
Abstract
This cross-sectional survey aims to determine whether cotinine exposure would enhance the relationship between blood manganese (Mn) and non-alcoholic fatty liver disease (NAFLD) in children using the NHANES database. Restricted cubic spline (RCS) and logistic regression analyses were adopted to determine the potential relationship. Besides, we tested the robustness of the results by performing trend tests and subgroup analyses. The study finally enrolled 866 children aged 18 years and below. Blood Mn was linearly linked to NAFLD and the risk of NAFLD was increased with the blood Mn elevation (P < 0.05). There was a notable relationship between blood Mn and NAFLD in crude model 1, which was still significant upon adjustment of all the identified covariates (all P < 0.05). Under Mn exposure, the cotinine-exposed group had a higher risk of NAFLD than the cotinine-unexposed group. In conclusion, blood Mn level is an independent risk factor for pediatric NAFLD, and cotinine exposure can enhance this relationship to some degree. Therefore, reducing cotinine exposure may alleviate detrimental consequences related to exposure to heavy metals in children.
Similar content being viewed by others

Introduction
Pediatric non-alcoholic fatty liver disease (NAFLD) is the most frequent form of chronic liver disease, with a prevalence of 7.6%, while it increases to 34.2% in obese children1. Mtabolic associated fatty liver disease (MAFLD) and pediatric fatty liver disease (PeFLD) have been proposed to replace NAFLD in children, but are not yet internationally recognized, so NALFD is still used in this study. Diagnosis of NAFLD in children is based on biomarkers, liver imaging (such as liver ultrasound, and magnetic resonance), or liver biopsy2. NAFLD comprises various fatty liver diseases without excessive alcohol intake3. It is a multisystem disease that affects extrahepatic organs, and its long-term health effects can extend into adulthood and lead to significant morbidity and mortality4. Some studies have shown that children with NAFLD are at a higher risk of developing cardiovascular diseases and metabolic disorders, which subsequently impact their quality of life5,6. The increased risks of intrahepatic and extrahepatic adverse outcomes attributed to NAFLD result in huge economic and clinical burden to both individuals and society7. Approved medications are not available for NAFLD, while physical exercise and diet control are the major recommended interventions8. Therefore, identifying the risk factors, especially modifiable risk factors is important for carrying out targeted interventions to reduce the disease burden of pediatric NAFLD.
There are 35 commonly encountered exposure metals, of which 23 are classified as heavy metals9. Heavy metals are metallic elements with high atomic weight and high density, which have adverse effects on human health since they are non-biodegradable and deposited in the body10. Humans are exposed to heavy metals mainly through contaminated air and food, domestic effluents, agriculture, and industrial waste11. The endoplasmic reticulum stress, hypothalamic dopaminergic system, impaired adipogenesis, and adipocytokines secretion can be disrupted by heavy metals, and hence liver inflammation and steatosis occur12.
Smoking is also a common source of heavy metal exposure, affecting the levels of various heavy metals in the human body. Smokers have significantly higher levels of cadmium, chromium, and lead in their urine and serum compared to non-smokers13,14. Elżbieta Kulikowska-Karpińska et al. found that smoking significantly influences the level of copper in the urine15. Heavy metal exposure due to smoking is associated with several diseases, such as nasal and sinus issues16, as well as periodontitis17. In addition, smoking is the leading preventable risk factor for cirrhosis, hepatitis B and C, and hepatocellular carcinoma, while the role of smoking in NAFLD remains controversial18,19. Liu et al. showed a positive association between smoking and NAFLD, while no association was observed in the others20,21,22. In America, children are the primary victims of secondhand smoke exposure (SHS), which has severe negative impacts on their health. Research has shown that secondhand smoke can lead to dental caries in children23 and attention deficit hyperactivity disorder24. This serious problem has attracted the attention of the American Academy of Pediatrics and the American Medical Association, and urged pediatricians and medical professionals to assist parents in protecting their children from SHS25,26.
