
Abstract
Enhancing efficiency and productivity in countries’ healthcare systems is a global challenge. The Chinese government invested huge resources to improve the efficiency and productivity of the healthcare system across the country. To assess the success of the mission above, this research utilized DEA-SBM Meta frontier analysis alongside the Malmquist Productivity Index. These methodologies were employed to gauge Efficiency, production technology heterogeneity, and productivity of healthcare systems change across 31 mainland Chinese provinces and four distinct geographical regions throughout the study period spanning from 1997 to 2022. Results revealed that the mean efficiency score of China’s healthcare system is 0.7672. It indicates a growth potential of 23.28 percent in the operational efficiency of healthcare systems. The eastern region’s efficiency level (0.86917) is higher among all four regions. Zhejiang, Shandong, and Guangdong are the top three healthcare-efficiency performers. The technology gap ratio indicates that eastern regions witnessed a high TGR (0.9909), showing the country’s attainment of superior healthcare technologies. Beijing, Guangdong, Shanghai, Tianjin, and Zhejiang witnessed higher TGR values among all 31 mainland Chinese provinces. The total factor productivity index of the healthcare system witnessed a slight growth of 0.33%, with an average MI score of 1.0033. Efficiency change (EC) was found to be the main determinant of TFPC as technology change TC is less than EC. Moreover, the MI score of the Western region (1.033) is higher than the corresponding Eastern, northeastern, and central regions. Guizhou, Anhui, and Yunnan were found to be the top three performers in TFPC growth. Finally, the Kruskal–Wallis test confirmed the statistically significant difference among 4 Chinese regions for the healthcare system’s efficiency, TFPC, and TGR.
Similar content being viewed by others

Introduction
A country’s healthcare system is crucial in safeguarding its population’s health and society’s overall stability. A strong healthcare system is crucial for protecting public health1. Implementing preventive measures, ensuring timely diagnosis, and providing appropriate treatment significantly reduce disease prevalence and limit their transmission throughout communities2. Quality healthcare services have a direct impact on individuals’ quality of life. An efficient medical system guarantees prompt medical care, enhancing health outcomes and longer life expectancy. It helps to create a healthier and more productive populace, ultimately boosting the country’s economy3. A reliable healthcare system promotes social stability by tackling health inequalities and guaranteeing fair access to medical services for all individuals in society4. Regardless of the socio-economic level, everyone should have access to vital healthcare services to create a more fair and unified society5. During situations like natural catastrophes or pandemics, the significance of a well-equipped medical system is crucial. The organization offers essential infrastructure, resources, and specialized knowledge to efficiently address emergencies, thereby saving lives and reducing the impact on communities6.
A robust medical and health system fosters innovation and research in healthcare. Countries can enhance medical science, create novel medicines, and enhance healthcare practices by investing in medical research and development, resulting in improved patient results7. The quality of its Healthcare system greatly influences a country’s global reputation. Countries with advanced healthcare systems are usually seen in a positive light, drawing medical tourists and promoting diplomatic ties8. An efficient and productive Healthcare system of a country is crucial for promoting public health, improving quality of life, stimulating economic growth, maintaining social stability, and developing scientific innovation9. An efficient Healthcare system is known for its capacity to maximize resource utilization and reduce inefficiency, ensuring that resources are distributed efficiently to address the healthcare requirements of the population10. Efficiency is enhanced by optimizing administrative processes and workflows to minimize redundant paperwork and bureaucratic obstacles that can drain time and resources. Moreover, these systems focus on preventive care and health promotion measures to detect and manage health conditions early, thus averting expensive complications and easing the strain on healthcare resources11. Furthermore, efficient medical systems utilize technology and data analytics to enhance decision-making, optimize patient care, and pinpoint areas for enhancement. These systems aim to provide high-quality care by adopting evidence-based methods and continuous quality improvement initiatives. This approach helps optimize resource utilization and reduce waste by limiting unneeded procedures, tests, and interventions12.
Technological progress has greatly improved the efficiency and overall productivity of the healthcare system by incorporating electronic health records, telemedicine, and health information systems. It has streamlined communication and enhanced access to patient information13. Artificial intelligence and machine learning algorithms are enhancing decision-making processes by providing tailored treatment plans and resource allocation. Wearable technologies, remote monitoring tools, and mobile health applications enable individuals to actively manage their health, encourage preventive care, and lessen the strain on conventional healthcare institutions14. Overall, these innovations improve efficiency by enabling smooth information sharing, empowering patients and clinicians, and supporting data-driven decision-making in healthcare delivery15.
China has experienced significant advancements in its healthcare system in recent decades. The government has made substantial investments in infrastructure, healthcare facilities, and medical education, resulting in enhanced healthcare service accessibility for its extensive population16. Reforms have been put in place to broaden health insurance coverage, decrease financial obstacles to care, and enhance affordability for millions of people. China has adopted technical advancements like telemedicine and digital health platforms to improve healthcare services, particularly in distant and underdeveloped regions17. The country has prioritized enhancing its public health infrastructure through efforts targeting illness prevention, health promotion, and emergency preparedness. Despite progress, obstacles persist, such as discrepancies in healthcare access between urban and rural areas, an ageing population, and the growing burden of chronic diseases, which are influencing the development of China’s healthcare system18.
Further, evidence of regional disparities in technology adoption exists throughout China’s healthcare system, spanning its Eastern, Western, Central, and Northeastern regions. Eastern China, such as Shanghai, has advanced healthcare infrastructure and access to cutting-edge medical technologies19. In contrast, Western regions struggle with geographical remoteness and underdevelopment, leading to disparities in access to advanced healthcare services. The Central region shows varying levels of development, where metropolitan areas may have superior access to advanced medical technologies in comparison to rural areas in the same province20. In Northeastern China, disparities exist in healthcare infrastructure between major cities such as Shenyang, which have excellent facilities, and rural areas. It is essential to overcome these regional differences in technology adoption to guarantee fair access to high-quality healthcare services across21.
The Chinese government has introduced programs to improve efficiency and total factor productivity in resource utilization in the provincial healthcare system and to reduce disparities in technology usage among different regions. Total Factor Productivity (TFP) in China’s healthcare system measures the efficiency with which resources such as labor, technology, and financing are utilized to provide high-quality healthcare services. A high level of Total Factor Productivity (TFP) indicates that the system effectively converts these resources into improved health outcomes and services. Promoting the integration of digital technology and telemedicine platforms is a crucial initiative to enhance access to healthcare services, especially in neglected rural regions. The government promotes the adoption of electronic health records (EHRs) and digital health solutions in healthcare facilities by providing subsidies and incentives22. It helps to streamline administrative processes and support data-driven decision-making. Further investments in infrastructure development and medical education assist in reducing healthcare disparities between regions by ensuring all provinces have access to enough resources and trained specialists. The Chinese government encourages collaboration and knowledge sharing among provinces to improve efficiency and productivity in resource usage in the country’s healthcare system23. All these national and provincial efforts show China’s dedication to tackling regional inequalities and advancing fair access to high-quality healthcare services for all its population.
Nevertheless, the extent of achievement in endeavors aimed at substantially improving efficiency and productivity growth while reducing regional disparities in technological adoption within China’s provincial healthcare system remains undisclosed and merits investigation. Thus, this study initially employed the DEA-SMB model to assess the efficiency of the healthcare systems across 31 Chinese mainland provinces from 1997 to 2022. It estimates the aggregate level of success in the efficiency enhancement of China’s healthcare system over the study period. Further, it elaborates on the efficiency level of 4 different regions in China, namely Eastern, Western, Central, and Northeastern regions (see Fig. 1). Secondly, the study employed Meta-frontier analysis to measure the technological gap ratio (TGR) in all 4 regions of China. TGR explores the gaps in the adaptation and utilization of advanced technology in the regional healthcare system. Thirdly, the research utilizes the Malmquist productivity index to assess the TFPC within the healthcare system. TFPC illustrates the dynamic change over the study period in the productivity of China’s healthcare system. Moreover, it explores the main determinant (efficiency change or technology change) of TFPC. It is a significant indicator for health authorities to determine whether to enhance the efficiency or technology of the healthcare system of China. Finally, the study employed the Kruskal–Wallis test to measure the statistically significant difference among 4 different Chinese regions for Efficiency, TGR, and TFPC. The rest of the study is arranged as follows: Section “Literature review” presents the relevant literature review of the study. The methodology employed in the study is discussed in section “Methodology”. Section “Inputs-outputs selection and data collection” provides a depiction of the selection process for inputs and outputs as well as details regarding data collection. Following this, Section “Results and discussion” offers the results and discussion of the study. Lastly, Section “Conclusion and policy implications” encapsulates the conclusion and outlines the policy implications derived from the findings.

Regional distribution of China for healthcare systems.
