
Abstract
The prognostic value of central pathology review in upper urinary tract cancer (UTUC) remains inadequately addressed in existing literature. In this study, we conducted an extensive central pathology review and presented its influence on multi-center UTUC studies. We conducted a retrospective review of patients who underwent radical nephroureterectomy or segmental resection for UTUC to determine eligibility for central pathology review. In the Taiwan UTUC Collaboration cohort, 377 cases met the criteria for pathology review. We assessed agreement between pathologists using both the total percentage of agreement and simple kappa statistics. The prognostic implications of original and review pathology for various parameters were examined using the Cox regression model. This study included 209 female and 168 male participants. Pathology review revealed substantial interobserver variability in pT staging, with a particularly high rate of pT2 cases being upgraded to pT3 upon central review (17/70 pT2 stage made by local pathologists were finally confirmed as pT3 disease by the review pathologist). The local pathologist cohort identified fewer significant histological predictors in survival models compared to the review pathology cohort. Advanced pT stage, perineural invasion (PNI), and positive surgical margin were independent predictors of poorer overall survival and cancer-specific survival. PNI, lymphatic vascular invasion, and positive surgical margin were independent predictors of disease recurrence. Substantial interobserver variability in histological assessment underscores the importance of centralized pathology review for both multi-center studies and accurate post-operative management of UTUC patients. Advanced stage, perineural invasion, and margin status were significant histological predictors of oncological outcomes.
Similar content being viewed by others
Introduction
Histopathological analysis of radical nephroureterectomy (RNU) specimens is crucial for evaluating the prognosis of upper urinary tract urothelial cancer (UTUC). It helps determine the prognostic staging (RNU or kidney sparing surgery) and the need for adjuvant treatments after RNU, as per the NCCN guidelines. Consensuses have been reached to ensure accurate histopathological staging, including handling specimens, using reliable techniques, and standardized reporting. Unlike bladder urothelial cancer, UTUC requires careful examination and sampling due to the complexity of the upper urinary tract system. Technical factors and processing artifacts can lead to difficulties and bias in staging. Pathology review is recommended for consistent diagnosis and staging in multi-center cancer research, particularly for rare cancers1. Inter-observer variations have been observed in bladder urothelial cancer, with significant discrepancies in tumor grade and stage between local and central pathology2,3,4. However, there is limited discussion on reviewing UTUC histology, especially regarding variant histology, which is an adverse and often under-recognized feature5.
Chang and their colleagues reported that though significant interobserver variations were observed, central pathology review had minimal impact on clinical practice based on current UTUC treatment guidelines6. Whether pathology review for important histological factors, such as tumor grading, staging and surgical margin status, of UTUC will have an prognostic impact on multicenter study largely remained unknown. In addition, due to the rarity of UTUC, the histological review analysis for UTUC remained extremely scarce in the literature. Here, we reported the commonly reported the inter-observer variations in important histological factors in UTUC studies and their potential impacts on the multi-center UTUC research.
Material and methods
Patients
The Taiwan UTUC Collaboration Group conducted a registry database for UTUC. This multicenter internet-based registry enrolled UTUC cases from teaching hospitals in Taiwan since June 2018. The study received institutional review board approval of Taipei TzuChi Hospital (IRB no.: 08-X-037 & 12-X-004) and the requirement of informed consent was waived due to its anonymous nature without any identifiable information in the database. The study protocols and methods were carried out in accordance with relevant guidelines and regulations.
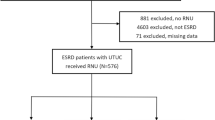
In our retrospective review of patients who underwent radical nephroureterectomy (RNU) or segmental resection for UTUC, a total of 756 cases were assessed. Among them, 377 cases met the eligibility criteria for specimen review. Cases without a definitive surgical treatment (RNU or segmental resection) or lacking accessible full sets of pathology slides were excluded from the pathology review. Eligible cases with a complete set of slides were sent for pathology review. The definition of a complete set of slides included all sections examined by the local institutional pathologist.
