
Abstract
Intracranial lesions in children often have good prognoses, allowing long-term survival. Cognitive functions, crucial for life quality, need more attention. Previous research has focused on adults, with pediatric studies limited by varied lesions and complex treatments. This study aims to evaluate cognitive and brain network changes in children with frontal lobe lesions, which significantly impact cognitive function, using a before-and-after comparison. The study enrolled 20 children with frontal lesions who underwent fMRI and cognitive tests before and after surgery, with only surgical treatment initially. Brain network changes were evaluated using functional metrics, and cognitive shifts were measured through test scores. Correlations were analyzed to explore brain mechanisms behind cognitive changes. Additionally, 20 healthy children underwent the same assessments for baseline data. Preliminary evidence of cognitive recovery, notably in social cognition, was observed about three months post-surgery, potentially linked to increased functional connectivity between the right lingual gyrus and right middle temporal gyrus. Children with frontal lobe lesions have demonstrated short-term postoperative cognitive improvement and associated reorganization and repair of brain networks, though this capacity for repair may diminish over time. This underscores the importance of timely rehabilitation interventions. This study offers unique insights into cognitive neuroscience and potential rehabilitation targets.
Similar content being viewed by others
Introduction
Intracranial space-occupying lesions (ISOLs), primarily tumors in the brain and central nervous system, are prevalent in children and constitute the most common solid tumors in this age group1. The frontal lobe, critical for cognitive tasks, emerges as the second most frequent site for ISOLs in pediatric cerebral convexity structures, surpassed only by the temporal lobe1. Contrary to earlier beliefs of its dormancy during childhood, the frontal lobe is now recognized for its vital contribution to children’s cognitive and developmental processes2. Most pediatric ISOLs are low to intermediate-grade or benign3, with surgical removal often sufficing for a positive long-term outcome and survival, negating the need for further therapy. The focus on cognitive outcomes, especially the impact of surgeries in crucial areas like the frontal lobe, is crucial for the long-term wellbeing of these children. Resting-state functional magnetic resonance imaging (rs-fMRI) offers a non-invasive method to explore brain activity and functional networks, providing insights into the cognitive changes and neural mechanisms involved4.
Research on post-neurosurgical brain network and cognitive changes has primarily targeted adults5,6,7. In children with ISOLs, studies have explored surgical and treatment impacts on brain networks and cognition. Seitzman et al.8 analyzed network differences between pediatric tumor survivors and normal children, while Semmel et al.9 observed changes in topological properties, like reduced small-worldness linked to working memory decline, in treated children. Papini et al.10 focused on long-term social cognition changes, and Zhang et al.11 investigated structural and cognitive changes in posterior fossa tumor survivors. These investigations, utilizing human data, enhance our understanding of brain functionality.
However, previous pediatric research has encountered unresolved issues, including patients with extensive lesion areas, various treatment approaches, and a lack of direct pre-and-post treatment comparisons within individuals. Many studies involved patients who received multiple treatments—such as surgery, radiotherapy, and chemotherapy—compared to healthy children, which made isolating the effects of each treatment modality challenging. Furthermore, few studies have focused on the effects on cognition after neurosurgery in children’s frontal lobes, which have a profound impact on higher cognitive functions. Our research addresses these challenges by focusing solely on patients with frontal lobe ISOLs (fISOLs) who have undergone only surgical treatment before their first follow-up. By utilizing a paired design, our study offers a more precise examination of the surgical impact while controlling for individual differences.
Our study examines cognitive and brain network changes in children with frontal lobe lesions, pre- and post-surgery, highlighting cognitive self-repair post-operation, notably in social cognition. The observed increased connectivity between the right lingual gyrus and middle temporal gyrus suggests a mechanism for this recovery. Our research offers unique insights into the control of indications for neurosurgical operations, cognitive neuroscience, and presents potential targets for rehabilitation therapy.
Method
Participants
Between November 2021 and January 2024, we enrolled 20 pediatric patients with fISOLs from Beijing Tiantan Hospital’s Pediatric Neurosurgery Department for our study, after excluding one due to significant head movement. These children, underwent both preoperative and postoperative MRI scans, but cognitive data was only available for 18 due to non-cooperation from two participants.
Inclusion criteria: willingness to participate, age range (6–18 years), diagnosis of primary fISOLs, and need for surgery. Exclusion criteria included: withdrawal from the study, non-cooperation in scans, existing medical conditions affecting the brain (such as hydrocephalus, traumatic brain injury, a history of brain surgery, mental or psychiatric disorders, genetic metabolic diseases, and endocrine disorders etc.), and contraindications to anesthesia.
The age range was chosen based on several considerations. The upper limit of 18 years aligns with our hospital’s practice of admitting patients 18 and under to the pediatric ward. The lower limit of six years is based on the typical age children enter primary school and acquire literacy skills essential for cognitive testing. Additionally, both our experience and the literature show that children six and older can effectively cooperate during MRI scans with minimal head movement, which is crucial for reliable data12.
All enrolled patients underwent craniotomy for lesion resection.
To enhance our analysis, we also included 20 healthy comparations, matched by age and gender from a separate cohort, who underwent identical MRI and cognitive tests, ensuring data integrity for comparison.
