. In addition, 77% of the participants in the current study were male. We did not detect a large difference between sex in the temperature-OSA association. However, this study sample may not be representative of the wider general population and does not resolve the long-standing issue in sleep research of under-representation of female in such analyses.
Furthermore, since we lacked access to precise geographical locations and the indoor temperature of users, exact temperature-related effects could not be calculated. The potential confounding effect of air pollution on the association between high temperature and nightly OSA status may also have been underestimated since we lacked precise geographical locations and indoor measurements of air pollution. We also lacked clinical information on participants’ co-morbidities, treatment status, daytime symptoms, and impairments, and thus, could not explore potential modifiable effects of these conditions and symptoms on the detected association. Individuals with OSA and daytime sleepiness are at much greater risk of motor-vehicle accidents compared to those with OSA alone41. Hence, the temperature-related burden of OSA may be greater in this specific population. This aligns with previous studies that indicate that sleep loss and ambient temperature disproportionately affect more vulnerable populations16,17. High ambient temperatures have also been found to exacerbate the severity of chronic diseases42. Thus, further consideration of co-morbidities and daytime symptoms associated with OSA is warranted to better determine the impact of ambient temperature on OSA in vulnerable populations, and the additional burden this may incur. Although our robust time-series analysis design provides support for a potential causal association between high temperature exposure and increased OSA prevalence, other time-varying confounders (e.g., alcohol intake) were not available in the current study, and should be accounted for in further studies.
The under-mattress sensor used in this study does not measure the contribution of some physiological aspects of OSA (e.g., hypoxia, arousals) which may undermine OSA detection. However, existing validation studies versus gold standard polysomnography in over 150 participants28,43 support the device performance characteristics. Furthermore, OSA prevalence estimates using non-contact multi-night data found in this study yield very similar findings to previously published literature19,28. Similarly, previous studies that used this device have shown that misclassification rates and AHI variability are comparable to other devices30, and that the effect size of the association between the estimated AHI and health outcomes is also similar to existing epidemiological trials44,45. Furthermore, conventional single-night polysomnography can lead to inaccurate OSA diagnoses and severity estimation in 20 to 50% of patients due to high-night-to-night variability of OSA28,29,46. Thus, these studies provide support that the multi-night AHI estimates used in the current study provide comparable or superior insight to conventional single-night polysomnography AHI while being less cumbersome and allowing nightly data collection over ~1.5 years per individual.
Our main analysis aimed to model rising temperature’s impact on OSA-related wellbeing and productivity by holding other factors constant. However, BMI is projected to increase over the next 50 years, likely leading to higher OSA prevalence34. This suggests our main estimates may understate the future temperature-related OSA burden. Indeed, once accounting for BMI-related increase in OSA prevalence in our sensitivity analyses, our estimates were 10 to 30% higher. On the other hand, recent developments in OSA treatment47, including FDA-approved weight loss medications48, could help manage OSA more effectively. Given that approximately 80% of OSA patients are currently undiagnosed or untreated49, improved treatment rates could serve as an adaptation mechanism to offset temperature-induced increases in OSA burden. We also assumed constant heat adaptation at the population level. However, heat-related mortality in Europe has declined over the past two decades50, and global air conditioning adoption has increased from 19.3% (2000) to 35.3% (2021). Studies that have investigated heat adaptation strategies and its effects on sleep and OSA are scarce15. Thus, we could not account for heat adaptation. In addition, heat adaptation is not uniform: highly developed countries have 44-48% household air conditioning coverage, while low and medium developed countries have 4% and 14%, respectively51. Accordingly, given our sample’s socioeconomic bias toward developed nations, we likely underestimate the global impact of temperature-induced OSA, even without accounting for increased adaptation capabilities.
In conclusion, our study underscores the potential significant impact of increasing ambient temperatures on the prevalence of OSA, globally. Without substantially greater policy change to slow global warming, the health and economic burdens associated with OSA may double by 2100. These results highlight the urgency of limiting global warming to 1.5 °C above pre-industrial levels, in alignment with the Paris Agreement. Our findings also emphasize the immediate need for targeted measures to potentially minimize the health and economic impacts of the growing OSA prevalence associated with rising temperatures.
Methods
The current study was approved by the Flinders University Human Research Ethics Committee (Project number: 4291). This study complies with the recommendations of the GATHER statement52, and GATHER checklist can be found at the end of supplementary materials.