Histologic review
A single pathologist, recommended by the Taiwan Society of Pathology, conducted a histological review using an approved standardized format. The format was based on the AJCC TNM staging system and NCCN guidelines for urothelial cancer management. The central reviewer was unaware of the initial local pathologist's diagnosis, except for basic information such as specimen description and number of sections. The median number of slides reviewed was 9, with a range of 8 to 12. The histological diagnosis and staging of UTUC specimens followed the AJCC TNM staging system (version 9), and grading was based on the 2015 WHO/ISUP recommendation grading system. The diagnostic criteria for UTUC variants were described in the WHO classification of tumors.
Follow-up
The patients were scheduled for follow-up appointments every 3–6 months during the first year, and then every 6–12 months thereafter. To determine recurrence or progression-free status, chest radiography and cross-sectional imaging (such as computer-tomography [CT] or magnetic resonance imaging [MRI]) were utilized. Ureteroscopy, urine cytology and cystoscopy were employed to detect upper tract and intravesical recurrence. In this trial, UTUC recurrence was defined as the return of the tumor in the original site, regional lymph nodes, or distant metastasis. The primary objective of the study was to assess overall survival (OS), cancer specific survival (CSS), and disease-free survival (DFS), which is defined as the duration from surgical treatment until death from cancer-related causes for CSS and the duration from surgical treatment to the first occurrence of disease recurrence or death from any cause for DFS.
Statistical analysis
Demographic and clinicopathological differences between groups were compared using Pearson Chi-square for categorical variables. Agreement between original pathology and review pathology was measured by the total percentage of agreement and by simple kappa statistics. The Kaplan–Meier estimator was used to estimate the rates of prognostic outcomes. The prognostic impact of original and review pathology for the different parameters was analyzed by the Cox regression model with the estimation of hazard ratios (HR) and 95% confidence intervals. Cox proportional hazard model was selected to assess the effect of prognostic outcomes by stepwise regression analysis and after adjusting for potential confounders. The Pearson correlation coefficient measures the strength and direction of the linear association between two variables. The resulting coefficient value, ranges between -1 and 1, with values closer to -1 indicating a strong negative monotonic relationship, values closer to 1 indicating a strong positive monotonic relationship, and a value of 0 suggesting no monotonic relationship between the variables. Variance Inflation Factor (VIF) measure how much the variance of the estimated regression coefficient for a particular independent variable is increased due to multicollinearity. Multicollinearity occurs when independent variables in a regression model are highly correlated with each other, which can lead to unstable coefficient estimates and difficulty in interpreting the results. We addressed this challenge using following techniques: Firstly the principal component analysis (PCA) to explore variable relationships. Secondly, the regularization techniques (LASSO regression) to manage multicollinearity in the survival prediction model. Thirdly, the Akaike information criterion (AIC) technique to identify models. The performance differences between models were evaluated using the concordance index (C-index) and calibration curves. Statistical analyses were carried out with IBM SPSS statistical software version 26 and R version 4.4.1. The description of statistical methods was based on standard format of statistical analysis of Taiwan UTUC collaboration group7.
Declaration of generative AI and AI-assisted technologies in English editing
During the preparation of this work the authors used [GPT-3.5/ChatGPT] in order to improve readability and language of the work. After using this service, the author reviewed and edited the content as needed and takes full responsibility for the content of the publication.
Ethical consideration
The protocol for this research project has been approved by a suitably constituted Ethics Committee of the institution and it conforms to the provisions of the Declaration of Helsinki. Committee of Taipei Tzu Chi Hospital, Approval No. IRB no.: 08-X-037 & 12-X-004.
Results
Baseline characteristics
In this study, a final pathology review and analysis were conducted on 377 patients with UTUC, consisting of 209 women and 168 men. The median follow-up time was 13.22 months (interquartile range: 7.0–20.2). The majority of patients underwent either radical nephroureterectomy (RNU) (364 patients) or segmental resection (13 patients) as the accepted surgical treatments (Table 1). At the end of the follow-up period, 216 patients remained disease-free, while 51 patients experienced UTUC-related deaths.