Literature review
The efficiency and productivity change of healthcare systems are extensively evaluated around the globe. Gong et al.24 use Network Data Envelopment Analysis (DEA) to evaluate the efficiency of China’s healthcare system after the reform in its provinces. Tobit regression is used to determine significant factors. The results indicate that regional characteristics and government health spending have beneficial benefits, while high education enrollments, public hospital counts, and social health expenditures have negative effects. Top et al.11 evaluated the healthcare system efficiency in 36 African countries. The input variables consist of health expenditure, physician and nurse density, and hospital bed availability. Output variables include life expectancy and infant mortality rates. Results illustrate that approximately 58.33% of countries demonstrate efficiency, whereas Senegal was found to be inefficient. Tobit regression shows that nurse density and the Gini coefficient are important factors influencing inefficiency. Further, the study highlights the importance of efficiently using both public and private health resources to attain similar health results worldwide. Analyzing Indonesia’s healthcare system efficiency from 2014 to 2018 in 33 provinces was done using Data Envelopment Analysis (DEA)25. The input variables consist of health human resources, the quantity of hospitals and community health centers, and the per capita distribution of health funding. The Life Expectancy Index is the output variable. Efficient healthcare systems have been recognized in Lampung, West Java, Banten, West Nusa Tenggara, and West Sulawesi. Regional disparities are shown by low absorption of health reconcentration funding, leading to inefficiencies. Ibrahim and Daneshvar26 evaluated Lebanon’s healthcare system efficiency using a customized DEA model. Results indicate that post-2005 health system reforms had resulted in enhanced efficiency. Further Lebanon’s healthcare system shows resilience by effectively handling higher demand through additional resources and ongoing enhancements. Asandului et al.27 assess the efficiency of public healthcare systems across 30 European states utilizing Data Envelopment Analysis (DEA). Their findings reveal a mix of developed and developing countries positioned along the efficiency frontier, with a majority of the evaluated countries demonstrating inefficiency. El Husseiny28 estimated the healthcare system efficiency in the Arab region. They employed a two-stage Data Envelopment Analysis (DEA) method across 20 countries. Results show efficiency improvements ranging from 0.4 to 16%, with six countries continuously demonstrating efficiency. Djibouti and Sudan have demonstrated significant enhancements. Bahrain, Mauritania, Morocco, and Qatar consistently demonstrate efficiency. Further, Tobit regression shows that corruption and government health expenditure have negative effects on efficiency. These numerous research studies evaluated the efficiency of healthcare systems around the globe29,30,31,32,33,34.
AYDIN35 investigated the efficiency of healthcare services in OECD countries by employing the Malmquist Total Factor Productivity analysis. It deals with the difficulty of efficiently providing intricate healthcare services in the face of limited resources. Mitropoulos36 examines how the global economic crisis affected hospital productivity and quality in Greece between 2009 and 2013. The study uses an innovative analytical framework that includes a quality-adjusted meta-frontier Malmquist index to examine efficiency, innovation, and leadership improvements in primary, secondary, and tertiary care levels. The findings suggest that austerity policies have a detrimental impact on the quality and productivity of tertiary hospitals. Al-Hanawi and Makuta37 analyze the variations in total factor productivity (TFP) within Saudi Arabia’s healthcare sector between 2006 and 2018. Analysis reveals an annual reduction of 5.6% in Total Factor Productivity (TFP), mostly attributed to technical regression. Public hospitals declined at a rate of 6.0% per year, whereas private hospitals declined at a rate of 4.8% per year. Tackling technical obstacles is essential for enhancing productivity in healthcare services. Asghar et al.38 analyzed variations in cost productivity among 55 member states of the Organization of Islamic Cooperation (OIC) between 2011 and 2015. The results show a 7.9% rise in cost productivity, mostly due to enhancements in allocative efficiency and technical advancements. Key factors such as literacy rate and per capita GDP have a significant influence. However, the effect of population growth on the overall changes in the health production frontier is deemed minimal. Furthermore, a multitude of research studies have utilized the Malmquist productivity index to assess the total factor productivity change and its key determinants, namely technical efficiency change or technological change39,40,41,42,43.
Moreover, few studies employed the DEA and Malmquist productivity index to evaluate the efficiency and productivity change of the healthcare system of China44,45,46. Hu et al.47 examined the impact of the information society’s advancement on healthcare system efficiency in China, specifically focusing on variations among provinces. An analysis was conducted using a two-stage Data Envelopment Analysis (DEA) methodology and panel data from 31 provinces (2014–2017), revealing a minor decrease in healthcare efficiency despite a rise in the Information Society index. Emphasizing pure technical efficiency (PTE) is essential for enhancing total technical efficiency (TE). The influence of information society development differs between provinces with varying levels of efficiency. Total efficiency (TE) increases in low-efficiency provinces because of higher pure technical efficiency (PTE), whereas it decreases in high-efficiency provinces due to lower scale efficiency (SE). The study highlights the significance of investing in information infrastructure and utilizing emerging technology to improve healthcare efficiency, particularly in areas with inefficiencies. Yu and Tang48 present a DEA-Tobit regression model to assess the efficiency of the healthcare system in Chinese coastal provinces. The data from 11 provinces indicates that future changes should prioritize rational resource distribution to enhance the system’s scale and structure. Chai et al.49 evaluated the effects of China’s healthcare reform in 2009 on the functioning of the health system, specifically examining productivity and efficiency in 31 mainland provinces. The study examined the period from 2008 to 2015 and identified a decrease in efficiency and productivity after the reform, mostly due to changes in technology. Suggestions involve improving financial stability, maximizing resource distribution, and using affordable technologies in the health sector, as well as boosting urban planning and investing in education to improve the efficiency of health services. Although few studies tried to evaluate the efficiency and productivity change of provincial healthcare systems of China. But still the variation in efficiency evaluation over study period, regional technological heterogeneity and technological impact on the TFPC of the health care system of China is undiscovered and a comprehensive investigation. Hence, this study evaluates the efficiency, TGR, and MI in the healthcare systems of 31 Chinese provinces spanning the period from 1997 to 2022.
Methodology
DEA is a frequently employed mathematical approach for evaluating the efficiency of homogeneous Decision-Making Units50,51. The foundational DEA model, initially introduced by Charnes et al.52 operates under the assumption of constant returns to scale. Banker et al.53 refined the model to encompass variable returns to scale (VSR). Tone’s pioneering work54 introduced the concept of Slack-based Measure (SBM). Furthermore, Karou Tone55 Later, a method was devised to rank the most efficient DMUs. Sections “DEA-SBM model”, “DEA-meta frontier model”, and “DEA-Malmquist productivity index” described the development of DEA-SBM, meta-frontier analysis, and Malmquist productivity index models, respectively. Moreover, section “Kruskal–Wallis test” illustrates the importance and application of the Kruskal–Wallis test.
DEA-SBM model
The SBM represents a non-radial technique utilized to assess the efficiency of DMUs. Efficiency estimation entails the incorporation of slack, which denotes the variance between inputs and outputs at the production frontier. The methodology operates on the following principles:
Consider research with n Decision-Making Units (DMUs) referred to as “Provinces.” Each DMU is defined by m input indications and S output indicators. Let \({B}_{j}\) denote the \(j\)-th Decision Making Unit (DMU), where j varies from 1 to n. DMU \({B}_{j}\) has input indicators represented by \(\left[{x}_{ij}\right]\), for i from 1 to m, and output indications represented by \(\left[{y}_{rj}\right]\) for r from 1 to \(s\). The efficiency value of the \(j\)-th DMU is represented as \({h}_{j0}\). Let’s explain how the output-focused DEA-SBM model with varying returns to scale operates.
In academic discussions, the efficiency value at the \(j\)-th position is represented by the symbol \(\theta\), where \({\lambda }_{j}\) represents a nonnegative vector. An efficient Decision-Making Unit (DMU) operates optimally when \(\theta\) = 1. If \(\theta\) is not equal to 1, the DMU is deemed inefficient, indicating room for improvement.
DEA-meta frontier model
Using the Meta-frontier Model improves the precision of evaluating DMU efficiency among different groups. Efficiency assessments should be conducted within a group’s boundaries when all DMUs operate under the same technological conditions. The Technological Gap Ratio (TGR) statistic is a crucial instrument for quantifying the difference in technological progress between different groups56.
\(GEi\) denotes the efficiency relevant to DMUs classified within a particular group (regions in our study), whereas \(ME\) signifies the MF efficiency associated with DMUs across the entire population (country), including all groups (regions). The TGR quantitatively separates MF technology and frontier technology specific to a group of DMUs. A TGR value of unity indicates no technical disparity between the MF and the group frontier, rendering TGR a vital instrument for assessing regional disparities57. The meta frontier and group frontier efficiency are estimated through DEA-SBM.
DEA-Malmquist productivity index
Malmquist productivity indices serve as a valuable instrument for Decision-Making Units (DMUs) to monitor enhancements in efficiency across various periods. The effective utilization of this index hinges upon the assumption of a production function that aptly depicts the existing technical milieu. DEA models play a critical role in precisely determining the position of the threshold of this production function. The variation in production levels between periods t and t + 1 distinguishes a specific Decision-Making Unit (DMU), denoted as (\(DM{U}_{0}\))58.
where:
-
\({D}_{0}^{t}\left({x}_{0}^{t},{y}_{0}^{t}\right)\) presents the technical efficiency of \(DM{U}_{0}\) for period t,
-
\({D}_{0}^{t+1}\left({x}_{0}^{t+1},{y}_{0}^{t+1}\right)\) illustrate the technical efficiency of \(DM{U}_{0}\) for period t + 1.
-
\({D}_{0}^{t}\left({x}_{0}^{t+1},{y}_{0}^{t+1}\right)\) specifies the dynamic change in technical efficiency from time t to t + 1.
-
The technical efficiency of a specific \(DM{U}_{0}\) is represented as \({D}_{0}^{t+1}\left({x}_{0}^{t},{y}_{0}^{t}\right)\) . The efficiency is calculated by replacing the data from period t with the data from period t + 1.