Ethical statements
Written informed consent was obtained from all enrolled children’s parents. This research was performed in line with the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Beijing Tiantan Hospital, Capital Medical University (KY 2021-100-02).
Cognitive assessment
Each participant’s neurocognitive abilities were evaluated using the CNS Vital Signs (CNS VS) battery13, designed for digital, repeat assessments and known for its validity and reliability. This 30-40-minute test measures 15 cognitive domains, providing age-standardized scores from 10 subtests. The 15 cognitive domains include Composite Memory (CM), Verbal Memory (VerbM), Visual Memory (VisM), Psychomotor Speed (PsyMotSpd), Reaction Time (RT), Complex Attention (ComAtt), Cognitive Flexibility (CogFlex), Processing Speed (ProcSpd), Executive Function (ExeFun), Social Acuity (SocAcu), Reasoning (Reason), Working Memory (WM), Sustained Attention (SustAtt), Simple Attention (SimAtt), and Motor Speed (MotSpd). Additionally, a Neurocognitive Index (NCI) is derived from CM, PsyMotSpd, RT, CogFlex, and ComAtt, indicating overall brain function. These evaluations were conducted before and after surgery, aligned with neuroimaging within the same week.
Imaging data acquisition
The participants were directed to maintain a seated position while keeping their eyes shut. Administration of sedatives was omitted throughout the examination process. All patients and healthy conparationsunderwent MRI scans on a 3T scanner (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) with a 64-channel head/neck coil. The protocol included T1 weighted structure imaging with magnetization prepared rapid acquisition gradient echo (MPRAGE) sequence and rs-fMRI with an echo-planar imaging (EPI) sequence. The scan parameters for the MPRAGE sequence were: repetition time (TR) = 1560 ms; echo time (TE) = 1.65 ms; flip angle = 8°; slices = 176; field of view (FOV) = 256 × 256 mm; and voxel size = 1 mm isotropic. The parameters for EPI with simultaneous multislice (SMS) acceleration technique were: TR = 2000 ms; TE = 35 msec; slices = 69; SMS = 3; FOV = 207 × 207 mm; voxel size = 2.2 mm isotropic; volumes = 240.
The imaging data for the patients enrolled in the study were obtained through scans conducted at Beijing Tiantan Hospital. The imaging data for the normal comparations were collected at Beijing RIMAG Medical Imaging Center. The MRI equipment used at both locations was of the identical model, and the scanning parameters employed were exactly the same.
Imaging data preprocessing
Data Processing and Analysis of Brain Imaging (DPABI v6.2,http://rfmri.org/dpabi) and Statistical Parametric Mapping (SPM 12, http://www.fli.ion.ucl.ac.uk/spm), implemented in MATLAB (Matlab Release 2020b, Mathworks Inc., Natick, MA), were used to preprocess rs-fMRI images14,15. The preprocessing steps were as follow:
(a) Discard the first 10 images; (b) Slice-timing correction and head motion correction. Exclude the subjects whose head movement translation is greater than 3 mm or rotation greater than 3 °. One patient was excluded due to excessive head movement during the MRI scan; (c) The linear trend, cerebrospinal fluid signal, white matter, and Friston 24-parameter head motion model were regressed as cumulative covariates from blood oxygen-level-dependent (BOLD) signal. Covariate regression of global signals was not used during preprocessing16,17; (d) Redirect the functional image to the standard space, Montreal Institute of Neurology space (MNI space), by DARTEL18, and then resample to 3 mm cube; (e) Band-pass filtering (0.01–0.10 Hz); (f) Smoothing the images with full width at half maximum 4 × 4 × 4.
The preoperative and postoperative data of the patient group and the data of the comparation group were preprocessed separately according to the above procedure.
Brain network analysis
Brain network analysis is classified into two main categories: functional segregation19, focusing on local brain functions, and functional integration19, examining connections between different brain areas. Key methods of functional segregation include Regional Homogeneity (ReHo)20, Amplitude of Low Frequency Fluctuations (ALFF)21, and Fractional ALFF (fALFF)22, which assess local brain activity, while functional integration methods like Seed-Based Analysis (SBA) analyze interregional brain connectivity.
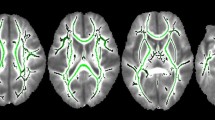
In our study, we had two experienced neurosurgeons delineate ISOL lesion boundaries and create individual masks for each patient. After preprocessing the imaging data, we converted the lesion masks to MNI standard space using individual deformation fields, and combined them into a composite mask (Fig. 1A). As shown in Fig. 1A, most lesions were in the frontal lobe, with some extending into the left postcentral gyrus and a small part of the right superior temporal gyrus. These extensions may be due to displacement from frontoparietal lesions or inaccuracies in mask delineation, considering potential errors from hand tremors or misjudgments of lesion boundaries.