A comparison between the histologic findings of local pathologists and the independent review pathologist revealed significant differences in various aspects. These differences included tumor grading, tumor architecture, invasiveness, variant histology, T stage, lymphovascular invasion (LVI), peri-neural invasion (PNI), and surgical margins (Table 2). The central pathologist identified a higher number of variant histology cases, as well as a greater presence of LVI, PNI, and positive surgical margins in the reviewed histology.
Level of agreement
The agreement rates and kappa values for various histology factors were examined and are presented in Table 3. Overall, tumor grading, peri-neural invasion (PNI), and surgical margin status demonstrated high levels of consistency, exceeding 80%. Conversely, the pT stage exhibited a low overall agreement rate, falling below 60%. The agreement rates for each pT stage were 42.9% for pTis, 92.7% for pTa, 15.1% for pT1, 34.3% for pT2, 75% for pT3, and 68.2% for pT4. The agreement for tumor grade (κ = 0.461), tumor architecture (κ = 0.524), pT stage (κ = 0.428), LVI (κ = 0.431), and surgical margin status (κ = 0.472) was deemed fair. On the other hand, the interobserver agreement for tumor invasiveness, PNI, and identification of variant histology were categorized as moderate.
Survival model
The univariate analysis of overall survival (OS) revealed that the review pathologist identified several significant histological predictors, including grading, tumor architecture, invasiveness, variant histology, pT stage, LVI, PNI, and surgical margin, more accurately compared to the local pathologists (Table 4). For cancer-specific survival (CSS) in the univariate analysis, all the histology variables examined by the review pathologists were significant predictors, while the local pathologists failed to recognize the tumor architecture and misinterpreted margin status and LVI as predictors for cancer-related death (Table 5). In the univariate analysis of disease-free survival (DFS), all the histology features examined by the review pathologist were found to be significant predictors (Table 6). However, the local pathologists failed to identify tumor architecture and variant histology as predictors for DFS.
Multicollinearity of histological variables in survival model
To address potential issues of overfitting and excessive redundant information in the cancer survival models, we initially assessed the homogeneity of variables through correlation analysis and variance inflation factor (VIF) (supp. Tables 1 & 2). In correlation analysis, the majority of histological features identified by the reviewing pathologist showed moderate to high correlation (16/21; 76%) with correlated other histological features, except for surgical margin status, which exhibited a consistently low correlation with other histological features (r = 0.197–0.358) (Supp. Table 1). In addition, correlation analysis revealed that the pT stage had high correlations with tumor architecture and invasiveness, and the LVI showed an unusual high correlation with the pT stage (r = 0.742). In VIF analysis, all the analyzed histological factors had moderate multicollinearity within the survival models. (Supp. Table 2) The pT stage exhibited the highest multicollinearity (VIF > 3) with other variables in the models but the margin status had the lowest VIF. To handle the possible multicollinearity, the PCA was employed to explore variable relationships (Fig. 1). PCA revealed strong correlations among histological variables except for pT stage and tumor architecture configuration. We compared survival models generated by LASSO and AIC with our feature-selected model that used only pT stage and margin status (Supp. Table 3). Both LASSO and AIC models significantly outperformed the feature selected model in terms of C-index (supp. Table 4) and calibration curve (Fig. 2). While the LASSO model included more histological variables (supp. Table 5) than the AIC model (Table 7) and achieved slightly better performance. The LASSO techinique also selected some statistically non-significant predictors (LVI in OS and CSS; UC variants in CSS; Invasiveness and pT stage in DFS). In addition, the LASSO model assigned extremely large or zero coefficients to some variables (e.g. pT stage and invasiveness in DFS), suggesting potential multicollinearity or overfitting. In contrast, the AIC model achieved comparable performance with the LASSO model but used a smaller set of statistically significant variables which were associated with lower Variance Inflation Factors (supp. Table 2). Therefore, for managing multicollinearity in our pathology survival model, we favor the AIC technique over LASSO (Table 7). The histology survival model revealed that advanced pT stage, PNI, and positive surgical margin were common independent predictors of worse OS and CSS. The LVI, PNI and positive surgical margin were independent predictors of disease recurrence.