-
Equation (5) shows the change in technical efficiency of \(DM{U}_{0}\) from period t to t + 1. The period indicated by the square brackets shows the technological advancements noticed in the same DMU. An index value greater than 1 shows that \(DM{U}_{0}\) achieved a higher output in the latter period than in the earlier era. Two possibilities can be suggested to account for this substantial rise in productivity. It is possible that \(DM{U}_{0}\) implemented sophisticated techniques, thus enhancing its effectiveness.1.
Kruskal–Wallis test
The Kruskal–Wallis test is a non-parametric technique utilized to evaluate distinctions among three or more separate groups. The method assesses the comparability of group medians by rating all values and examining for significant differences. It is beneficial when data does not adhere to the assumptions of parametric tests. Commonly utilized in social sciences, healthcare, and environmental investigations, it is efficient for comparing groups with data that does not follow a normal distribution59. The study focused on the existence of regional heterogeneity in efficiency, production technology, and total factor productivity in China’s health and care systems. However, differences in diverse regions for efficiency, TGR, and TFPC are statistically significant is a question of great concern for the validation of results. Therefore, to validate the heterogeneity existence, comparing average efficiency, TGR, and TFPC among four Chinese regions helps identify significant statistical disparities. The following 4 hypotheses are illustrated to quantify the regional differences in efficiency, TGR, and TFPC of the health and care systems in 4 different regions of China.
H01
The distribution of the healthcare system’s efficiency is the same across the Central, Eastern, Northeastern, and Western Chinese Regions.
H02
The distribution of MI in the healthcare system is the same across the Central, Eastern, Northeastern, and Western Chinese Regions.
H03
The distribution of TGR in the healthcare system is the same across the Central, Eastern, Northeastern, and Western Chinese Regions.
Inputs-outputs selection and data collection
Choosing the appropriate inputs and outputs for Data Envelopment Analysis (DEA) estimation is essential to guarantee result accuracy. Thoroughly analyzing these variables is crucial since they have a direct impact on the efficiency scores of Decision-Making Units (DMUs). Choosing the right inputs and outputs enables a thorough evaluation of the production process and ensures that important aspects influencing efficiency are included. Incorrect or unsuitable choices can result in biased output, misinterpretation of efficiency levels, and inefficient decision-making. Identifying the most pertinent inputs and outputs according to the aims and characteristics of the entities being evaluated is crucial for achieving dependable and significant DEA results. Based on previous studies on the topic, we employed the following inputs and outputs discussed in Table 1 to evaluate the efficiency and productivity change of the medical and health system of China60,61,62. For our analysis, we selected particular inputs and outputs to assess the efficiency and productivity of the healthcare sector. Regarding inputs, we examined the quantity of healthcare personnel, healthcare facilities, hospital beds, and government expenditure on healthcare. The quantity of medical personnel indicates the extent of human resources accessible for delivering healthcare. The quantity of medical institutions is indicative of the extent of infrastructure available for healthcare services. The quantity of medical beds signifies the ability to provide care for patients who require hospitalization. At the same time, government health expenditure represents the financial resources allocated to healthcare, which significantly impacts the total effectiveness and efficiency.
Regarding outputs, we took into variables the number of patients treated and the number of hospitalizations. The patient volume quantifies the extent of healthcare services rendered to individuals, indicating the number of persons who received medical care. The hospitalization count reflects the utilization of inpatient services, hence emphasizing the healthcare system’s capacity to address more severe medical conditions. These outputs provide valuable insights into the extent to which the healthcare system effectively addresses the demands of the public. The healthcare system of one province is considered a decision-making unit. The inputs-output data of 31 Chinese mainland provinces were collected from the China Statistical Yearbook and China Health Statistics Yearbook for the years 1997–2022.
Results and discussion
Sections “Efficiency of the healthcare system of china”, “Meta frontier, group frontier, and TGR in the healthcare system of China”, and “Total factor productivity of the healthcare system of China” present the results of efficiency, regional technological gap ratio, and total factor productivity change in the healthcare system across Chinese provinces for the study period 19,197-2022.
Efficiency of the healthcare system of china
Table 2 and Figure A1 present the efficiency of the healthcare system of China estimated through DEA-SBM for the study period of 1997–2022. It illustrates the efficiency trends across different periods and elaborates on the efficiency level of the healthcare system of China. In general, higher scores signify enhanced efficiency in the provision of healthcare services. Conversely, lower scores indicate deficiencies or opportunities for improvement. From 1997 to 2022, the mean efficiency score was 0.7672. It provides a comprehensive summary of the performance of the healthcare system over these years and identifies potential for improvement of 23.28. A consistent upward trajectory is observed in efficiency scores over time, signifying improvements in the efficiency of the healthcare system. The efficiency scores fluctuate from 1997 to 2009 but remain relatively constant within a certain range. Notable growth in efficiency is evident starting from 2010, as evidenced by consistently raised scores compared to preceding years. A marginal decrease in efficiency scores has been observed in recent years, specifically between 2020 and 2022; however, the overarching trajectory continues to be favorable. A moderate level of efficiency has been observed in the healthcare system throughout the entire period (1997–2022), as indicated by the average efficiency score of 0.7672. Significant enhancements in the provision of healthcare services have been indicated by the maximum efficiency scores observed in recent years, specifically from 2010 to 2016. The healthcare system experienced possible challenges or inefficiencies in management during the late 1990s and early 2000s, as evidenced by the lowest efficiency scores recorded during that period. The observed upward trajectory in efficiency scores implies that the Chinese healthcare system’s performance may have been influenced positively by reforms or interventions that have been implemented over time. The marginal decrease in efficiency scores observed between 2020 and 2022 may serve as an indication of emerging obstacles or domains necessitating focus to maintain or enhance the efficiency of the healthcare system63.
The healthcare reform in China had the objective of attaining Universal Health Coverage (UHC) by enhancing the accessibility, quality, and affordability of healthcare services for the public. The key initiatives were the expansion of insurance coverage, augmentation of government health expenditure, reformation of public hospitals, and the promotion of primary care. There was a notable rise in efficiency scores between 2009 and 2010, as depicted in Fig. A1, which can likely be ascribed to several reasons associated with these reforms. Firstly, the significant government investment in healthcare likely resulted in improved resource availability and more effective utilization. Increased insurance coverage facilitated greater accessibility to healthcare services, thereby mitigating the burden of out-of-pocket payments and financial obstacles for patients. Efforts aimed at improving the efficiency and standard of public hospitals have resulted in improved healthcare outcomes and more optimal utilization of resources. In addition, enhancing primary care services contributed to the efficient management of prevalent health conditions, alleviating the strain on tertiary institutions and enhancing the overall effectiveness of the healthcare system. The previous research studies discussed the benefits of these health measures in Chinese and global healthcare systems64,65,66.
A comprehensive analysis of the efficiency levels within healthcare systems across different provinces in China is presented in Table 3 and Fig. A2. Efficiency scores are assigned to each province as indications of the effectiveness and productivity of healthcare service delivery. The scores enable a comparative evaluation of healthcare system performance at a regional level. The observed variation in efficiency scores among the provinces underscores notable inequalities in the performance of healthcare systems. Significantly high efficiency scores are observed in provinces such as Guangdong, Zhejiang, and Shandong, suggesting that their healthcare systems are operating with effectiveness and efficiency. In contrast, it is seen that provinces such as Inner Mongolia, Tibet, and Hainan exhibit comparatively lower efficiency scores, indicating the presence of possible obstacles or inefficiencies within their healthcare systems. A comprehensive analysis of provinces exhibiting remarkably high-efficiency scores, namely Shanghai, Zhejiang, and Guangdong, provides significant insights into the underlying variables that contribute to their notable achievements. The greater performance of these provinces can be attributed to their well-structured healthcare infrastructure, effective healthcare management techniques, high-quality healthcare services, or a combination of these factors67.
On the other hand, provinces exhibiting lower efficiency scores may require additional scrutiny to ascertain potential areas for enhancement. Inadequate healthcare infrastructure, limited access to healthcare services, inefficiencies in healthcare delivery, and socioeconomic variables may be potential contributors to lower efficiency scores. Ensuring equitable access to quality healthcare services for all individuals across China demands the imperative task of addressing regional variations in healthcare system efficiency. Policymakers can employ the data presented to effectively allocate resources, direct investments, and execute focused initiatives to enhance the efficiency of healthcare systems in regions exhibiting lower ratings. By adopting this approach, individuals can strive towards attaining a more equitable and efficient provision of healthcare services on a national scale68.
Table 4 and Figs. A2 & A3 present a comprehensive analysis of the efficiency levels witnessed in the healthcare systems of four different regions in China, namely Central, Eastern, Northeastern, and Western. Every region consists of multiple provinces, and each province’s healthcare system is granted efficiency scores. The above-mentioned scores function as metrics that assess the efficiency and output of healthcare service provision in each respective geographical region. Commencing with the Eastern area, provinces such as Shanghai, Zhejiang, and Shandong exhibit conspicuously high-efficiency scores, signifying the presence of accurately structured and proficient healthcare systems. The Eastern area exhibits a commendable performance in healthcare delivery, as evidenced by its average efficiency score of 0.86917. In contrast, it is seen that provinces located in the Western and Northeastern areas tend to demonstrate comparatively lower efficiency scores, with average scores of 0.6983 and 0.7236, respectively. These regions’ healthcare systems may face issues or inefficiency.