Lesion mapping, ALFF and Reho. (A) The figure depicts lesion distribution, predominantly concentrated in the right frontal lobe, with some extending into the left postcentral gyrus and right temporal gyrus, likely due to lesions at the junction of brain regions and delineation errors. (B) ALFF reflects the local neural activity. Postoperatively, patients exhibited decreased neural activity in the right cuneus, bilateral middle occipital gyrus, and left insula compared to preoperative levels. (C) Reho is capable of reflecting the functional covariance between a voxel and its nearest neighbors, akin to highly localized functional connections. Postoperatively, patients exhibit a significant decrease in Reho within the left middle temporal gyrus and left calcarine.
After creating the lesion masks, we binarized the Automated Anatomical Labeling (AAL) atlas23 to produce a binary mask. This mask was then utilized to subtract both the lesion masks and the cerebellum, resulting in a mask designated for further analysis. Although this mask excluded some unaffected regions, such as the left postcentral gyrus and the right superior temporal gyrus, these exclusions were minor. Thus, all further statistical analyses were conducted using this refined mask.
In our study, we used the DPABI toolbox to calculate ReHo, ALFF, and fALFF for functional segregation. For functional integration, we applied SBA with the Power atlas24, excluding nodes in lesioned and cerebellar areas, leaving 187 nodes for analysis. Node and cluster localization was delineated using the AAL atlas23. Furthermore, we employed the “winner-takes-all” principle to align the AAL brain atlas with Yeo’s 7-network model25, detailing methodologies and region-network correspondences in Supplementary Materials 1 and 2 for scholarly reference.
Exploratory correlation analysis
We conducted Spearman rank correlation analyses between the changes in statistically significant cognitive test scores, the changes in statistically significant neuroimaging metrics (postoperative minus preoperative differences), and certain demographic information. Due to the availability of cognitive test data from only 18 pairs, all our correlation analyses were conducted within this subset of 18 patients. Detailed analyses will be elaborated upon in the subsequent Results section.
Statistical analysis and result display
In our study, we used paired designs to compare postoperative with preoperative data in patients. For rs-fMRI data, we applied paired T-tests with Gaussian random-field theory (GRF) correction (voxel p < 0.001, cluster p < 0.05, two-tailed) for ReHo, ALFF, fALFF, and SBA. Cognitive tests were analyzed using paired T-tests (p < 0.05, two-tailed) in SPSS. Spearman rank correlations were set at a 0.05 significance level (two-tailed), without multiple comparison corrections26.
Healthy comparations served as baselines for comparing preoperative patient data to understand postoperative changes. Imaging data comparisons between patients and comparations were done using two-sample t-tests with GRF correction. Continuous and dichotomous data were analyzed with independent t-tests and Chi-square tests, respectively, and ordinal data with Fisher’s exact test.
Results were visualized with BrainNet Viewer27, CAT12, and Graph Pad 8.
Results
Demographics of enrolled subjects
The study’s final group included 20 pediatric patients with complete imaging data before and after surgery, but only 18 completed cognitive tests both times. The patients’ average age was 10.3 years (ranging from 6.3 to 14.4 years), with equal gender distribution. Seizures were the most common initial symptom, and brain tumors accounted for half of the diagnoses, followed by vascular malformations (30%). The gross total resection rate was 90%, and the average lesion volume was 15.8 cm³, with a follow-up period of 15 weeks on average. Most patients had siblings, and most parents had completed high school, with fewer having higher or lower education levels. Mothers were typically the primary caregivers. Clinical and pathological details are in Table 1 and Supplementary Material 3, respectively. Comparisons with a healthy comparation group (detailed in Supplementary Material 4) revealed significant differences in parental education, which was adjusted as covariates for in subsequent analyses to reduce bias.
Cognitive assessment
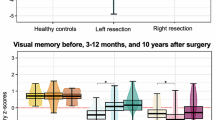
We noted a significant postoperative improvement in the SocAcu ___domain compared to preoperative levels within the patient group, whereas other cognitive domains did not exhibit significant changes (refer to Table 2). When comparing preoperative patient data to cognitive scores of healthy comparations, there were significant reductions in ComAtt, SocAcu, WM, SustA, and SimA domains in patients relative to typically developing children, with SocAcu showing the most marked decrease (refer to Supplementary Material 5).
In essence, compared to normal children, patients with fISOLs exhibited cognitive deficits in the aforementioned five domains, including SocAcu. However, only SocAcu demonstrated significant improvement post-surgery, with no notable changes in other domains. This suggests that SocAcu may possess a propensity for improvement.
Brain imaging analysis
The main goal of this study is to explore the overall impact of surgery and postoperative natural recovery on brain networks and cognitive functions. Healthy comparations are used mainly for baseline comparisons to aid in interpreting our results, which are primarily detailed in the supplementary materials when comparing preoperative data with healthy comparations.
ALFF, fALFF and Reho
Regarding functional segregation, post-surgery, only specific ALFF and ReHo clusters showed statistical significance after correcting for multiple comparisons (Table 3). Postoperative ALFF showed significant decreases in the right cuneus, bilateral middle occipital gyrus, and left insula (Fig. 1B), while ReHo decreases were notable in the left middle temporal gyrus and left calcarine (Fig. 1C). These changes, mainly in the visual, default mode, and ventral attention networks, indicate surgery and recovery might alter neural activity in these areas. Differences in functional segregation between patients and comparations, detailing widespread variations in brain regions, are detailed in Supplementary Material 6, showing both significant increases and decreases compared to healthy individuals.