Principal component analysis (PCA) was employed to explore variable relationships. PCA revealed strong correlations among most histological variables except for pT stage and tumor architecture configuration.

Calibration curve analysis for overall survival (OS), cancer specific survival (CSS), and disease free survival (DFS) in the original feature-selection model, LASSO regression model, and Akaike information criterion (AIC) generated model.
Discussion
Pathology review plays a crucial role in ensuring consistent diagnosis and accurate staging in multi-center cancer research, particularly for rare cancers1. A prior central pathology review in a retrospective UTUC cohort revealed significant interobserver variations in identifying variant histology of UTUC; however, their impact on treatment guidelines and clinical practice were minimal5. The present study constitutes the most extensive centrally pathology-reviewed cohort that thoroughly examined the correlations and their impact among commonly reported histological features, thus far. Our review identified substantial inter-observer variability in the assessment of outcome-predictive histological factors, including pT stage and surgical margin status. To improve consistency, we recommend a second evaluation of these factors by an experienced genitourinary pathologist. When consensus cannot be reached, centralized review is essential for multi-center studies. Notably, the Cox regression model derived from the centrally reviewed cohort demonstrated superior identification of clinically relevant histological features compared to the model based on local pathology assessments. Consequently, central pathology review significantly enhanced the accuracy and reliability of survival models in this multi-institutional UTUC study.
Due to the retrospective nature of this study, all patient treatments were completed prior to central pathology review, limiting the clinical implications of our findings to future patient management. However, if central review is carried out in a prospective nature, it would identify discrepancies in 14 of 377 cases initially diagnosed as pTa-1 disease. These cases would subsequently be reclassified as pT2-4 disease, necessitating adjuvant platinum-based chemotherapy or nivolumab per treatment guidelines. Additionally, 24 cases with positive surgical margins, undetected by initial local pathology, would be identified. These patients, also at increased risk for recurrence, required adjuvant chemotherapy to optimize outcomes. These findings underscore the potential for improved oncological outcomes through routine central pathology review in identifying under-staged advanced UTUC.
The comparison between the histologic findings of local pathologists and an independent review pathologist revealed significant differences in various important histological factors, such as tumor grading, tumor architecture, invasiveness, variant histology, pT stage, lymphovascular invasion (LVI), peri-neural invasion (PNI), and surgical margin status. In addition, the agreement rates of these outcome related histological factors were only moderate to fair consistency between the pathologists. Even for the most important treatment guiding histological factor, the pT stage, the overall agreement rate was only 55.4% with a kappa value of 0.428. Based on above findings, we propose that pT stage and surgical margin should undergo a second review by a genitourinary pathologist, and if consensus on pT staging cannot be reached, centralized review should be considered. Because the pT stage and the surgical margin status not only alter the following treatment strategy following nephroureterectomy, but also have significant impact on disease recurrence and long-term survival.
For multi-center trials, these inter-viewer differences clearly had significant impacts on all our survival prediction models (Tables 4, 5, 6). Therefore, an independent pathology review by an experienced pathologist or central pathology review is required to enhance the accuracy and consistency of multi-center UTUC studies. We recommend that the original full set pathology slide should be reviewed by an independent pathologist who is experienced in UTUC interpretation. In addition, those important survival prediction histological factors of UTUC, such as the pT stage, perineural invasion, and surgical margin status should be carefully addressed in histological review.