The central provinces, namely Henan, Hubei, and Jiangsu, exhibit notable levels of efficiency, but marginally lower compared to the Eastern area. The Central provinces have an average efficiency score of 0.757, which suggests a moderate level of efficiency in delivering healthcare services. On the other hand, it is seen that provinces located in the Western and Northeastern regions exhibit comparatively lower levels of efficiency, as evidenced by their overall average ratings, in contrast to the Central and Eastern regions. This highlights the requirement for focused interventions and allocation of resources to tackle inefficiencies and enhance the performance of healthcare systems in these locations. In general, the variations in efficiency levels across different regions highlight the significance of customized approaches and cooperative endeavors in improving healthcare provision on a national scale. The policymakers can effectively allocate funding and execute focused interventions to enhance the efficiency of healthcare systems in various regions of China. China may strive to achieve a more equitable and effective healthcare delivery by addressing regional differences and exchanging best practices. This would ensure that all residents have equal access to high-quality healthcare services throughout the country69 (Fig. 2).

The average regional efficiency level of the healthcare system in China.
Meta frontier, group frontier, and TGR in the healthcare system of China
Table 5 provides a comprehensive overview of three key indicators, Meta Frontier (MF), Group Frontier (GF), and Technology Gap Ratio (TGR), within the healthcare system of China over the period from 1997 to 2022. MF is the same efficiency score presented in Table 2 and labelled the M&H efficiency. These measures offer valuable insights into the disparities in efficiency and technology among various regions of China’s healthcare sector. The Meta Frontier values are indicative of the efficiency benchmarks established by the National healthcare system, signifying the utmost level of efficiency attainable within the sector. On the other hand, the Group Frontier values represent the degrees of efficiency achieved by the collective healthcare system in one specific Chinese region. Although Meta Frontier values generally exceed Group Frontier values, both metrics exhibit a constant rising trajectory over time, suggesting broad enhancements in efficiency across the Chinese healthcare industry. The Technology Gap Ratio (TGR) is a significant metric used to assess the disparity in production technology among different regions in China. This statement clarifies the degree to which various regions exhibit disparities in technical progress within their healthcare systems. A smaller technology gap across regions is indicated by a lower Technology Gap Ratio (TGR), whereas a higher TGR signifies a greater discrepancy in manufacturing technology. By tracking TGR values over the study period, policymakers and stakeholders can pinpoint areas that may need extra assistance or financial resources to close the technological disparity and ensure fair and equal access to advanced healthcare services across the country. The TGR after 2010 enhanced dramatically showing a rapid growth in production technology in the healthcare systems of China. It indicates that technology gaps have been reduced during 2010–2022.
Table 6 provides a detailed analysis of the Meta Frontier (MF), Group Frontier (GF), and Technology Gap Ratio (TGR) scores in different areas and provinces of China’s healthcare system. The provinces are classified into four regions: Central, Eastern, Northeastern, and Western. These regions are accompanied by their corresponding scores for MF, GF, and TGR. The aforementioned scores offer significant insights into the levels of efficiency and digital inequities that exist across healthcare systems across various areas. There are noticeable differences in the scores among regions, indicating different levels of efficiency and technical progress. The Eastern provinces typically demonstrate higher MF and GF scores, suggesting the presence of more efficient healthcare systems in comparison to the Western and Northeastern provinces. It is noteworthy that certain provinces, particularly those in the Eastern region, have greater TGR scores, which suggests a narrower disparity between the Group Frontier and Meta Frontier scores. This implies that these provinces are in closer proximity to attaining the efficiency standards established by the most successful healthcare systems nationally.
The scores of the Technology Gap Ratio (TGR) provide insights into variations in production technology among different provinces. Greater Technology Gap Ratio (TGR) scores are indicative of narrower disparities in technology between the Group Frontier and Meta Frontier scores. This implies that specific provinces are in closer proximity to attaining the efficiency criteria established by the most successful healthcare systems nationally. This highlights the significance of implementing focused interventions to address existing inequities and provide fair and equal access to modern healthcare technologies. Examining specific provinces within each region uncovers different degrees of effectiveness and disparities in technology. Provinces that exhibit higher MF and GF scores typically demonstrate more efficient healthcare systems and narrower technology disparities. Conversely, provinces with lower scores may require strategic investments and policy initiatives to enhance their healthcare infrastructure and address any lingering technical inequalities. In addition, the computation of average values for each region offers a comprehensive perspective on the overall levels of efficiency and changes in the technology gap. Regions characterized by higher average MF and GF scores generally exhibit superior performance in the healthcare system as a whole and possess narrower technological gaps. This observation implies the presence of places that possess relative strength and possibility for enhancement.
Figure 3 indicates the TGR of all 4 regions. It indicates that the TGR of Eastern Chinese provinces is 0.9909, which is higher among all 4 regions. It illustrates that eastern China has the most advanced technologies employed in the health care system. Western regions witnessed a TGR value of 0.8109, ranked second in all four regions, and shows that after the eastern region, the western provinces keep more technologically advanced health care systems. Moreover, central (0.7942) and northeastern (0.7236) regions are ranked third and fourth, respectively. Elaborating on the TGR of different provinces study found that Beijing, Guangdong, Shanghai, Tianjin, and Zhejiang are the provinces with the latest healthcare technologies across all 31 mainland Chinese provinces for the study period. On the other hand, Heilongjiang (0.6878) and Jilin (0.5914) were found to have the least advanced healthcare technologies.

Technology gap ratio of healthcare systems in 4 different regions of China.
Ensuring fair access to sophisticated healthcare services nationally in China’s healthcare system requires the reduction of technological heterogeneity across various regions. Figure 3 presents the Technology Gap Ratio (TGR) values, which provide valuable information about the differences in production technology among the four regions: Eastern, Western, Central, and Northeastern. Based on the data provided, it can be observed that the Eastern region demonstrates the greatest TGR value of 0.9909 when compared to the other three regions. This observation suggests that the healthcare systems in the Eastern Chinese provinces are equipped with the most sophisticated technologies. To decrease the diversity of technology in this region, it is crucial to adopt methods that focus on spreading modern technologies to other regions and promoting cooperation and the exchange of knowledge across healthcare facilities.
Among the four regions, the Western regions exhibit a TGR value of 0.8109, placing them in second place. These findings indicate that the Western provinces have healthcare systems that are more technologically advanced compared to the central and northeastern regions. To address the existing technological gaps in Western regions, it is imperative to allocate resources toward infrastructure development, training initiatives, and research and development endeavors. These expenditures are crucial to ensuring that healthcare facilities are equipped with state-of-the-art technologies and can proficiently integrate them into patient care practices. Conversely, the Central and Northeastern regions exhibit lower TGR values of 0.7942 and 0.7236, respectively, suggesting that their healthcare systems utilize relatively least modern technologies. To tackle this issue, specific measures such as enhancing skills and knowledge, implementing technology transfer initiatives, and providing incentives for innovation can be employed to improve technological capabilities in these regions70,71.
In providing additional details regarding the TGR of various provinces, the research highlights Beijing, Guangdong, Shanghai, Tianjin, and Zhejiang as the provinces exhibiting the most advanced healthcare technology among all 31 provinces in mainland China throughout the study. In contrast, it has been observed that provinces such as Heilongjiang and Jilin exhibit the lowest levels of healthcare technology advancement, as indicated by their respective TGR values of 0.6878 and 0.5914. To mitigate technological inequities among provinces, it is imperative to prioritize the improvement of infrastructure, the cultivation of research and development activities, and the facilitation of collaboration between healthcare institutions and technology suppliers. The mitigation of technological disparities among various areas and provinces within China’s healthcare system demands a holistic strategy encompassing focused investments, knowledge dissemination, and capacity enhancement endeavors. China can reduce these technological gaps to provide fair and equal access to sophisticated healthcare services and enhance overall health outcomes for its population72.
Total factor productivity of the healthcare system of China
Table 7 presents a thorough examination of the Malmquist Index (MI), Efficiency Change (EC), and Technology Change (TC) in the healthcare system of China, covering the period from 1997 to 2022. The mean index (MI), which measures the overall change in productivity, exhibits an average value of 1.0033, indicating 0.33% growth in TFPC over the study period. The MI is further decomposed to efficiency change and technology change. This suggests a marginal growth in production within the system. The Efficiency Change (EC) exhibits an average value of 1.0123, indicating a 1.23 percent enhancement in the efficiency of the healthcare system. However, the average Technology Change (TC) is at 0.986, suggesting a decline of 1.4 percent in technical progress within the healthcare industry. These indicators provide a comprehensive understanding of the system’s performance. MI evaluates the combined effect of efficiency and technological changes, EC measures resource usage efficiency, and TC measures technological advancement. These results indicate that efficiency change is the main determinant of total factor productivity growth in the healthcare system of China. Policymakers and stakeholders can utilize these findings to identify areas that require improvement and develop specific initiatives to strengthen the efficiency and technical progress of China’s healthcare system73.
China must prioritize the enhancement of technology innovation within its healthcare industry to boost productivity growth. This objective can be accomplished by allocating resources towards research and development, cultivating an environment conducive to the advancement of medical technologies, encouraging the integration of digital health solutions, and enhancing the cooperation between healthcare providers and technology firms. China can achieve substantial enhancements in productivity and ultimately provide superior healthcare services to its population by prioritizing the advancement of technology. Policymakers and stakeholders can employ these data to identify areas in need of enhancement and devise targeted measures to boost the efficiency and technological advancement of China’s healthcare system74.