Participants
Retrospective data were acquired from 125,295 participants who registered to use an under-mattress sleep sensor (Withings Sleep Analyzer/Sleep Rx; WSA) between January 2020 and September 2023. To be included in this analysis, participants were required to have ≥28 nights of data and an average of ≥4 sleep recordings per week. When participants sign-up to the Withings app, they are prompted to fill in their age, sex, height, and weight. Information on gender is not collected. Participants were required to be 18 years or older to be included in this study. Participants were geo-localized to the closest city within a given time zone. A more precise ___location was not available due to concern for re-identification and privacy. All participants provided written consent through the Withings app for their deidentified data to be used for research purposes when signing up for a Withings account.
Country level information
Country level GDP per capita and GDP per capita employed were collected from the World Bank (https://data.worldbank.org/indicator/NY.GDP.PCAP.CD). Population and life expectancy estimates were based on the United Nations World 2024 Populations Prospects report53.
Objective OSA monitoring
The WSA is a FDA-cleared sleep monitoring device placed under the mattress that estimates sleep timing, quality, and breathing using ballistography and sound data (FDA 510(k) number: K231667)43. WSA-derived sleep duration, timing, and AHI have good agreement against polysomnography in multiple independent validation studies28,43,54. The WSA-estimated AHI also shows good agreement with in-laboratory polysomnography-derived AHI to classify moderate-to-severe OSA (88% sensitivity and 88% specificity to detect ≥15 events/h during sleep)28,43. The AHI cannot be reliably calculated for nights with a sleep duration of less than five hours43, and these nights were excluded from analysis. Our primary outcome of interest was the nightly OSA status for a given participant on a given night, based on the AHI and clinically defined severity categories (nightly OSA: AHI ≥ 15; and nightly severe OSA: AHI ≥ 30 event/h). For each participant, we also calculated the average OSA severity category based on the average AHI on all available nights and using pre-defined clinical cut-offs (mild: 5–15; moderate: 15–30 and severe: ≥30 events/h). The prevalence of OSA per country was calculated based on the average OSA severity category for each participant.
Assessment of weather information and climate projections
Weather information was time-matched for each day of data for every user based on their closest ___location, collected from the Copernicus Climate Change Service55. We extracted and calculated 24 h minimum, maximum, and average daily temperature as well as total cloud cover, surface pressure, and relative humidity from the fifth generation of ERA5 dataset31. We extracted fine particulate matter (aerodynamic diameter <2.5 µm) concentration from the ECMWF Atmospheric Composition Reanalysis 4 model as a measure of air quality56. These re-analysis models have been validated against station-based measurements57,58,59 and are widely applied in environmental health research57,58,60. We used the climate scenarios CMIP633 from the 2021 sixth assessment report of the IPCC2. We downloaded daily temperatures from 2023 to 2100 projections for 4 SSPs (SSP126, SSP245, SSP370, SSP585), based on 27 climate models from multiple countries and climate modelling groups. Averaged daily projections were calculated as the daily median of the 27 projections. Detailed information on pre-processing and weather variable extraction can be found in the Supplementary Methods.
Statistical analysis
Non-linear fixed effect models were used to study the effects of 24 h average ambient temperature on nightly OSA status on the following night, defined as an AHI ≥ 15 events/h for that night. We followed the recently proposed case-time series methodology61 which has been used extensively in environmental health studies42,62,63,64,65, including in our previous study estimating the effect of high ambient temperature on sleep18. We used participant/year/month strata intercepts, natural splines of time (day of the year; with 4 degrees of freedom [df]), and indicators of the day of the week to model individual baseline risks, in addition to shared long-term, seasonal, and weekly trends. Models were further adjusted for total cloud cover (4 df), relative humidity (4 df), density of particulate matter with aerodynamic diameter <2.5 µg/m3 (4 df), surface pressure (4 df), total precipitation (4 df), wind speed (4 df) and variation in total sleep time (4 df) as these potential confounders may have effects on OSA prevalence within the 1-month stratum27.