Given the observed moderate to high correlation among the reviewed histological features, it is essential to address the possibility of multicollinearity among the enrolled histological variables to prevent overfitting of the survival model. Given the high correlation and potential multicollinearity between most histological variables and pT stage, we selected pT stage, PNI, and surgical margin status as the most efficient predictors of OS and CSS. For DFS, PNI, LVI, and surgical margin were identified as the most efficient predictors. The present study's findings emphasize the importance of central pathology review, as it led to the identification of more significant histological features, ultimately enhancing the efficiency and accuracy of predicting UTUC outcomes. In addition, the pT stage continues to serve as the benchmark risk stratification tool for both survival outcome studies and treatment guidelines.
Based on the EAU Guidelines, various histological features have been identified as histological prognostic factors for UTUC, including stage, grade, LVI, tumor architecture, positive surgical margin, and variant histology8. Among these factors, LVI stands out as one of the most crucial independent risk factors. As a result, the International Collaboration on Cancer Reporting (ICCR) has recommended regular reporting of LVI in the pathological reports of all UTUC specimens9. While these histological factors have all been associated with oncological outcomes in UTUC, they may potentially exhibit similar patterns in a cancer survival model, leading to the problem of multicollinearity, which can greatly impact the accuracy and reliability of prognostic predictions. Remarkably, the collinearity of histological variables has not been thoroughly examined in prior reported multi-center UTUC studies up to this point. Additionally, a clear assessment of multicollinearity necessitates adherence to the same histological evaluation standards, underscoring the critical importance of independent central pathology review. Therefore, understanding the potential multicollinearity among histological factors in UTUC prognostic models is vital for ensuring reliable and meaningful predictions. While LVI remains a significant independent risk factor, its strong correlation and moderately high VIF level with the pT stage render it unsuitable for integration into survival models within UTUC prognostic prediction studies. Based on our findings, we can enhance the accuracy of prognostic predictions and advance our knowledge of UTUC outcomes.
Based on the agreement rates among various common histological features in UTUC, most features had moderate agreements between the local and central pathologists, except in diagnosis of variant histology. Pathology review for bladder UC exposed considerable inter-observer variations in reporting variant histology, with an agreement rate as low as 46% upon evaluation by an expert genitourinary pathologist10. In the current UTUC cohort, approximately 30% of cases displayed at least one variant subtype based on the review of pathological findings. This proportion aligns with observations from historical series. In Taiwan, genitourinary pathologists have adhered to a standardized regimen encompassing uniform training, specimen handling protocols, diagnostic criteria, standardized reporting templates, and peer review processes across diverse local institutions. Consequently, a noteworthy agreement rate of 77.2% (kappa value: 0.305) has been achieved among peers, indicating a level of agreement that, while not perfect, is still considered fair.
Despite these standardized practices, significant inter-observer discrepancies persist within multi-center studies. To effectively address these challenges, it is crucial to implement a pathology review mechanism, particularly focused on histological attributes that might be inadequately recognized, such as pT stage, surgical margin status, and variant histology. Moreover, a discernible pattern emerges, indicating that experienced consultant pathologists conducting review consultations demonstrate higher confidence and a greater inclination to identify and report variant histology when compared to their local counterparts.
In current study, those patients who underwent conservative endoscopic treatment were excluded from this study because definitive pathological staging is primarily based on imaging studies in this cohort. Additionally, the limited tissue obtained through ureteroscopy often provides insufficient histological information about the tumor base, making accurate pathological staging and comparison between pathologists challenging.
Limitations
The study has several limitations. Firstly, large scale central pathology review in a multi-center study still limited by insufficient manpower and relevant resources, which limit the sample size of current study. Secondly, while the study considers interobserver bias in pathology, it does not explore intra-observer reliability in reporting pathology. Thirdly, the absence of standardized templates for reporting specific variant histology, tumor architecture and PNI introduces bias in reported results. Fourthly, the review pathologist lacks complete access to original specimens; however, detailed descriptions, specimen sections, and pathology slides are provided. Additionally, the potential impact of limited manpower and resources would limit the generalizability of the study’s findings. Lastly, notable discrepancies between review and local pathology exist in adverse histologic findings. While not listed as factors for treatment changes in current guidelines, these discrepancies could affect patient outcomes. Thus, while pathology review in UTUC may have limited impact on clinical practice, it could influence multi-center trial outcomes.