Table 8 and Fig. 4 display the mean values of the Malmquist Index (MI), Efficiency Change (EC), and Technology Change (TC) among the healthcare systems of 31 mainland provinces in China. The MI values across different provinces reveal a combination of positive and negative trends in productivity growth. Some provinces have seen improvement, while others have experienced slight losses. Efficiency Change (EC) and Technology Change (TC) provide valuable information about the effectiveness of resource usage and the progress of technology in each province. Results indicate that MI of Guizhou, Anhui, Yunnan, Jiangxi, Chongqing, Beijing, Guangxi, Ningxia, Qinghai, Fujian, Tibet, Gansu, Sichuan, Hainan, Shanghai, Inner Mongolia, and Tianjin witnessed growth as their corresponding score is greater than 1. On the other hand, the MI values of Henan, Guangdong, Hunan, Jiangsu, Zhejiang, Xinjiang, Shaanxi, Shandong, Hubei, Hebei, Shanxi, Jilin, Liaoning, and Heilongjiang are less than 1; indicating a decline in the productivity in these provinces over the study period. Results further elaborate that growth is mostly attributed to the EC as technology change values are less than 1. The study found that the EC of Shandong, Shanxi, Guangdong, Jilin, Liaoning, and Heilongjiang is less than one. These provinces need to enhance their efficiency in the healthcare system. All other provinces witnessed growth in EC. On the other hand, Guizhou, Anhui, Ningxia, Yunnan, Beijing, Tibet, Qinghai, Fujian, Chongqing, and Shanghai witnessed growth in TC. It shows that only these provinces enhance their technological growth in the healthcare system.

Variation in MI, EC, and TC of the healthcare system in Chinese provinces.
The growth in MI is influenced by Efficiency Change, while the majority of Technology Change values are below 1. It is crucial to improve the effectiveness of healthcare systems in different provinces. Provinces exhibiting EC scores below 1, such as Shandong, Shanxi, and other regions, should prioritize the enhancement of efficiency. In contrast, provinces such as Guizhou, Anhui, and others have had an increase in TC, which suggests the achievement of successful technical progress. To further augment MI, provinces should prioritize tactics that are customized to their requirements. In provinces characterized by suboptimal efficiency, the adoption of strategies such as process streamlining, resource allocation optimization, and the implementation of best practices might yield advantageous outcomes. Conversely, provinces that have lower technical progress might allocate resources towards research and development, encourage partnerships with technology companies, and facilitate the implementation of cutting-edge healthcare solutions. Provinces can effectively increase their MI and contribute to overall improvements in healthcare delivery and outcomes by carefully tackling both Efficiency Change and Technology Change75.
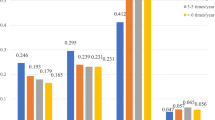
Table 9 and Figs. 5 and 6 depict the regional Malmquist Index (MI), Efficiency Change (EC), and Technology Change (TC) within the healthcare system of China. The 31 provinces are categorized into four regions: Central, Eastern, Northeastern, and Western. Every region consists of multiple provinces, and average values for MI, EC, and TC are derived within each region. In the Central region, provinces such as Anhui and Jiangxi demonstrate elevated MI values, which signify a comprehensive increase in production resulting from the combined influence of efficiency and technological progress. The Central region has an average MI of 1.0018, indicating a 0.18 percent marginal enhancement in productivity growth. The Efficiency Change (EC) in this region is significantly high, with an average value of 1.0198, which suggests efficient utilization of healthcare resources. However, the Technology Change (TC) exhibits a comparatively lower value of 0.9683, indicating the potential for enhancement in technological progress.

Total factor productivity change in the regional healthcare systems of China.

MI, EC, and TC of healthcare systems in 4 different regions of China.
The Eastern region exhibits a combination of outcomes, as provinces such as Beijing and Shanghai display higher MI values, indicating an increase in productivity influenced by both EC and TC. The mean MI value for the Eastern area is 0.9955, suggesting a consistent level of productivity. Although EC typically has a positive value of 1.007, TC has a significantly lower value of 0.9886, suggesting a requirement for more substantial technological progress. Provinces such as Jilin and Liaoning in the Northeastern area demonstrate lower MI values, suggesting a decrease in productivity. The Northeastern region has an average MI of 0.9137, indicating difficulties in achieving productivity growth. Both the EC and TC values exhibit relatively low levels, suggesting inefficiency in the utilization of resources and a lack of significant technological progress. Provinces such as Chongqing and Guizhou in the Western area exhibit higher MI values, suggesting a strong productivity increase influenced by both EC and TC. The mean MI for the Western area is 1.033, indicating substantial enhancements in production. Both the EC and TC values exhibit a notable raise, suggesting effective utilization of resources and substantial progress in technology.
To optimize MI in each region, provinces should prioritize the implementation of customized solutions. The Central and Eastern areas have the potential to enhance their resource utilization by prioritizing the advancement of technology. It is imperative for the Northeastern provinces to effectively tackle inefficiencies in resource consumption and allocate resources towards technical developments. In the meantime, it is recommended that Western provinces persist in utilizing their effective resource allocation and allocate more resources towards technological developments to maintain and augment productivity growth within their healthcare systems76.
To improve the Malmquist Index (MI) in the Central area, it is necessary to adopt a comprehensive strategy that combines technical advancements and efficiency enhancements in healthcare systems. First and foremost, it is imperative to cultivate partnerships among healthcare facilities, research centers, and technology businesses. This collaboration can expedite the advancement and acceptance of cutting-edge healthcare solutions customized to the specific requirements of the region. Moreover, allocating resources towards telemedicine services might enhance healthcare accessibility in remote regions, thereby optimizing the efficiency of healthcare provision. Additionally, the integration of data analytics and artificial intelligence technologies has the potential to enhance the allocation of resources, enhance patient outcomes, and reduce administrative procedures, so fostering overall productivity expansion. Promoting technological innovation and efficiency enhancement in healthcare systems is crucial for enhancing the MI in the Eastern area. The promotion of digital health technologies, such as electronic health records and telehealth platforms, is a crucial approach. These proposed solutions have the potential to not only enhance operational efficiency but also improve patient care and availability of services. The provision of incentives and resources to healthcare technology entrepreneurs has the potential to foster innovation within the region. In addition, it is imperative to allocate resources towards enhancing healthcare infrastructure to facilitate the integration of cutting-edge technologies and enhance the effectiveness of service provision.
The Northeastern region encounters distinct obstacles in augmenting Motivational Interviewing (MI) using technology progress and increasing efficiency in healthcare systems. It is essential to invest in information technology infrastructure, such as electronic health records and telemedicine capabilities, to modernize healthcare systems. Implementing training and educational initiatives for healthcare personnel to improve their proficiency in digital literacy and technology utilization can also facilitate advancement. Furthermore, promoting cooperation between healthcare providers and research institutions helps expedite the creation and application of cutting-edge technology specifically designed to meet the healthcare requirements of different regions. Expanding healthcare technology availability and promoting innovation are crucial methods for improving MI in the Western area. The facilitation of successful utilization of healthcare technology can be achieved by enhancing access to technology through infrastructure development and providing training for healthcare workers. The establishment of innovation hubs and technology incubators with a specific focus on healthcare has the potential to foster the creation of locally pertinent solutions. In addition, promoting collaborations between the public and private sectors can utilize resources and knowledge from both parties to promote technical progress in healthcare provision, ultimately leading to enhancements in overall efficiency as indicated by the Malmquist Index. Numerous research studies highlight the importance of technology advancement and efficiency enhancement to promote the healthcare system across the globe77,78.
Kruskal Wallis test
The results of sections “Efficiency of the healthcare system of china”, “Meta frontier, group frontier, and TGR in the healthcare system of China”, and “Total factor productivity of the healthcare system of China” reveal that the Efficiency, MI, and TGR of the healthcare system across the four distinct regions of China exhibit heterogeneity and are at different levels for different regions. Kruskal–Wallis test evaluates the statistically significant differences among the four regions of China concerning the average values of efficiency, MI, and TGR. The results of the Kruskal–Wallis test are illustrated in Table 10 and Figs. A4, A5 and A6. The significance level of all 3 hypotheses is less than 0.05. Therefore, we reject these hypotheses that state that the distribution of efficiency, MI, and TGR of the healthcare system is the same across the categories of 4 Chinese Regions. These results illustrate that efficiency, productivity growth, and production technology of healthcare systems of eastern, central, western, and northeastern China are heterogeneous.
The findings underscore prominent differences in the efficiency, rate of productivity growth, and utilization of production technology across the healthcare systems of eastern, central, western, and northeastern China. The observed diversity indicates that various regions within the country are encountering varying degrees of efficiency in how resources are utilized and technological improvements are embraced within their healthcare systems. To mitigate this heterogeneity and foster a more consistent advancement throughout various places, several techniques can be contemplated. The implementation of standardized practices and protocols across different regions has the potential to enhance operational efficiency and optimize resource allocation. Furthermore, it is imperative to allocate equal funding to healthcare infrastructure to guarantee that all regions have equitable access to essential resources and technology. To address the disparity, it is imperative to implement training and capacity-building initiatives targeting healthcare workers in regions characterized by poorer efficiency and technological advancement. The promotion of progress can be further enhanced through the facilitation of knowledge sharing and collaboration within regions, as well as the development of focused policy interventions that are customized to address the unique needs of each region. Through the implementation of these initiatives, policymakers and stakeholders can strive to decrease disparities and promote a fairer and more effective healthcare system in all regions of China. Research studies proved that the healthcare system of a country could be enhanced through resource utilization efficiency and technological advancement79,80.