The exposure-response association of interest between temperature and nightly OSA status was modelled using distributed lags9,66. We primarily chose a 4-day lag structure since the effect of temperature on sleep duration was shown to be significant up to the fourth day18. Other lag structures were explored but made little difference to the main findings (see Supplementary Methods and Supplementary Figs. 7 and 8). Similar to previous studies on the effect of temperature on health9,10,13,66, we used the sum of the effect over the lag period to summarize the association between temperature and nightly OSA status. This analytic approach was conducted on the complete dataset, and in independent analyses stratified by country. Further analyses examined specific subgroups of interest, including age groups (10-year categories), sex, BMI categories, habitual sleep duration categories (average sleep duration over the recording period), and tertiles of GDP per capita. The above analyses also estimated the association between ambient temperature and severe OSA (AHI ≥ 30 events/h) prevalence rates. Models are summarized using RR [95%CI], calculated from the odds ratio using existing formula67. We used the R programming language (version 4.3.3), specifically with the dlnm68 (version 2.4.7) and gnm69 packages (version 1.1-5). Sensitivity analyses were conducted, and the analysis was repeated by using minimum 24h-average temperature and maximum 24h-average temperature to further validate our findings. We also conducted a sensitivity analysis to investigate potential bias due to missing data when users are sleeping less than five hours. In this sensitivity analysis, we calculated the exposure-response curve between temperature and nightly OSA for each quartile of missing data proportion (determined per-participant).
Calculation of the global warming-related increase in nightly OSA prevalence
For each country, we calculated the difference in temperature for a given year compared to the 1950–1990 historical average temperature (see Fig. 5a for an example in the UK). This difference in temperature was used to calculate the change in the probability of having OSA between a given calendar year (e.g., 2022) versus historical data, which was subsequently transformed into a RR. Using this RR, we calculated the relative change in nightly OSA prevalence associated with global warming-related increased temperatures for each calendar day (in person-days) for that specific year and country. This approach was repeated for each ___location and each calendar day between 1950 and 2100, as well as for each tested climate projection.

a The difference in temperature for a given year (here 2023—black solid line) was compared to the 1950–1990 historical average temperature (dashed red line). b This difference in temperature (blue arrow) was used to calculate the change in the risk of nightly OSA between current vs. historical average temperature, for a particular day. This daily change was summed over the year and used to calculate the associated wellbeing and workplace productivity burden (see text for further details). Figure 5b represents the cumulative exposure–response (and 95%CI in shaded area) between ambient temperature and nightly OSA in the UK. Source data are provided as a Source Data file.
Wellbeing burden modelling
DALYs are a standardized summary measure employed by the World Health Organization and the GBD studies32 to quantify the impact of illness, injury, and/or dying prematurely. DALY combines time lost due to premature death (YLL) and time lived with less than-optimal health (YLD). DALYs measures have been used to assess the effect of temperature on health in other studies70,71. For this study, we followed the methodology previously used to assess the wellbeing burden of OSA in Australia22,72 and our previous report on the global wellbeing burden of reduced sleep duration18. DALYs, YLLs, and YLDs were quantified using the calculated warming-related person-days increase in OSA prevalence (see previous section) and published literature on associations between OSA and health outcomes.
Given the well-established association between OSA and motor-vehicle accidents, we estimated the years of life lost (YLL) due to increased motor vehicle accidents associated with the warming-related increase in OSA prevalence. We also estimated temperature-related OSA effects on other conditions that may induce less-than-optimal health and hence increase the number of YLD. In our study, we based these estimates for the YLD using data from a previous studies22,72. More formally, \({{YLL}}_{c,y}\) for a given country c at a year y was calculated as follows:
where \({{MVA}}_{{{death\_rate}}_{c}}\) is the daily rate of fatal motor vehicle accidents for a given country c, extracted from the GBD73; \({{RR}}_{{MVA\_OSA}}\) is the daily RR of fatal motor vehicle accidents associated with OSA, here estimated to be 100% based on previous literature21,41,74,75,76; \({{RR}}_{c}\) is the daily RR function for OSA function for a given country c; \({{Thist}}_{d,1950-90}\) is the average historical temperature (1950–1990; Fig. 5a red) for a particular day of the year (1–365); \({T}_{d,y}\) is the temperature for a particular day of the year d and a year y; \({p0}_{c}\) is the prevalence of OSA for a given country c; and \({{APOP}}_{c,y}\) is the given adult population for a country c in year y; \({{RLE}}_{c}\) is the average years of life lost for a given fatal motor vehicle accident for a country c, also extracted from the GBD73. Uncertainty intervals for YLLs were constructed using an \({{RR}}_{{MVA\_OSA}}\) of 50% (lower bound) and 150% (upper bound), using 100% as the mean.