SBA
Post-surgery, we noted extensive brain network changes, mainly in the default mode, limbic, frontoparietal, and visual networks, with generally reduced functional connectivity (FC) values, except for an increase in ROI 140 (see Table 4; Fig. 2). SBA comparisons between patients and comparations, detailed in Supplementary Material 7, revealed significant network alterations in patients, mostly as increased FC values compared to healthy children.

SBA. The SBA is capable of reflecting changes in brain networks. Among the 187 nodes examined in this study, we ultimately identified 16 nodes with significant alterations. The majority of nodes exhibited decreases in FC values between nodes and clusters postoperatively. Only ROI 140 showed an increase in values (Fig. 2G). ROI 140 belongs to the visual network, while the two clusters connected to it belong to the default mode network.
Exploratory correlation analysis
We conducted Spearman rank correlation analyses to assess the relationships between SocAcu changes and significant imaging metrics changes, as well as SocAcu changes and basic clinical characteristics (age, parental education, lesion volume, follow-up interval). We also examined correlations between imaging metrics changes and clinical characteristics mentioned above.
Our findings reveal a positive correlation between SocAcu changes and FC changes between ROI 140 and Temporal_Mid_R (Fig. 3A), and a negative correlation with FC changes between ROI 166 and Cuneus_L (Fig. 3B). Additionally, a positive correlation exists between SocAcu changes and lesion size (Fig. 3C). We also identified a negative correlation between the follow-up interval and various imaging metrics changes, and observed correlations between maternal education and FC changes (Fig. 4). For other correlation analyses that did not show significant results, please refer to Supplementary Material 8. All results of our correlation analyses have been included in Supplementary Material 8. We hope that these results will provide additional information to the readers, aiding in a more comprehensive understanding.

Results of Correlation Analysis between SocAcu Changes and Imaging Metrics and Basic Clinical Features. (A) The change in SocAcu positively correlates with the change in FC values between ROI 140 (Lingual_R) and Temporal_Mid_R. The violin plot in the lower right corner of Panel A suggests a tighter FC between ROI 140 (Lingual_R) and Temporal_Mid_R postoperatively. Considering the postoperative change in SocAcu, we can infer that the strengthening of FC between Lingual_R and Temporal_Mid_R is conducive to the increase in SocAcu. (B) The change in SocAcu is negatively correlated with the change in FC values between ROI 166 and Cuneus_L, with ROI 166 being located within Cuneus_L. The violin plot in the bottom right corner of Panel B suggests a certain degree of decoupling in FC between the two postoperatively. Considering the postoperative change in SocAcu, we can speculate that functional decoupling within Cuneus_L may be beneficial for the increase in SocAcu. (C) Panel C indicates that larger lesion volumes may be associated with greater changes in SocAcu.

Results of Correlation Analysis between Basic Clinical Characteristics and Imaging Metrics. (A)-(D) Panels A-D depict the correlation analysis results between the follow-up interval and the changes in ROI 140, ROI 106, ROI 153, and ROI 160, respectively. It can be observed that there is a negative correlation between the follow-up interval and imaging metrics. (E) Panel E illustrates the correlation between ROI 11 and the follow-up interval and maternal education level. The correlation with the follow-up interval remains negative, while it is positively correlated with maternal education level.
Discussion
This study indicates that social cognition might be the first cognitive ___domain to exhibit a short-term improvement trend following fISOLs surgery in children. We suggest that the right lingual gyrus and the right middle temporal gyrus (MTG) could be underlying or partly involved in this brain network mechanism, a finding seldom reported in previous research.
In our study on 20 children with fISOLs, 60% showed right-sided frontal lobe lesions, with most cognitive functions stable post-surgery, except for SocAcu which improved. This suggests potential short-term cognitive improvement after surgery, particularly in social cognition. Notably, changes in the brain network of supratentorial structures outside the lesion, impacts several networks with decreased activity and connectivity. Enhanced connectivity between the right lingual gyrus and bilateral middle temporal gyrus was linked to social cognition improvement, indicating a possible mechanism for post-surgical recovery in social cognitive functions in fISOL patients.
SocAcu scores come from an emotion perception test, assessing the ability to interpret and react to emotional signals by having subjects match facial expressions with corresponding words. In this study, the majority of cases involved right frontal lobe lesions, areas of which are inherently involved in emotion recognition28. The right hemisphere plays a significant role in emotion recognition as well29,30. This elucidates the preoperative presence of social cognitive impairments in these children.