Conclusion and policy implications
The implementation of efforts by the Chinese government aims to improve resource utilization efficiency and productivity within provincial healthcare systems, to mitigate inequities in technology adoption across different regions. It is crucial to prioritize the incorporation of digital technology and telemedicine platforms to enhance healthcare accessibility, especially in rural areas that lack sufficient services. Further, allocations towards infrastructure development and medical education serve to reduce healthcare disparities across different regions. However, the level of success in these efforts to improve efficiency, increase productivity growth, and reduce regional differences in technological adoption is still undiscovered and requires further examination. To fill this gap, this research used the DEA-SMB model to evaluate the efficiency of healthcare systems in 31 Chinese mainland provinces from 1997 to 2022, providing a clear understanding of the general trajectory of efficiency improvement. Additionally, Meta-frontier analysis is utilized to evaluate the technological gap ratio (TGR) across four distinct regions of China, thereby elucidating differences in the adoption of advanced technology. Furthermore, the Malmquist productivity index examines the overall change in total factor productivity (TFPC) throughout the study period. It scrutinizes the key drivers behind it, namely efficiency change or technological change, to offer insights for enhancing the healthcare system. The Kruskal–Wallis test is employed to assess the statistical significance of variations in efficiency, TGR, and TFPC across the four regions in China.
The findings reveal that the average efficiency score of China’s healthcare system is 0.7672, suggesting a moderate level of efficiency. China’s healthcare system has an efficiency score of 0.7672, which indicates a moderate level of efficiency when compared to the average across all provinces. While many provinces are achieving optimal performance with optimum efficiency scores of 1, others are experiencing lower levels of efficiency. The average score highlights the disparities in effectiveness around the country and indicates that there is potential for enhancement in specific regions. By prioritizing the enhancement of efficiency in the less efficient provinces, the total national healthcare system can experience substantial improvement. Throughout the study duration, there was a consistent and progressive rise in efficiency scores, signifying improvements in the overall efficiency of the healthcare system. Significant progress was notably observed starting from 2010, as efficiency scores continuously exceeded those of preceding years. Nevertheless, there was a slight decline in efficiency scores from 2020 to 2022, indicating the possibility of new issues or areas that need specific attention. Nevertheless, despite these oscillations, there have been notable improvements in healthcare service provision in recent years, particularly between 2010 and 2016, as seen by peak efficiency scores. In contrast, the late 1990s and early 2000s witnessed the presence of inefficiencies in healthcare management, as indicated by the lower efficiency scores observed during those years.
Provinces such as Guangdong, Zhejiang, and Shandong exhibit significantly higher efficiency scores, which serve as indicators of the effective functioning of their healthcare systems. In contrast, Inner Mongolia, Tibet, and Hainan demonstrate much lower efficiency scores, indicating the presence of inefficiencies. The investigation of provinces such as Shanghai, Zhejiang, and Guangdong that exhibit high efficiency demonstrates the presence of a well-organized healthcare infrastructure, efficient management strategies, and the provision of high-quality services, all of which contribute to their achievements. The healthcare performance in the Eastern region of China, encompassing Shanghai, Zhejiang, and Shandong, is significant, whereas the Western and Northeastern regions demonstrate comparatively lower levels of efficiency.
Technology Gap Ratio (TGR) is a metric used to evaluate the disparities in technology across different regions. After 2010, there was a significant improvement in TGR was witnessed, indicating a decrease in technology gaps. Eastern provinces generally demonstrate superior performance, indicating more effective healthcare systems. The analysis conducted by TGR reveals that the Eastern and Western areas exhibit the highest levels of technological progress, with Beijing, Guangdong, Shanghai, Tianjin, and Zhejiang emerging as prominent leaders. The Eastern region demonstrates the highest value (0.9909), suggesting the presence of highly sophisticated healthcare technologies. To address the issue of technology diversity, it is imperative to implement measures that facilitate the diffusion and collaboration of technology. The TGR of 0.8109 is observed in Western regions, whereas the Central and Northeastern regions demonstrate lower values of 0.7942 and 0.7236, respectively. These findings indicate that healthcare technology in these regions is comparatively less sophisticated.
During the study period, the MI indicates a slight increase of 0.33% in total factor productivity change (TFPC). Efficiency Change (EC) demonstrates a 1.23% enhancement, while Technology Change (TC) experiences a decline of 1.4%. These statistics underscore the significance of efficiency as the principal catalyst for the advancement of productivity growth within China’s healthcare system. Provinces such as Guizhou, Anhui, and Beijing witnessed an increase in MI while Henan and Guangdong experienced a decrease. Provinces like Shandong and Shanxi, with EC scores below 1, require efficiency improvements, while provinces like Guizhou and Anhui, which have TC growth, require a focus on technological advancement. The analysis of different regions indicates that there are varied trends in MI, with the Central region placing a strong emphasis on efficiency, while the Western region demonstrates excellence in both efficiency and technological advancements. On the other hand, the Northeastern region has obstacles in terms of productivity, requiring enhancements in the utilization of resources and advancements in technology. Kruskal–Wallis analysis reveals that healthcare systems in Eastern, Central, Western, and Northeastern China exhibit heterogeneity in terms of efficiency, productivity growth, and production technology.
Policymakers should prioritize investments in digital infrastructure due to the significant impact of digital technology and telemedicine platforms on improving healthcare accessible, particularly in rural areas. The aforementioned initiatives encompass the augmentation of broadband internet connectivity, the establishment of telecommunication infrastructure, and the promotion of the incorporation of digital health solutions within healthcare delivery systems. China has the potential to address the disparity in healthcare access between urban and rural areas and promote equal access to healthcare services in all regions by enhancing its digital infrastructure. Policymakers should commit resources towards medical education and training programs, specifically in underserved communities, to tackle gaps in healthcare quality and service delivery. China can expand the availability of trained medical workers in rural locations and improve the overall quality of healthcare services by allocating resources towards the recruitment and training of healthcare experts. Furthermore, the implementation of continuous professional development programs can effectively guarantee that healthcare professionals stay updated on the most recent breakthroughs in medical technology and optimal methodologies. The significance of strategic resource allocation is underscored by the identification of provinces with notably better efficiency scores, such as Guangdong, Zhejiang, and Shandong. It is recommended that policymakers give precedence to allocating resources towards regions characterized by lower efficiency scores, such as Inner Mongolia, Tibet, and Hainan, to effectively tackle prevailing inefficiencies and enhance the provision of healthcare services. This may entail the allocation of specific financial resources towards the enhancement of infrastructure, expansion of the healthcare workforce, and implementation of technology adoption programs within these regions.
China should give priority to developing technology innovation within the healthcare industry, based on the observed advances in technology adoption and productivity growth. This involves cultivating a setting that is favorable for the advancement of research and development, promoting cooperation between healthcare practitioners and technology companies, and providing incentives for the implementation of breakthrough healthcare solutions. Through strategic investments in state-of-the-art medical technologies and the cultivation of an innovative culture, China has the potential to establish itself as a prominent global frontrunner in healthcare innovation, therefore enhancing patient outcomes on a national scale. To acknowledge the variation in healthcare system performance among different locations, policymakers should enact customized measures to tackle challenges and opportunities that are distinct to each region. This may entail the formulation of healthcare development plans tailored to individual regions, the establishment of task groups dedicated to regional healthcare, and the promotion of collaboration among local governments, healthcare providers, and community partners. Through the implementation of a localized strategy to enhance the healthcare system, China may effectively cater to the distinct requirements and conditions of each region, thereby attaining a more equal healthcare outcome on a national scale. In conclusion, policymakers must give precedence to the ongoing monitoring and assessment of healthcare system performance to monitor advancements effectively, detect rising obstacles, and facilitate decision-making based on empirical data. This encompasses the routine review of efficiency measurements, productivity indicators, and technology adoption trends, and the implementation of periodic assessments to evaluate the effects of policy actions. China may enhance its healthcare system management by adopting a data-driven approach, enabling the country to promptly adjust its policies in response to changing healthcare demands and guarantee the ongoing enhancement of healthcare service provision across the nation. This study admits that numerous key constraints affect the complexity of the performance evaluation of China’s regional health systems. An important concern is the data availability on social health insurance, which is a vital component in assessing the effectiveness of healthcare. The specific data about the technology output in the health & care system is not available; therefore, it is a limitation of our study therefore could not be included in the production function of the efficiency and productivity estimation. Furthermore, the utilization of aggregated information may overlook substantial regional disparities and fluctuations in socioeconomic and institutional elements. In order to enhance future studies, it would be advantageous to incorporate more comprehensive data, including specific details regarding social health insurance and more precise area indicators. This would enhance the clarity and precision of the healthcare efficiency assessment. In addition, taking into account contextual elements such as regional healthcare policy and socioeconomic conditions would contribute to developing a more accurate comprehension of health system performance. By focusing on these specific areas, future research can provide a more comprehensive and precise evaluation of the efficiency of health systems, ultimately resulting in more informed policies and advancements in healthcare delivery.
Data availability
The data supporting the findings of this article is included within the article. Data for this study is freely available at the following links: China Statistical Yearbook: https://www.stats.gov.cn/sj/ndsj/, China Health Statistics Yearbook: https://data.cnki.net/yearBook?type=type&code=A.
References
Reibling, N., Ariaans, M. & Wendt, C. Worlds of healthcare: A healthcare system typology of OECD countries. Health Policy https://doi.org/10.1016/j.healthpol.2019.05.001 (2019).