Similarly, \({{YLD}}_{c,y}\) can be calculated as follows:
where DW is the daily disability weight associated with OSA, and was estimated to be between 0.05–0.11 based on previous literature22,72. Uncertainty intervals for YLDs were constructed using a disability weight of 0.05 (lower bound) and 0.11 (upper bound), using 0.08 as the mean. L is the duration of the “diseases/impairment” associated with OSA on a given day. Here, we conservatively assumed this duration to be 1 day, similar to a previous study on quality of life lost to heatwaves in Japan77. Other terms are similar to the calculation of \({{YLL}}_{c,y}\). Finally, \({{DALY}}_{c,y}\) can be calculated as follows:
The economic cost of wellbeing loss can be calculated using estimated values of DALYs. Here we used values of one time (lower bound), two times (mean) and three times (upper bound) GDP per capita (2023 USD) as proxies for the value of a DALY, as used in previous studies78,79. In our primary model, to isolate the effect of temperature on DALY modelling, we fixed the prevalence of OSA and population per country to a constant number (2023 estimate) until 2100. However, in a sensitivity analysis, we account for these factors using population forecasts from the UN world prospect 2024 and using projection on increased OSA prevalence (30% increase by 2050) due to increased obesity34.
Workplace productivity loss modelling
Sleep disorders have a considerable impact on productivity and are associated with increased likelihood of absenteeism and presenteeism (being at work but not functioning at full capacity)80. On average, people with OSA report five additional days of sick leave per year, relative to people without OSA, and spend 6.8% of their working days with reduced productivity22,35. The additional absenteeism and presenteeism due to the increase in OSA prevalence days were quantified using similar methodology to the wellbeing burden in the previous section. The overall labor loss was then calculated by adding absenteeism and presenteeism days and multiplying by the average gross domestic product per capita employed. Presenteeism and absenteeism days for a given country c and year y can be calculated as follows:
where \({NWD}\) is the number of working days per person on a given year for a full-time employee, here assumed to be 235 (assuming 5 weeks of annual leave). \({{PRES}}_{{rate}}\) and \({{ABS}}_{{rate}}\) is the daily absenteeism on presenteeism rate (2.1% and 6.8% for absenteeism and presenteeism, respectively). \({{LF}}_{c}\) is the labor force for a given country c in 2023, downloaded from the World Bank. Since labor force estimates do not account for part-time labor, we weighted overall labor force using estimate of part-time worker percentage from the World Bank. We multiplied labor force population by half the percentage of part time employment (assuming part-time employment is 50% full time equivalent) and subtracted it to the overall labor force. The overall labor loss was then calculated as follows:
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The dataset associated with this study is stored in a proprietary repository (Withings) and cannot be shared publicly due to concern for privacy, ethical and legal reasons. The investigator team accessed the data through an application process to Withings, and a formal data sharing agreement designed to safeguard user confidentiality, as outlined in the terms and conditions and privacy policy documentation. Queries for data access can be directed to Withings ([email protected]) with a timeframe for response of four weeks. Specific de-identified raw data that support the findings of this study, including individual data, are available from the corresponding author ([email protected]) upon request subject to ethical and data custodian (Withings) approval described above. The timeframe for response to requests will be up to four weeks. ERA5 weather data and climate model projections are freely available from the Copernicus data store (https://cds.climate.copernicus.eu/). Information on country GDP, rate of motor vehicle accident, and population number are freely available from the world bank (https://www.worldbank.org/ext/en/home), the UN world population prospect (https://population.un.org/wpp/), and the GBD. Exposure-response curve between temperature and OSA RR derived in this study are available on GitHub: https://github.com/bastienlechat/OSA_climate. Wellbeing and economic projection modelling for each country is also available on GitHub: https://github.com/bastienlechat/OSA_climate. Source data are provided with this paper.
Code availability
Code to reproduce the figures, wellbeing projections and economic projections are all available on GitHub: https://github.com/bastienlechat/OSA_climate.
References
Esper, J., Torbenson, M. & Büntgen, U. 2023 summer warmth unparalleled over the past 2,000 years. Nature. https://doi.org/10.1038/s41586-024-07512-y (2024).
IPCC. IPCC, 2023: Climate Change 2023: Synthesis Report. Contribution of Working Groups I, II and III to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change. (IPCC, Geneva, Switzerland, (2023).
Romanello, M. et al. The 2023 report of the Lancet Countdown on health and climate change: the imperative for a health-centred response in a world facing irreversible harms. Lancet 402, 2346–2394 (2023).