Recent researches on facial expression recognition theory and neural networks are extensive. Studies have identified a distributed neural network involved in expression perception, including the fusiform facial area (FFA), occipitofacial area (OFA), superior temporal sulcus (STS), amygdala, and insula31,32,33, though their specific roles remain under debate. A meta-analysis by Liu et al.28 highlighted that frontal regions such as the inferior frontal gyrus (IFG) and middle frontal gyrus (MFG) contribute to the ventral stream and play significant roles in emotion processing. They also found that dynamic expressions elicit stronger activations in areas including the bilateral fusiform gyrus, MTG, left amygdala, left middle occipital gyrus (MOG), and right STS compared to static or neutral expressions. Zhen et al.34 proposed a hierarchical brain network for face recognition with 25 nodes across three sub-networks. Their findings positioned the STS within the middle temporal gyrus marked by AAL, anatomically proximate to the MTG activation area relevant to this study. The STS-containing network primarily facilitates expression recognition. Recent studies also identified anatomical connections between the fusiform gyrus and both the lingual and frontal lobes35, highlighting distinct areas responsibilities and interconnections.
Following brain injury in children, self-repair mechanisms are activated36. Signs of self-repair have been observed on social cognition, mainly expression recognition, in our study. The FC enhancement between the right lingual gyrus and right MTG was observed about an average of three months post-surgery for frontal lesions, whereas pre-surgery FC was comparable to that in normal children. Given the pivotal roles of both regions in expression perception, enhanced connectivity post-surgery may suggest a potential network mechanism for social cognitive recovery in children. However, some case reports indicate that congenital frontal lobe lesions37, frontal lobe trauma, or surgical damage38 can result in severe impairments in social cognition and affect the normal lives of affected children. This seems to contradict our findings. But we do not share this view. Firstly, the concept of “social cognition” in these case reports pertains to a different ___domain from the “emotion recognition” studied in our research. Secondly, the children in these cases had frontal lobe “damage” at a very young age, whereas our study involved patients with significantly older ages. The study by Taylor et al.39 supports the hypothesis that the younger children are when they sustain brain injury, the greater the adverse impact on their development. Additionally, research by On et al.40 indicates that there are no significant differences in emotion perception or recognition between children with brain injury and typically developing controls. In contrast, children and adolescents with traumatic brain injury perform significantly worse on theory of mind and language tasks compared to controls. These findings support both our results and those reported in previous case studies to some extent.
Facial expression recognition, crucial for social cognition and interactions41, was the sole cognitive ___domain to show recovery signs in this study. Linked to parent-child interactions42 and caregiver physical contact43, its recovery post-frontal lobe surgery may hinge on enhanced parental engagement. This improvement might also foster recovery in other cognitive areas44. Given its significance in nonhuman primate social interactions45, facial expression recognition appears as a fundamental, evolutionarily conserved cognitive skill, suggesting inherent self-repair mechanisms post-injury.
In this study, we identified numerous post-surgical brain network changes, most unrelated to facial expression recognition, with some correlated with the follow-up period. Only functional uncoupling in the cuneus was linked to improved facial expression recognition. These changes might represent typical post-surgical brain alterations46, potentially influencing social cognition or being irrelevant to it. The significance of these changes remains uncertain, necessitating further investigation. Maternal education may impact brain connectivity, though its importance was unclear. Additionally, a longer follow-up interval negatively correlated with FC changes in the right lingual gyrus and right MTG, implying limited self-repair capabilities and the potential need for post-surgical rehabilitation interventions. In the study conducted by Jacobs et al.47 on the executive functions of children with focal lesions, a nonlinear relationship was observed between the age of injury and outcomes. The sensitivity of the brain to damage and its capacity for recovery vary across different age groups. The authors suggested that injuries occurring between the ages of 7 to 9 tend to have relatively better outcomes. The mean age of the patients included in our study were over 10 years old, and our findings reveal that changes in FC in the right lingual gyrus and right MTG are associated with cognitive improvement. However, these changes in FC tend to decrease as the follow-up period extends. This observation suggests that even in the short term, the ability of cognitive self-repair diminishes gradually, underscoring the necessity of active rehabilitation interventions for postoperative children. Our findings may provide indirect support for the conclusions of Jacobs et al., and suggest that beyond a certain age window, the potential for cognitive improvement following injury is limited, with any such improvements likely occurring only in the early stages.
Xu et al.‘s48 research on cortical and subcortical plasticity in low-grade glioma patients revealed that larger tumor volumes correlate with higher gray matter density in compensatory brain regions. This phenomenon is attributed to the slow growth of low-grade gliomas, allowing time for the brain to adapt and reorganize, enhancing functionality48,49,50. The prevalence of low-grade tumors in our study participants likely accounts for the observed link between tumor volume and improvements in social cognition.
In neuropsychological research, patients with tumors or strokes are often studied due to their different disease mechanisms and resulting damage. Anderson et al.51 found that patients with tumors had less severe cognitive impairments compared to those with strokes. They suggested that tumors cause less direct damage to brain tissue than strokes do. Recent studies also indicate that the longer course of tumors allows for neuroplastic changes in the brain, which may lead to better cognitive outcomes52. Our study’s findings of improved cognitive abilities in postoperative children could be due to such preemptive compensations. Additionally, recent research suggests that inducing neuroplasticity before surgery may help reduce postoperative neurological deficits53,54.