Petre, I. et al. Analysis of the healthcare system in Romania: A brief review. Healthcare https://doi.org/10.3390/healthcare11142069 (2023).
Radević, I., Dimovski, V., Lojpur, A. & Colnar, S. Quality of healthcare services in focus: The role of knowledge transfer, hierarchical organizational structure and trust. Knowl. Manag. Res. Pract. https://doi.org/10.1080/14778238.2021.1932623 (2023).
Rojas, J. C., Rohweder, G., Guptill, J., Arora, V. M. & Umscheid, C. A. Predictive analytics programs at large healthcare systems in the USA: A national survey. J. Gen. Intern. Med. https://doi.org/10.1007/s11606-022-07517-1 (2022).
Young, Y., Alharthy, A. & Hosler, A. S. Transformation of Saudi Arabia’s health system and its impact on population health: What can the USA learn?. Saudi J. Health Syst. Res. https://doi.org/10.1159/000517488 (2021).
Ip, A. et al. Socioeconomic differences in help seeking for colorectal cancer symptoms during COVID-19: A UK-wide qualitative interview study of patient experiences in primary care. Br. J. Gen. Pract. https://doi.org/10.3399/BJGP.2021.0644 (2022).
IŞIK, M. A comparison study on healthcare systems for different countries during covid-19 crisis. New Era J. Interdiscip. Soc. Stud. https://doi.org/10.51296/newera.110 (2021).
Gurajala, S. Healthcare system in the Kingdom of Saudi Arabia: An expat doctor’s perspective. Cureus https://doi.org/10.7759/cureus.38806 (2023).
Saghafian, S., Song, L. D. & Raja, A. S. Towards a more efficient healthcare system: Opportunities and challenges caused by hospital closures amid the COVID-19 pandemic. Health Care Manag. Sci. https://doi.org/10.1007/s10729-022-09591-7 (2022).
Ngobeni, V., Breitenbach, M. C. & Aye, G. C. Technical efficiency of provincial public healthcare in South Africa. Cost Eff. Resour. Alloc. https://doi.org/10.1186/s12962-020-0199-y (2020).
Top, M., Konca, M. & Sapaz, B. Technical efficiency of healthcare systems in African countries: An application based on data envelopment analysis. Health Policy Technol. https://doi.org/10.1016/j.hlpt.2019.11.010 (2020).
Ibrahim, M. D., Daneshvar, S., Hocaoğlu, M. B. & Oluseye, O. W. G. An estimation of the efficiency and productivity of healthcare systems in sub-Saharan Africa: Health-centred millennium development goal-based evidence. Soc. Indic. Res. https://doi.org/10.1007/s11205-018-1969-1 (2019).
Singh, S., Kumar Sharma, S., Mehrotra, P., Bhatt, P. & Kaurav, M. Blockchain technology for efficient data management in healthcare system: Opportunity, challenges and future perspectives. Mater. Today Proc. https://doi.org/10.1016/j.matpr.2022.04.998 (2022).
Verma, R. Smart city healthcare cyber physical system: Characteristics. Technol. Chall. Wirel. Pers. Commun. https://doi.org/10.1007/s11277-021-08955-6 (2022).
Tian, S. et al. Smart healthcare: Making medical care more intelligent. J. Glob. Health https://doi.org/10.1016/j.glohj.2019.07.001 (2019).
Qiu, Y., Lu, W., Guo, J., Sun, C. & Liu, X. Examining the urban and rural healthcare progress in big cities of China: Analysis of monitoring data in dalian from 2008–2017. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph17041148 (2020).
Gao, L. et al. Effect of healthcare system reforms on public hospitals’ revenue structures: Evidence from Beijing, China. Soc. Sci. Med. https://doi.org/10.1016/j.socscimed.2021.114210 (2021).
Tao, W. et al. Towards universal health coverage: Lessons from 10 years of healthcare reform in China. BMJ Glob. Health https://doi.org/10.1136/bmjgh-2019-002086 (2020).
Ahmad, M. et al. Stylized heterogeneous dynamic links among healthcare expenditures, land urbanization, and CO2 emissions across economic development levels. Sci. Total Environ. https://doi.org/10.1016/j.scitotenv.2020.142228 (2021).
Zhang, H., Shi, L., Yang, J. & Sun, G. Efficiency and equity of bed utilization in China’s health institutions: Based on the rank-sum ratio method. Int. J. Equity Health https://doi.org/10.1186/s12939-023-01986-4 (2023).
Li, D. et al. The efficiency analysis and spatial implications of health information technology: A regional exploratory study in China. Health Inf. J. https://doi.org/10.1177/1460458219889794 (2020).
Chen, T. & Pan, J. The effect of spatial access to primary care on potentially avoidable hospitalizations of the elderly: Evidence from Chishui City, China. Soc. Indic. Res. https://doi.org/10.1007/s11205-020-02413-9 (2022).
Hung, J. Policy development on upskilling/reskilling older population care staff in China. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph19159440 (2022).
Gong, G., Chen, Y., Gao, H., Su, D. & Chang, J. Has the efficiency of China’s healthcare system improved after healthcare reform? A network data envelopment analysis and tobit regression approach. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph16234847 (2019).
Atmanti, H. D. & Naylah, M. The efficiency of healthcare system in Indonesia in 2014–2018. Hum. Soc. Sci. Rev. https://doi.org/10.18510/hssr.2019.7696 (2019).
Ibrahim, M. D. & Daneshvar, S. Efficiency analysis of healthcare system in Lebanon using modified data envelopment analysis. J. Healthcare Eng. https://doi.org/10.1155/2018/2060138 (2018).
Asandului, L., Roman, M. & Fatulescu, P. The efficiency of healthcare systems in Europe: A data envelopment analysis approach. Proc. Econ. Finance https://doi.org/10.1016/s2212-5671(14)00301-3 (2014).
El Husseiny, I. A. The efficiency of healthcare systems in the Arab countries: A two-stage data envelopment analysis approach. J. Hum. Appl. Soc. Sci. https://doi.org/10.1108/jhass-10-2021-0168 (2023).
Lee, D. H. Comparison of efficiency of healthcare systems of countries with global competitiveness using data envelopment analysis. Glob. Bus. Finance Rev. https://doi.org/10.17549/gbfr.2016.21.1.46 (2016).
Konca, M. & Top, M. What predicts the technical efficiency in healthcare systems of OECD countries? A two-stage DEA approach. Int. J. Healthc. Manag. https://doi.org/10.1080/20479700.2022.2077510 (2023).
Lo Storto, C. & Goncharuk, A. G. Efficiency vs effectiveness: A benchmarking study on European healthcare systems. Econ. Soc. https://doi.org/10.14254/2071-789X.2017/10-3/8 (2017).
Kozun-Cieslak, G. & Zdrazil, P. Efficiency of healthcare systems in the European Union States—Who performs better—Bismarckians or Beveridgeans?. Eur. Res. Stud. J. https://doi.org/10.35808/ersj/2725 (2021).
Breitenbach, M. C., Ngobeni, V. & Aye, G. C. Efficiency of healthcare systems in the first wave of covid-19-a technical efficiency analysis. Econ. Stud. 30(6), 3–21 (2021).
Knezevic, B., Lewandowski, R. A., Goncharuk, A. & Vajagic, M. Studying the impact of human resources on the efficiency of healthcare systems and person-centred care. Intell. Syst. Ref. Libr. https://doi.org/10.1007/978-3-030-79353-1_8 (2022).
Aydin, A. Benchmarking healthcare systems of OECD countries: A DEA—Based Malmquist productivity index approach. Alphanumeric J. https://doi.org/10.17093/alphanumeric.1057559 (2022).
Mitropoulos, P. A metafrontier Global Malmquist framework for hospitals productivity and quality measurement: Evidence from the Greek economic recession. EURO J. Decis. Proc. https://doi.org/10.1016/j.ejdp.2022.100018 (2022).
Al-Hanawi, M. K. & Makuta, I. F. Changes in productivity in healthcare services in the Kingdom of Saudi Arabia. Cost Eff0. Resour. Alloc. https://doi.org/10.1186/s12962-022-00338-3 (2022).
Asghar, N., Rehman, H. U. & Ali, M. Cost productivity of healthcare systems in OIC’s member countries: An application of cost Malmquist total productivity index. Rev. Econ. Dev. Stud. https://doi.org/10.26710/reads.v5i3.696 (2019).
Singh, S., Bala, M. M., Kumar, N. & Janor, H. Application of DEA-based Malmquist productivity index on health care system efficiency of ASEAN countries. Int. J. Health Plan. Manag. https://doi.org/10.1002/hpm.3169 (2021).
Yu, J., Liu, Z., Zhang, T., Hatab, A. A. & Lan, J. Measuring productivity of healthcare services under environmental constraints: Evidence from China. BMC Health Serv. Res. https://doi.org/10.1186/s12913-020-05496-9 (2020).
Cheng, Z. et al. Efficiency and productivity measurement of rural township hospitals in China: A bootstrapping data envelopment analysis. BMJ Open https://doi.org/10.1136/bmjopen-2016-011911 (2016).
Mancuso, P. & Valdmanis, V. G. Care appropriateness and health productivity evolution: A non-parametric analysis of the Italian regional health systems. Appl. Health Econ. Health Policy https://doi.org/10.1007/s40258-016-0257-y (2016).
Gearhart, R. The robustness of cross-country healthcare rankings among homogeneous OECD countries. J. Appl. Econ. https://doi.org/10.1016/S1514-0326(16)30005-8 (2016).