Bell, M. L., Gasparrini, A. & Benjamin, G. C. Climate Change, Extreme Heat, and Health. N. Engl. J. Med 390, 1793–1801 (2024).
Obradovich, N., Migliorini, R., Paulus, M. P. & Rahwan, I. Empirical evidence of mental health risks posed by climate change. Proc. Natl Acad. Sci. 115, 10953–10958 (2018).
Thompson, R., Hornigold, R., Page, L. & Waite, T. Associations between high ambient temperatures and heat waves with mental health outcomes: a systematic review. Public Health 161, 171–191 (2018).
Nori-Sarma, A. et al. Association Between Ambient Heat and Risk of Emergency Department Visits for Mental Health Among US Adults, 2010 to 2019. JAMA Psychiatry 79, 341–349 (2022).
Obradovich, N. & Fowler, J. H. Climate change may alter human physical activity patterns. Nat. Human Behav. 1, https://doi.org/10.1038/s41562-017-0097 (2017).
Gasparrini, A. et al. Mortality risk attributable to high and low ambient temperature: a multicountry observational study. Lancet 386, 369–375 (2015).
Ballester, J. et al. Heat-related mortality in Europe during the summer of 2022. Nat. Med. 29, 1857–1866 (2023).
He, C. et al. Cause-specific accidental deaths and burdens related to ambient heat in a warming climate: A nationwide study of China. Environ. Int 180, 108231 (2023).
Masselot, P. et al. Excess mortality attributed to heat and cold: a health impact assessment study in 854 cities in Europe. Lancet Planet Health 7, e271–e281 (2023).
Alahmad, B. et al. Associations Between Extreme Temperatures and Cardiovascular Cause-Specific Mortality: Results From 27 Countries. Circulation 147, 35–46 (2023).
Lee, H., Myung, W., Kim, H., Lee, E. M. & Kim, H. Association between ambient temperature and injury by intentions and mechanisms: A case-crossover design with a distributed lag nonlinear model. Sci. Total Environ. 746, 141261 (2020).
Chevance, G. et al. A systematic review of ambient heat and sleep in a warming climate. Sleep Med. Rev. https://doi.org/10.1016/j.smrv.2024.101915 (2024).
Minor, K., Bjerre-Nielsen, A., Jonasdottir, S. S., Lehmann, S. & Obradovich, N. Rising temperatures erode human sleep globally. One Earth 5, 534–549 (2022).
Obradovich, N., Migliorini, R., Mednick, S. C. & Fowler, J. H. Nighttime temperature and human sleep loss in a changing climate. Sci. Adv. 3, e1601555 (2017).
Lechat, B. et al. O011 Loss of sleep due to high ambient temperatures and its impact on healthy life years: Implications for global warming. Sleep. Adv. 5, A5–A5 (2024).
Benjafield, A. V. et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir. Med 7, 687–698 (2019).
Redline, S., Azarbarzin, A. & Peker, Y. Obstructive sleep apnoea heterogeneity and cardiovascular disease. Nat. Rev. Cardiol. https://doi.org/10.1038/s41569-023-00846-6 (2023).
Bonsignore, M. R. et al. European Respiratory Society statement on sleep apnoea, sleepiness and driving risk. Eur. Respir. J. 57, https://doi.org/10.1183/13993003.01272-2020 (2021).
Economics, D. A. Rise and try to shine: The social and economic cost of sleep disorders In Australia. (Sleep Health Foundation, 2021).
Watson, N. F. Health Care Savings: The Economic Value of Diagnostic and Therapeutic Care for Obstructive Sleep Apnea. J. Clin. Sleep. Med. 12, 1075–1077 (2016).
Li, A. et al. Higher ambient temperatures may worsen obstructive sleep apnea: A nationwide smartwatch-based analysis of 6.2 million person-days. Sci. Bull. (Beijing) https://doi.org/10.1016/j.scib.2024.05.016 (2024).
Weinreich, G. et al. Association of short-term ozone and temperature with sleep disordered breathing. Eur. Respir. J. 46, 1361–1369 (2015).
Zanobetti, A. et al. Associations of PM10 with sleep and sleep-disordered breathing in adults from seven U.S. urban areas. Am. J. Respir. Crit. Care Med 182, 819–825 (2010).
Lechat, B. et al. Seasonal and Weekly Variability in OSA Severity [abstract]. Am. J. Respir. Crit. Care Med 209, A2987 (2024).