Our study has certain constraints. The interpretation of the results of this study are limited by the sample size, extensiveness of the follow-up interval and study design. Although these factors may introduce confounding variables that complicate the interpretation of results, their presence make this study more reflective of real-world conditions, thereby enhancing the practical significance of the findings to some extent. The observed behavioral improvements and brain network changes in pediatric patients may be underpinned by more complex mechanisms. However, due to methodological limitations, our study is unable to delve deeper into these mechanisms. Further research is needed to explore these underlying processes comprehensively. From a research design perspective, this study only conducted a single follow-up, and it was a short-term follow-up after surgery. While our findings suggest the possibility of postoperative cognitive improvement, there remains the potential for an overly optimistic estimation of cognitive recovery following frontal lobe damage in children. As noted in the study by Jacobs et al.47, the full consequences of frontal lobe lesions in childhood may not become apparent until the child reaches adulthood. This is an important consideration for future research designs. Additionally, there are limitations inherent in the computerized cognitive testing battery we used. Firstly, the scope of the domains we could assess was constrained by the limitations of the testing battery itself. In this study, social cognition was evaluated through facial recognition tasks; however, social cognition encompasses a wide range of abilities, and due to the limitations of the testing battery, we were unable to gather data on other aspects of social cognition. Furthermore, the tests used in this study were not adaptive, which could lead to ceiling effects or floor effects, particularly when testing children of varying ages, whose abilities may not align with the fixed difficulty level of the tests. This potential source of bias is another important consideration for future research designs.
Conclusion
This study observed early signs of social cognition recovery around three months post-fISOL surgery, the first cognitive ___domain to show improvement. The right lingual gyrus and right MTG, external to the lesion, appear to facilitate social cognitive recovery in children through enhanced FC, which diminishes over time. This suggests that although there may be early improvements in cognitive abilities post-surgery, the injury could still disrupt the trajectory of cognitive development, thereby underscoring the importance of timely rehabilitation interventions. Although factors such as the sample size and the broad range of follow-up intervals may limit the interpretation and generalizability of our results, this study provides valuable insights based on real-world findings in the absence of prior knowledge. These insights offer potential targets for future rehabilitation research in this field and contribute to the understanding of neuroscience. Our findings provide valuable clues for subsequent research efforts.
Data availability
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request.
References
Ostrom, Q. T., Cioffi, G., Waite, K., Kruchko, C. & Barnholtz-Sloan, J. S. CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2014–2018. Neuro-oncology23, iii1–iii105. https://doi.org/10.1093/neuonc/noab200 (2021).
Anderson, V. & Spencer-Smith, M. in Principles of Frontal Lobe Function (eds Silvia A. Bunge, Arthur W. Toga, Donald T. Stuss, & Robert T. Knight) 0 (Oxford University Press, 2013).
Cohen, A. R. Brain tumors in children. N. Engl. J. Med.386, 1922–1931. https://doi.org/10.1056/NEJMra2116344 (2022).
Stam, C. J. Modern network science of neurological disorders. Nat. Rev. Neurosci.15, 683–695. https://doi.org/10.1038/nrn3801 (2014).
Busch, R. M. et al. Neuropsychological outcome following frontal lobectomy for pharmacoresistant epilepsy in adults. Neurology88, 692–700. https://doi.org/10.1212/WNL.0000000000003611 (2017).
Jutten, K. et al. Asymmetrictumor-relatedalterations ofnetwork-specificintrinsic functional connectivity in glioma patients. Hum. Brain. Mapp.41, 4549–4561. https://doi.org/10.1002/hbm.25140 (2020).
You, X. et al. fMRI prediction of naming change after adult temporal lobe epilepsy surgery: Activation matters. Epilepsia60, 527–538. https://doi.org/10.1111/epi.14656 (2019).
Seitzman, B. A. et al. Cognitive deficits and altered functional brain network organization in pediatric brain tumor patients. Brain Imaging Behav.https://doi.org/10.1007/s11682-023-00798-y (2023).
Semmel, E. S., Calhoun, V. D., Hillary, F., Morris, R. & King, T. Z. Graph analysis of resting state functional brain networks and associations with cognitive outcomes in survivors of pediatric brain tumor. Neuroimage: Rep.3. https://doi.org/10.1016/j.ynirp.2023.100178 (2023).
Papini, C. et al. Social cognition and adjustment in adult survivors of pediatric central nervous system tumors. Cancer. https://doi.org/10.1002/cncr.34889 (2023).
Zhang, Y. et al. Brain structural abnormalities in survivors of pediatric posterior fossa brain tumors: A voxel-based morphometry study using free-form deformation. Neuroimage42, 218–229. https://doi.org/10.1016/j.neuroimage.2008.04.181 (2008).
Byars, A. W. et al. Practical aspects of conducting large-scale functional magnetic resonance imaging studies in children. J. Child. Neurol.17, 885–890. https://doi.org/10.1177/08830738020170122201 (2002).
Gualtieri, C. & Johnson, L. Reliability and validity of a computerized neurocognitive test battery, CNS Vital Signs. Arch. Clin. Neuropsychol.21, 623–643. https://doi.org/10.1016/j.acn.2006.05.007 (2006).
Yan, C. G., Wang, X. D., Zuo, X. N. & Zang, Y. F. DPABI: Data processing & analysis for (resting-state) brain imaging. Neuroinformatics14, 339–351. https://doi.org/10.1007/s12021-016-9299-4 (2016).