In conclusion, central pathology review is indispensable for conducting robust multi-center cancer research, especially in rare malignancies such as upper tract urothelial carcinoma (UTUC). By enhancing diagnostic accuracy and consistency, central pathology review significantly improves the quality of multi-institutional UTUC studies. Prospective implementation of central pathology review holds the potential to translate these findings into improved patient outcomes. Addressing challenges such as inter-observer variability, multicollinearity, and standardized reporting will optimize the efficacy of pathology review in future UTUC trials.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Vujanić, G. M., Sandstedt, B., Kelsey, A. & Sebire, N. J. Central pathology review in multicenter trials and studies: Lessons from the nephroblastoma trials. Cancer 115(9), 1977–1983 (2009).
Van Der Meijden, A., Sylvester, R., Collette, L., Bono, A. & Ten Kate, F. The role and impact of pathology review on stage and grade assessment of stages Ta and T1 bladder tumors: A combined analysis of 5 European Organization for Research and Treatment of Cancer Trials. J. Urol. 164(5), 1533–1537 (2000).
Witjes, J. A., Moonen, P. M. & van der Heijden, A. G. Review pathology in a diagnostic bladder cancer trial: Effect of patient risk category. Urology 67(4), 751–755 (2006).
Gordetsky, J., Collingwood, R., Lai, W. S., Del Carmen Rodriquez Pena, M. & Rais-Bahrami, S. Second opinion expert pathology review in bladder cancer: Implications for patient care. Int. J. Surg. Pathol. 26(1), 12–17 (2018).
Shah, R. B., Montgomery, J. S., Montie, J. E. & Kunju, L. P. Variant (divergent) histologic differentiation in urothelial carcinoma is under-recognized in community practice: Impact of mandatory central pathology review at a large referral hospital. Urol. Oncol. 31(8), 1650–1655 (2013).
Chang, C. H. et al. Impact of pathology review in adverse histological characteristics and pT stages of upper tract urothelial cancer in a multicenter study. Front. Oncol. 11, 757359 (2021).
Lo, C. W. et al. Impact of adjuvant chemotherapy on variant histology of upper tract urothelial carcinoma: A propensity score-matched cohort analysis. Front. Oncol. 12, 843715 (2022).
Rouprêt, M. et al. European association of urology guidelines on upper urinary tract urothelial carcinoma: 2023 update. Eur. Urol. 84(1), 49–64 (2023).
Samaratunga, H. et al. Data set for the reporting of carcinoma of the renal pelvis and ureter-nephroureterectomy and ureterectomy specimens: Recommendations from the International Collaboration on Cancer Reporting (ICCR). Am. J. Surg. Pathol. 43(10), e1–e12 (2019).
Lee, M. C., Levin, H. S. & Jones, J. S. The role of pathology review of transurethral bladder tumor resection specimens in the modern era. J. Urol. 183(3), 921–927 (2010).
Acknowledgements
All members of the Taiwan Upper Tract Urothelial Carcinoma Collaboration Group.
Author information
Authors and Affiliations
Contributions
Conceptualization: YC Tsai*, Data curation: Hsiang Ying Lee, Wen-Jeng Wu, Ching-Chia Li, Chih-Hung Lin, Chung-Tai Yue, Yuan-Hong Jiang, Yu-Khun Lee Kuan Hsun Huan, Yao-Chou Tsai, Formal analysis: Yao-Chou Tsai*, Methodology: Yao-Chou Tsai*, Supervision: Wen-Jeng Wu, Writing—original draft: Yao Chou Tsai*, Writing—review and editing: Yung-Tai Chen, Yao-Chou Tsai*. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, YT., Lee, H.Y., Wu, WJ. et al. Central pathology review and its prognostic value in upper tract urothelial carcinoma patients: a nationwide multi-institutional study. Sci Rep 14, 19633 (2024). https://doi.org/10.1038/s41598-024-70785-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-70785-w