Lechat, B. et al. Multinight Prevalence, Variability, and Diagnostic Misclassification of Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med 205, 563–569 (2022).
Punjabi, N. M., Patil, S., Crainiceanu, C. & Aurora, R. N. Variability and Misclassification of Sleep Apnea Severity Based on Multi-Night Testing. Chest 158, 365–373 (2020).
Lechat, B. et al. Multi-night measurement for diagnosis and simplified monitoring of obstructive sleep apnoea. Sleep. Med Rev. 72, 101843 (2023).
Muñoz-Sabater, J. et al. ERA5-Land: a state-of-the-art global reanalysis dataset for land applications. Earth Syst. Sci. Data 13, 4349–4383 (2021).
Collaborators, G. B. D. R. F. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 396, 1223–1249 (2020).
O’Neill, B. C. et al. The Scenario Model Intercomparison Project (ScenarioMIP) for CMIP6. Geoscientific Model Dev. 9, 3461–3482 (2016).
Boers, E. et al. An Estimate of the Prevalence of Obstructive Sleep Apnea in the United States into 2050. Am J. Resp. Crit. Care 209, https://doi.org/10.1164/ajrccm-conference.2024.209.1_MeetingAbstracts.A3895 (2024)
Bailly, S. et al. Impact of CPAP Termination on Permanent Work Disability in Obstructive Sleep Apnea: A French Nationwide ALASKA Database Analysis. Ann. Am. Thorac. Soc. https://doi.org/10.1513/AnnalsATS.202404-389OC (2024).
Core Writing Team, H. L. a. J. R. e. IPCC, 2023: Climate Change 2023: Synthesis Report. Contribution of Working Groups I, II and III to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change. (Geneva, Switzerland, 2023).
Kotz, M., Levermann, A. & Wenz, L. The economic commitment of climate change. Nature 628, 551–557 (2024).
Glanemann, N., Willner, S. N. & Levermann, A. Paris Climate Agreement passes the cost-benefit test. Nat. Commun. 11, 110 (2020).
Davis, L., Gertler, P., Jarvis, S. & Wolfram, C. Air conditioning and global inequality. Glob. Environ. Change 69, https://doi.org/10.1016/j.gloenvcha.2021.102299 (2021)
Lim, D. C. et al. The need to promote sleep health in public health agendas across the globe. Lancet Public Health 8, e820–e826 (2023).
Gottlieb, D. J., Ellenbogen, J. M., Bianchi, M. T. & Czeisler, C. A. Sleep deficiency and motor vehicle crash risk in the general population: a prospective cohort study. BMC Med 16, 44 (2018).
Zhang, Z. et al. Ambient heat exposure and kidney function in patients with chronic kidney disease: a post-hoc analysis of the DAPA-CKD trial. Lancet Planet Health 8, e225–e233 (2024).
Edouard, P. et al. Validation of the Withings Sleep Analyzer, an under-the-mattress device for the detection of moderate-severe sleep apnea syndrome. J. Clin. Sleep. Med https://doi.org/10.5664/jcsm.9168 (2021).
Lechat, B. et al. High night-to-night variability in sleep apnea severity is associated with uncontrolled hypertension. NPJ Digit Med 6, 57 (2023).
Lechat, B. et al. Single-Night Diagnosis of Sleep Apnea Contributes to Inconsistent Cardiovascular Outcome Findings. Chest 164, 231–240 (2023).
Roeder, M. et al. Night-to-night variability of respiratory events in obstructive sleep apnoea: a systematic review and meta-analysis. Thorax 75, 1095–1102 (2020).
Pépin, J.-L., Eastwood, P. & Eckert, D. J. Novel avenues to approach non-CPAP therapy and implement comprehensive obstructive sleep apnoea care. Eur. Respir. J. 59, https://doi.org/10.1183/13993003.01788-2021 (2022).
Malhotra, A. et al. Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity. N. Engl. J. Med 391, 1193–1205 (2024).
Kapur, V. et al. Underdiagnosis of sleep apnea syndrome in U.S. communities. Sleep. Breath. 6, 49–54 (2002).
Gallo, E. et al. Heat-related mortality in Europe during 2023 and the role of adaptation in protecting health. Nat. Med 30, 3101–3105 (2024).