Chao-Gan, Y. & Yu-Feng, Z. D. P. A. R. S. F. A MATLAB toolbox for pipeline data analysis of resting-state fMRI. Front. Syst. Neurosci.4, 13. https://doi.org/10.3389/fnsys.2010.00013 (2010).
Saad, Z. S. et al. Trouble at Rest: How correlation patterns and Group Differences Become Distorted after Global Signal Regression. Brain Connect.2, 25–32. https://doi.org/10.1089/brain.2012.0080 (2012).
He, H. & Liu, T. T. A geometric view of global signal confounds in resting-state functional MRI. Neuroimage59, 2339–2348. https://doi.org/10.1016/j.neuroimage.2011.09.018 (2012).
Ashburner, J. A fast diffeomorphic image registration algorithm. Neuroimage38, 95–113. https://doi.org/10.1016/j.neuroimage.2007.07.007 (2007).
Lv, H. et al. Resting-state functional MRI: Everything that nonexperts have always wanted to know. Am. J. Neuroradiol.39, 1390–1399. https://doi.org/10.3174/ajnr.A5527 (2018).
Zang, Y., Jiang, T., Lu, Y., He, Y. & Tian, L. Regional homogeneity approach to fMRI data analysis. Neuroimage22, 394–400. https://doi.org/10.1016/j.neuroimage.2003.12.030 (2004).
Zang, Y. F. et al. Altered baseline brain activity in children with ADHD revealed by resting-state functional MRI. Brain Dev.29, 83–91. https://doi.org/10.1016/j.braindev.2006.07.002 (2007).
Zou, Q. H. et al. An improved approach to detection of amplitude of low-frequency fluctuation (ALFF) for resting-state fMRI: Fractional ALFF. J. Neurosci. Methods172, 137–141. https://doi.org/10.1016/j.jneumeth.2008.04.012 (2008).
Tzourio-Mazoyer, N. et al. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage15, 273–289. https://doi.org/10.1006/nimg.2001.0978 (2002).
Power, J. D. et al. Functional network organization of the human brain. Neuron72, 665–678. https://doi.org/10.1016/j.neuron.2011.09.006 (2011).
Yeo, B. T. et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J. Neurophysiol.106, 1125–1165. https://doi.org/10.1152/jn.00338.2011 (2011).
Xu, M. et al. Modulations of static and dynamic functional connectivity among brain networks by electroacupuncture in post-stroke aphasia. Front. Neurol.13. https://doi.org/10.3389/fneur.2022.956931 (2022).
Xia, M., Wang, J. & He, Y. BrainNet Viewer: A network visualization tool for human brain connectomics. PLoS ONE8, e68910. https://doi.org/10.1371/journal.pone.0068910 (2013).
Liu, M., Liu, C. H., Zheng, S., Zhao, K. & Fu, X. Reexamining the neural network involved in perception of facial expression: A meta-analysis. Neurosci. Biobehav. Rev.131, 179–191. https://doi.org/10.1016/j.neubiorev.2021.09.024 (2021).
Abbott, J. D., Cumming, G., Fidler, F. & Lindell, A. K. The perception of positive and negative facial expressions in unilateral brain-damaged patients: A meta-analysis. Laterality18, 437–459. https://doi.org/10.1080/1357650X.2012.703206 (2013).
Adolphs, R., Jansari, A. & Tranel, D. Hemispheric perception of emotional valence from facial expressions. Neuropsychology15, 516–524 (2001).
Adolphs, R. & Spezio, M. in Progress in Brain Research Vol. 156 (eds S. Anders et al.) 363–378 (Elsevier, 2006).
Haxby, J. V., Hoffman, E. A. & Gobbini, M. I. Human neural systems for face recognition and social communication. Biol. Psychiatry51, 59–67. https://doi.org/10.1016/s0006-3223(01)01330-0 (2002).
Haxby, J. V., Hoffman, E. A. & Gobbini, M. I. The distributed human neural system for face perception. Trends Cogn. Sci.4, 223–233. https://doi.org/10.1016/s1364-6613(00)01482-0 (2000).
Zhen, Z., Fang, H. & Liu, J. The hierarchical brain network for face recognition. PLoS ONE8, e59886. https://doi.org/10.1371/journal.pone.0059886 (2013).
Palejwala, A. H. et al. Anatomy and white matter connections of the fusiform gyrus. Sci. Rep.10https://doi.org/10.1038/s41598-020-70410-6 (2020).
Fasotti, L. In Neuropsychological Rehabilitation 25–35 (Routledge, 2017).
Boes, A. D. et al. Behavioral effects of congenital ventromedial prefrontal cortex malformation. BMC Neurol.11, 151. https://doi.org/10.1186/1471-2377-11-151 (2011).
Anderson, S. W., Damasio, H., Tranel, D. & Damasio, A. R. Long-term sequelae of prefrontal cortex damage acquired in early childhood. Dev. Neuropsychol.18, 281–296. https://doi.org/10.1207/S1532694202Anderson (2000).