Nevertheless, little is known about the relationship between blood heavy metals and pediatric NAFLD, especially in the case of smoking exposure. Therefore, we first explored the relationship between NAFLD and blood heavy metals in children whose information was collected from the National Health and Nutrition Examination Survey (NHANES). Our study showed no significantly different distribution of blood lead, cadmium, mercury, and selenium in groups of NAFLD and control; however, the disease group exhibited higher blood manganese (Mn) levels. The inconsistent findings27,28,29 triggered us to further explore the association of Mn with NAFLD the previous research. Then, we continued to explore the relationship between the two under smoking exposure. Notably, self-reported smoking status might have bias and serum cotinine level is an indicator reflecting both direct and indirect smoking quantity30. Thus, we assessed the modification role of cotinine exposure in the association of Mn with pediatric NAFLD.
Materials and methods
Data source and study population
NHANES (https://www.cdc.gov/nchs/nhanes/index.htm) is a database to assess the health and nutritional status of children and adults in the United States performed by the National Center for Health Statistics (NCHS). The database includes information on demographics, examination, laboratory, dietary, and questionnaires from 1999 to 2018. The research received approval from the NCHS Research Ethics Review Board and participants signed informed consent forms.
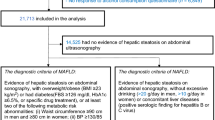
A total of 9254 samples from the 2017 to 2018 cycle were obtained. Exclusion criteria: age > 18 years since children are persons up to the age of 18 [United Nations Youth. [(accessed on 1 January 2020)];2020 Available online: https://www.un.org/en/sections/issues-depth/youth-0/index.html]; ever having over 4/5 or more drinks every day; serologic positivity for viral hepatitis; missing data of cotinine levels; missing information on heavy metals. Therefore, 866 remaining participants were enrolled in the study: non-NAFLD group (n = 685) and NAFLD group (n = 181). Figure 1 shows the screening process of the study population.

Flow charts of the inclusion and exclusion of participants.
Diagnosis of pediatric NAFLD
Based on previous research31, NAFLD in children can be diagnosed by waist circumference, body mass index, or fasting plasma glucose level > 100 mg/dL. In lean children, the presence of at least following two metabolic risk disturbances is also defined as NAFLD: high-density lipoprotein cholesterol (HDL-C) < 40 mg/dL, triglycerides ≥ 150 mg/dL, C-reactive protein level > 2 mg/L, HOMA-IR ≥ 2.5, diastolic blood pressure ≥ 85 or systolic blood pressure ≥ 130 mmHg.
Blood heavy metal measurements
The concentrations of blood lead, cadmium, mercury total, selenium, and Mn were determined by inductively coupled plasma mass spectrometry. All QC procedures recommended by the manufacturers were followed32. Limits of detection for blood lead, cadmium, mercury total, selenium, and Mn were 0.07, 0.1, 0.28, 24.48, and 0.99, respectively.
Serum cotinine levels
Serum cotinine is measured by an isotope dilution, high-performance liquid chromatography, and tandem mass spectrometry method (https://wwwn.cdc.gov/Nchs/Nhanes/2017-2018/COT_J.htm). The limit of detection of serum cotinine is 0.015.
Covariates
Based on the previous research and our interest, information on gender, race, age, education, poverty income ratio (PIR), waist circumference, total bilirubin, anion gap (AG), albumin, alanine transaminase (ALT), aspartate aminotransferase (AST), blood urea nitrogen (BUN), creatinine, and HDL-C, and triglycerides were collected. Gender (male and female), race (Hispanic, non-Hispanic White, non-Hispanic Black, and other races), age (≤ 18 years), education level (less than 9th grade and over 9th grade), and PIR were collected from the “Demographic variables and sample weights” file. Waist circumference data were acquired from the “Body measures” file in the “Examination data”. We retrieved data on total bilirubin, AG, albumin, ALT, AST, BUN, creatinine, HDL-C, and triglycerides from the “Laboratory data”. Detailed information is accessible from the official website (https://www.cdc.gov/nchs/nhanes/index.htm).
Statistical analysis
Baseline characteristics of the study population in the non-NAFLD and NAFLD groups were compared using the Chi-square test and Mann-Whitney U test for the categorical and continuous variables, respectively. The categorical data were expressed as counts (percentages), and the continuous data were represented as median [interquartile range] due to the skewed distribution. To avoid potential bias due to a confounding effect, we performed an analysis of collinearity in which the variance inflation factors (VIF) were below 3. Next, restricted cubic spline (RCS) combined with logistic regression models were employed for the exploration of the relationship between blood heavy metal levels as a continuous variable and NAFLD. Mode l was the crude model. Model 2 was adjusted for the demographic characteristics and body measures including age, race, PIR, and waist circumference. Model 3 was additionally corrected for the total bilirubin, AG, albumin, ALT, AST, HDL-C, and triglycerides except for the variables in Model 2. For sensitivity analysis, the heavy metal level was coded into three groups by tertiles to assess its association with NAFLD. Besides, the P for trend test was conducted to observe the trend of NAFLD risk across increasing blood heavy metal levels.