Romanello, M. et al. The 2024 report of the Lancet Countdown on health and climate change: facing record-breaking threats from delayed action. Lancet. https://doi.org/10.1016/S0140-6736(24)01822-1 (2024)
Stevens, G. A. et al. Guidelines for Accurate and Transparent Health Estimates Reporting: the GATHER statement. Lancet 388, e19–e23 (2016).
United Nations, D. o. E. a. S. A., Population Division. World Population Prospects 2024, Online Edition, https://population.un.org/wpp/.
Scott, H. et al. Sleep Irregularity Is Associated With Hypertension: Findings From Over 2 Million Nights With a Large Global Population Sample. Hypertension 80, 1117–1126 (2023).
Copernicus Climate Change Service (C3S) Climate Data Store (CDS). Copernicus Climate Change Service (2022): ERA5-Land hourly data from 1950 to present.
Inness, A. et al. The CAMS reanalysis of atmospheric composition. Atmos. Chem. Phys. 19, 3515–3556 (2019).
Urban, A. et al. Evaluation of the ERA5 reanalysis-based Universal Thermal Climate Index on mortality data in Europe. Environ. Res 198, 111227 (2021).
Mistry, M. N. et al. Comparison of weather station and climate reanalysis data for modelling temperature-related mortality. Sci. Rep. 12, 5178 (2022).
Gueymard, C. A. & Yang, D. Worldwide validation of CAMS and MERRA-2 reanalysis aerosol optical depth products using 15 years of AERONET observations. Atmosp. Environ. 225, https://doi.org/10.1016/j.atmosenv.2019.117216 (2020).
Requia, W. J., Amini, H., Mukherjee, R., Gold, D. R. & Schwartz, J. D. Health impacts of wildfire-related air pollution in Brazil: a nationwide study of more than 2 million hospital admissions between 2008 and 2018. Nat. Commun. 12, 6555 (2021).
Gasparrini, A. The Case Time Series Design. Epidemiology 32, 829–837 (2021).
Gasparrini, A. A tutorial on the case time series design for small-area analysis. BMC Med Res Methodol. 22, 129 (2022).
Jones, P. J. et al. Characterising non-linear associations between airborne pollen counts and respiratory symptoms from the AirRater smartphone app in Tasmania, Australia: A case time series approach. Environ. Res 200, 111484 (2021).
Sun, Y. et al. Short term exposure to low level ambient fine particulate matter and natural cause, cardiovascular, and respiratory morbidity among US adults with health insurance: case time series study. BMJ 384, e076322 (2024).
Quilty, S. et al. The relative value of sociocultural and infrastructural adaptations to heat in a very hot climate in northern Australia: a case time series of heat-associated mortality. Lancet Planet Health 7, e684–e693 (2023).
Gasparrini, A. Modeling exposure-lag-response associations with distributed lag non-linear models. Stat. Med 33, 881–899 (2014).
Zhang, J. & Yu, K. F. What’s the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA 280, 1690–1691 (1998).
Gasparrini, A. Distributed Lag Linear and Non-Linear Models in R: The Package dlnm. J. Stat. Softw. 43, 1–20 (2011).
gnm: Generalized Nonlinear Models. (Version 1.1-5) [Computer software]. (2023).
Liu, J. et al. Estimating the burden of disease attributable to high ambient temperature across climate zones: methodological framework with a case study. Int J. Epidemiol. 52, 783–795 (2023).
Burkart, K. G. et al. Estimating the cause-specific relative risks of non-optimal temperature on daily mortality: a two-part modelling approach applied to the Global Burden of Disease Study. Lancet 398, 685–697 (2021).
Economics, D. A. Asleep on the job Costs of inadequate sleep in Australia. (Sleep Health Foundation, 2017).
Spencer, L. J. et al. Morbidity and mortality from road injuries: results from the Global Burden of Disease Study 2017. Inj. Prev. 26, i46 (2020).
Garbarino, S., Pitidis, A., Giustini, M., Taggi, F. & Sanna, A. Motor vehicle accidents and obstructive sleep apnea syndrome: A methodology to calculate the related burden of injuries. Chron. Respir. Dis. 12, 320–328 (2015).
Tregear, S., Reston, J., Schoelles, K. & Phillips, B. Obstructive sleep apnea and risk of motor vehicle crash: systematic review and meta-analysis. J. Clin. Sleep. Med 5, 573–581 (2009).
Mulgrew, A. T. et al. Risk and severity of motor vehicle crashes in patients with obstructive sleep apnoea/hypopnoea. Thorax 63, 536–541 (2008).