Taylor, H. G. & Alden, J. Age-related differences in outcomes following childhood brain insults: An introduction and overview. J. Int. Neuropsychol. Soc.3, 555–567. https://doi.org/10.1017/s1355617797005559 (1997).
On, Z. X., Ryan, N. P., Konjarski, M., Catroppa, C. & Stargatt, R. Social cognition in paediatric traumatic brain injury: A systematic review and meta-analysis. Neuropsychol. Rev.32, 127–148. https://doi.org/10.1007/s11065-021-09488-2 (2022).
Jessen, S. & Grossmann, T. The developmental origins of subliminal face processing. Neurosci. Biobehav. Rev.116, 454–460. https://doi.org/10.1016/j.neubiorev.2020.07.003 (2020).
Guajardo, N. R., Snyder, G. & Petersen, R. Relationships among parenting practices, parental stress, child behaviour, and children’s social-cognitive development. Infant Child. Dev.18, 37–60. https://doi.org/10.1002/icd.578 (2008).
Thrasher, C. & Grossmann, T. Children’s emotion perception in Context: The role of Caregiver Touch and Relationship Quality. Emot. (Washington D C)21. https://doi.org/10.1037/emo0000704 (2019).
Hagiya, K. et al. Facial expression perception correlates with verbal working memory function in schizophrenia. J. Neuropsychiatry Clin. Neurosci.69, 773–781. https://doi.org/10.1111/pcn.12329 (2015).
Schmidt, K. L. & Cohn, J. F. Human facial expressions as adaptations: Evolutionary questions in facial expression research. Am. J. Phys. Anthropol.33, 3–24. https://doi.org/10.1002/ajpa.2001 (2001).
Guan, X. Y. et al. Changes in a sensorimotor network, occipital network, and psychomotor speed within three months after focal surgical injury in pediatric patients with intracranial space-occupying lesions. BMC Pediatr.22, 321. https://doi.org/10.1186/s12887-022-03348-5 (2022).
Jacobs, R., Harvey, A. S. & Anderson, V. Executive function following focal frontal lobe lesions: Impact of timing of lesion on outcome. Cortex43, 792–805. https://doi.org/10.1016/s0010-9452(08)70507-0 (2007).
Xu, J. et al. Cortical and subcortical structural plasticity Associated with the glioma volumes in patients with cerebral gliomas revealed by Surface-Based Morphometry. Front. Neurol.8, 266. https://doi.org/10.3389/fneur.2017.00266 (2017).
Mandonnet, E. et al. Continuous growth of mean tumor diameter in a subset of grade II gliomas. Ann. Neurol.53, 524–528 (2003).
Cargnelutti, E., Ius, T., Skrap, M. & Tomasino, B. What do we know about pre- and postoperative plasticity in patients with glioma? A review of neuroimaging and intraoperative mapping studies. NeuroImage Clin.28, 102435. https://doi.org/10.1016/j.nicl.2020.102435 (2020).
Anderson, S. W., Damasio, H. & Tranel, D. Neuropsychological impairments associated with lesions caused by tumor or stroke. Arch. Neurol.47, 397–405. https://doi.org/10.1001/archneur.1990.00530040039017 (1990).
Desmurget, M., Bonnetblanc, F. & Duffau, H. Contrasting acute and slow-growing lesions: A new door to brain plasticity. Brain130, 898–914. https://doi.org/10.1093/brain/awl300 (2007).
Duffau, H., Denvil, D. & Capelle, L. Long term reshaping of language, sensory, and motor maps after glioma resection: A new parameter to integrate in the surgical strategy. J. Neurol. Neurosurg. Psychiatry. 72, 511–516. https://doi.org/10.1136/jnnp.72.4.511 (2002).
Sughrue, M. et al. Prehabilitation and rehabilitation using data-driven, parcel-guided transcranial magnetic stimulation treatment for brain tumor surgery: Proof of concept case report. Brain Netw. Modulation. 1https://doi.org/10.4103/2773-2398.340144 (2022).
Acknowledgements
My effusive thanks to Shihao He for help and support during my studies. I couldn’t have done the research without his guidance. Thanks to my mentor and his team for their trust and support.
Author information
Authors and Affiliations
Contributions
X.Y.G., B.H.H., W.J.Z. and J.G. designed this study. X.Y.G., B.H.H., H.N.Z., X.H., C.L.H., N.C., Z.L. collected data for this study. X.Y.G., B.H.H., W.J.Z., Z.H.Y. and X.L. performed the statistical analyses. X.Y.G. and W.J.Z. interpreted the results. X.Y.G. and B.H.H. drafted the manuscript work. W.J.Z. and J.G. revised it critically for important intellectual content. All authors approved of final version to be published and agreed to be accountable for the integrity and accuracy of all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics declarations
This study adhered to the ethical principles outlined in the Declaration of Helsinki and received approval from the Institutional Review Board of our hospital under protocol number KY 2021-100-02.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Guan, X., Hu, B., Zheng, W. et al. Short-term changes in brain networks and cognition in children with frontal lobe lesions treated solely with neurosurgical procedures. Sci Rep 14, 29930 (2024). https://doi.org/10.1038/s41598-024-73088-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-73088-2