Lin, Z., Ba, F., Allore, H., Liu, G. G. & Chen, X. Geographic variation in inpatient care utilization, outcomes and costs for dementia patients aged 65 years or Older—China, 2017–2019. China CDC Weekly https://doi.org/10.46234/ccdcw2022.202 (2022).
Gu, T., Li, L. & Li, D. A two-stage spatial allocation model for elderly healthcare facilities in large-scale affordable housing communities: A case study in Nanjing City. Int. J. Equity Health https://doi.org/10.1186/s12939-018-0898-6 (2018).
Zhu, Y. et al. The hospital management practices in Chinese county hospitals and its association with quality of care, efficiency and finance. BMC Health Services Res. https://doi.org/10.1186/s12913-021-06472-7 (2021).
Hu, Y., Wang, Y., Lu, S. & Li, Y. Impact of the development of information society on healthcare efficiency: Empirical evidence from 31 Chinese provinces. Digital Health https://doi.org/10.1177/20552076231154375 (2023).
Yu, D. & Tang, W. Marine healthcare system: An analysis of economy and efficiency. J. Coast. Res. https://doi.org/10.2112/SI94-182.1 (2019).
Chai, P., Wan, Q. & Kinfu, Y. Efficiency and productivity of health systems in prevention and control of non-communicable diseases in China, 2008–2015. Eur. J. Health Econ. https://doi.org/10.1007/s10198-020-01251-3 (2021).
Zhu, N., Shah, W. U. H., Kamal, M. A. & Yasmeen, R. Efficiency and productivity analysis of Pakistan’s banking industry: A DEA approach. Int. J. Finance Econ. https://doi.org/10.1002/ijfe.2123 (2020).
Shah, W. U. H., Hao, G., Yan, H., Yasmeen, R. & Lu, Y. Energy efficiency evaluation, changing trends and determinants of energy productivity growth across South Asian countries: SBM-DEA and Malmquist approach. Environ. Sci. Pollut. Res. 19890–19906 https://doi.org/10.1007/s11356-022-23484-w (2022).
Charnes, A., Cooper, W. W. & Rhodes, E. Measuring the efficiency of decision making units. Eur. J. Oper. Res. https://doi.org/10.1016/0377-2217(78)90138-8 (1978).
Banker, R. D., Charnes, A. & Cooper, W. W. Some models for estimating technical and scale inefficiencies in data envelopment analysis. Manag. Sci. 30, 1078–1092 (1984).
Tone, K. Slacks-based measure of efficiency in data envelopment analysis. Eur. J. Oper. Res. https://doi.org/10.1016/S0377-2217(99)00407-5 (2001).
Tone, K. A slacks-based measure of super-efficiency in data envelopment analysis. Eur. J. Oper. Res. https://doi.org/10.1016/S0377-2217(01)00324-1 (2002).
Sun, J., Wang, Z. & Li, G. Measuring emission-reduction and energy-conservation efficiency of Chinese cities considering management and technology heterogeneity. J. Cleaner Prod. https://doi.org/10.1016/j.jclepro.2017.12.042 (2018).
Chiu, C. R., Lu, K. H., Tsang, S. S. & Chen, Y. F. Decomposition of meta-frontier inefficiency in the two-stage network directional distance function with quasi-fixed inputs. Int. Trans. Oper. Res. 20, 595–611 (2013).
Färe, R., Grosskopf, S., Lindgren, B. & Roos, P. Productivity changes in Swedish pharamacies 1980–1989: A non-parametric Malmquist approach. J. Prod. Anal. https://doi.org/10.1007/BF00158770 (1992).
Ostertagová, E., Ostertag, O. & Kováč, J. Methodology and application of the Kruskal–Wallis test. Appl. Mech. Mater. https://doi.org/10.4028/www.scientific.net/AMM.611.115 (2014).
Pourmahmoud, J. & Bagheri, N. Uncertain Malmquist productivity index: An application to evaluate healthcare systems during COVID-19 pandemic. Soc. Econ. Plan. Sci. https://doi.org/10.1016/j.seps.2023.101522 (2023).
Henriques, C. O. & Gouveia, M. C. Assessing the impact of COVID-19 on the efficiency of Portuguese state-owned enterprise hospitals. Soc. Econ. Plan. Sci. https://doi.org/10.1016/j.seps.2022.101387 (2022).
Mourad, N., Habib, A. M. & Tharwat, A. Appraising healthcare systems’ efficiency in facing covid-19 through data envelopment analysis. Decis. Sci. Lett. https://doi.org/10.5267/j.dsl.2021.2.007 (2021).
Lee, S. & Kim, C. Estimation of association between healthcare system efficiency and policy factors for public health. Appl. Sci. (Switz.) https://doi.org/10.3390/app8122674 (2018).
Zhang, Y., Zhao, G. & Gu, H. Investing in health capital: Does medical insurance matter?. Res. Int. Bus. Finance https://doi.org/10.1016/j.ribaf.2022.101661 (2022).
Jakovljevic, M. et al. Successes and challenges of China’s health care reform: A four-decade perspective spanning 1985–2023. Cost Eff. Resour. Alloc. https://doi.org/10.1186/s12962-023-00461-9 (2023).
Yip, W. et al. 10 years of health-care reform in China: Progress and gaps in Universal Health Coverage. The Lancet https://doi.org/10.1016/S0140-6736(19)32136-1 (2019).
Sousa, K. M., Pinhanez, M. D., Monte, P. A. & Diniz, J. A. Salary, financial autonomy and efficiency of healthcare systems in local governments. Appl. Econ. Lett. 27(2), 122–6 (2020).
Abolghasem, S., Toloo, M. & Amézquita, S. A dataset of healthcare systems for cross-efficiency evaluation in the presence of flexible measure. Data Brief https://doi.org/10.1016/j.dib.2019.104239 (2019).
Hodžić, S., Vuković, D. & Muharemović, A. the efficiency of healthcare system expenditures: Evidence from Croatia. Ekon. Vjesn. Rev. Contemp. Entrep. Bus. Econ. Issues 32(2), 361–71 (2019).
Harris, D. A. et al. Rapid telehealth-centered response to COVID-19 outbreaks in postacute and long-term care facilities. Telemed. e-Health https://doi.org/10.1089/tmj.2020.0236 (2021).
Silas, O. A. et al. Telepathology in Nigeria for global health collaboration. Ann. Glob. Health https://doi.org/10.5334/aogh.3673 (2022).
Rahman, M. A., Babaye, Y., Bhat, A., Collins, P. Y. & Kemp, C. G. Availability of two essential medicines for mental health in Bangladesh, the democratic republic of Congo, Haiti, Nepal, Malawi, Senegal, and Tanzania: Evidence from nationally representative samples of 7958 health facilities. J. Glob. Health https://doi.org/10.7189/jogh.12.04063 (2022).
Feng, Q. Q., Ao, Y. B., Chen, S. Z. & Martek, I. Evaluation of the allocation efficiency of medical and health resources in China’s rural three-tier healthcare system. Public Health https://doi.org/10.1016/j.puhe.2023.02.009 (2023).
Wu, J., Qiao, J., Nicholas, S., Liu, Y. & Maitland, E. The challenge of healthcare big data to China’s commercial health insurance industry: Evaluation and recommendations. BMC Health Serv. Res. https://doi.org/10.1186/s12913-022-08574-2 (2022).
Chen, Z. et al. Technical efficiency of regional public hospitals in china based on the three-stage dea. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph17249383 (2020).
Du, J., Cui, S. & Gao, H. Assessing productivity development of public hospitals: A case study of Shanghai, China. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph17186763 (2020).
Sefton, L. & Tierney, L. Pay-for-performance in the Massachusetts Medicaid delivery system transformation initiative. J. Healthc. Qual. https://doi.org/10.1097/JHQ.0000000000000357 (2023).
Akinola, S. & Telukdarie, A. Sustainable digital transformation in healthcare: Advancing a digital vascular health innovation solution. Sustain. (Switz.) https://doi.org/10.3390/su151310417 (2023).
Singh, T. et al. Systematic healthcare smart systems with the integration of the sensor using cloud computing techniques. In 2022 2nd International Conference on Advance Computing and Innovative Technologies in Engineering, ICACITE 2022 (2022). https://doi.org/10.1109/ICACITE53722.2022.9823626.
Serbezeanu, D. et al. Evaluation of poly(vinyl alcohol)–Xanthan gum hydrogels loaded with neomycin Sulfate as systems for drug delivery. Gels https://doi.org/10.3390/gels9080655 (2023).
Author information
Authors and Affiliations
Contributions
Conceptualization, Xiaowei Xu; methodology, Wasi Ul Hassan Shah, Xiaowei Xu, formal analysis, Xiaowei Xu; resources, Rizwana Yasmeen; data curation, Rizwana Yasmeen; writing—original draft preparation, Rizwana Yasmeen.; writing—review and editing, Wasi Ul Hassan Shah; visualization, Wasi Ul Hassan Shah.; supervision, Xiaowei Xu.;. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xu, X., Yasmeen, R. & Shah, W.U.H. Efficiency evaluation, regional technological heterogeneity and determinant of total factor productivity change in China’s healthcare system. Sci Rep 14, 19606 (2024). https://doi.org/10.1038/s41598-024-70736-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-70736-5
Keywords
This article is cited by
-
Evaluating the Impact of Transformation and Upgrading on the Green Efficiency of Industrial Water: Evidence from Sectoral Performance
Water Resources Management (2025)