Ihara, T., Narumi, D., Fukuda, S., Kondo, H. & Genchi, Y. Loss of disability-adjusted life years due to heat-related sleep disturbance in the Japanese. Sleep. Biol. Rhythms 21, 69–84 (2023).
Arias, D., Saxena, S. & Verguet, S. Quantifying the global burden of mental disorders and their economic value. EClinicalMedicine 54, 101675 (2022).
Bertram, M. Y. et al. Cost-effectiveness thresholds: pros and cons. Bull. World Health Organ 94, 925–930 (2016).
Reynolds, A. C. et al. Insomnia and workplace productivity loss among young working adults: a prospective observational study of clinical sleep disorders in a community cohort. Med J. Aust. 219, 107–112 (2023).
Acknowledgements
D.J.E. is supported by a National Health and Medical Research Council (NHMRC) of Australia Leadership Fellowship (1196261). B.L. is supported by a NHMRC of Australia Emerging Leadership Fellowship (2025886). J.L.P. and S.B. are partly supported by the French National Research Agency in the framework of the “Investissements d’avenir” program (ANR-15-IDEX-02) and the “e-health and integrated care and trajectories medicine and MIAI artificial intelligence” Chairs of excellence from the Grenoble Alpes University Foundation; MIAI @ Grenoble Alpes, (ANR-19-P3IA-0003). The results contain modified Copernicus Climate Change Service information 2020. Neither the European Commission nor ECMWF is responsible for any use that may be made of the Copernicus information or data it contains. We acknowledge the World Climate Research Programme, which, through its Working Group on Coupled Modelling, coordinated and promoted CMIP6. We thank the climate modelling groups for producing and making available their model output, the Earth System Grid Federation (ESGF) for archiving the data and providing access, and the multiple funding agencies who support CMIP6 and ESGF.
Author information
Authors and Affiliations
Contributions
B.L., J.M., L.P., B.T., B.K. and D.J.E. developed the study concepts and aims. B.L., D.P.N. and J.M. performed the data extraction. B.L., B.T., D.P.N., J.M., A.C.R. and B.K. contributed to the data analysis. B.L., J.M., L.P., D.P.N., and D.J.E. drafted the manuscript. B.L., J.M. L.P., A.C.R., H.S., D.V., S.B., J.F., B.T., B.K., R.A., J.L.P., P.E., D.J.E. provided important insight on data analysis, interpretation and contributed to drafting and to the final version of the manuscript. All authors had full access to all the data in the study and accept responsibility to submit for publication.
Corresponding author
Ethics declarations
Competing interests
P.E. serves as a consultant for Withings. Outside the submitted work, B.L. has had research grants from Withings, Medical Research Future Fund and NHMRC. Outside the submitted work, D.J.E. has had research grants from Bayer, Apnimed, Takeda, Invicta Medical, Eli Lilly and Withings. D.J.E. currently serves as a scientific advisor/consultant for Apnimed, Invicta Medical, Takeda, SleepRes and Mosanna. A.C.R. has received research funding from the Lifetime Support Authority, Sleep Health Foundation, Flinders Foundation, Medical Research Future Fund, NHMRC, the Hospital Research Foundation, Compumedics, and Sydney Trains, and speaker and consultancy fees from Teva Pharmaceuticals, Sealy Australia, and the Sleep Health Foundation for work unrelated to this study. H.S. reports consultancy and/or research support from Re-Time Pty Ltd, Compumedics Ltd, the American Academy of Sleep Medicine Foundation, and Flinders University. R.J.A. reports research support from the NHMRC, Flinders Foundation, the Hospital Research Foundation, Big Health, Philips Respironics, ResMed Foundation, Flinders University, Sydney Trains and, and speaker and consultancy fees from SomnoMed. P.C. reports grants from NHMRC, Medical Research Future Fund, Flinders Foundation, Invicta Medical, Garnett Passe and Rodney Williams Memorial Foundation, Defence Science and Technology Group. None of the other authors have any potential conflicts to declare.
Peer review
Peer review information
Nature Communications thanks Martino F. Pengo and the other, anonymous, reviewers for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lechat, B., Manners, J., Pinilla, L. et al. Global warming may increase the burden of obstructive sleep apnea. Nat Commun 16, 5100 (2025). https://doi.org/10.1038/s41467-025-60218-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41467-025-60218-1