Then, an RCS analysis stratified by cotinine exposure was evaluated to investigate the modification of cotinine exposure in the relationship between blood heavy metals and NAFLD. The same three models were also adopted to analyze the association of heavy metals both as a continuous and categorical variable with NAFLD in two cotinine groups (unexposed and exposed groups). Finally, the relationship between the heavy metal and NAFLD was evaluated in different subgroups. P < 0.05 indicated statistical significance.
Results
Baseline characteristics
The characteristics of the participants are demonstrated in Table 1. The characteristics of the study population across three blood Mn groups are shown in Table S1. Older age, lower PIR, and higher waist circumference were observed in the NAFLD group with statistical significance (all P < 0.05). Total bilirubin, albumin, and HDL-C were decreased, while AG, ALT, AST, and triglycerides were increased in the NAFLD compared to those in the non-NAFLD (all P < 0.05). Particiapnts with NAFLD are more likely to be Hispanics. There was no remarkable difference in gender, education, cotinine concentration, BUN, and creatinine between the two groups. Moreover, except for blood Mn with a significant elevation in the NAFLD groups (P < 0.05), the other four blood heavy metals including blood lead, cadmium, mercury total, and selenium were not differentially distributed in the two groups (P > 0.05). Therefore, we focused on the association of blood Mn with NAFLD. There was no collinearity since the VIFs of all the significant variables were less than 3 (Table 2).
The association of blood mn level and NAFLD
First, RCS analysis showed a linear relationship between blood Mn level and NAFLD both in the crude model (P for nonlinear = 0.078) and adjusted model (P for nonlinear = 0.677) (Fig. 2A and B). The blood Mn level as a continuous variable was significantly related to NAFLD in three different models (P < 0.05) (Table 3). The models were adjusted in an additive way, starting from no covariate-adjusted model 1, adding for age, race, PIR, and waist circumference (model 2), total bilirubin, AG, albumin, ALT, AST, triglycerides, and HDL-C (model 3). In model 1, participants with higher blood Mn levels were 1.035 times more likely to be NAFLD [95% CI: 1.001–1.069]. Age, race, PIR, and waist circumference led to an increase in the odds ratio (OR) of NAFLD (OR [95% CI]: 1.051 [1.003, 1.101]). Laboratory variables enrolled in model 3 further increased the odds of NAFLD (OR [95% CI]: 1.071 [1.004, 1.142]). A similar trend was observed when blood Mn was taken as a categorical variable (P < 0.05). The positive relationship between blood Mn level and NAFLD was further confirmed by the trend test (P for trend < 0.05).

Restricted cubic spline analysis of the association of blood manganese level and nonalcoholic fatty liver disease. (A) A crude model with no covariate-adjusted. (B) An adjusted model with race, age, poverty income ratio, waist circumference, total bilirubin, anion gap, albumin, alanine transaminase, aspartate aminotransferase, high-density lipoprotein cholesterol, and triglycerides adjusted.
Cotinine exposure enhanced the association of blood mn level with NAFLD
Although we didn’t find a connection between cotinine concentration and NAFLD (Table 1), there was an obvious association of blood Mn level with NAFLD in different cotinine groups through an RCS model (Fig. 3). Blood Mn level had a positive relation with NAFLD and this relationship strengthened with the exposure of cotinine.

The association of blood manganese and non-alcoholic fatty liver disease stratified by cotinine exposure group.
The association of blood Mn level and NAFLD in two cotinine groups is exhibited in Table 4. In the cotinine unexposed group, the relationship between blood Mn and NAFLD was insignificant in three models (all P > 0.05). However, their relationship became significant in the cotinine-exposed group (all P < 0.05). When blood Mn was coded into three groups, the risk of NAFLD in the Tertile 3 group was positively related to blood Mn by taking the Tertile 1 groups as a reference. In the cotinine unexposed group, the OR of NAFLD in the tertile 3 group was 4.452 [95% CI: 1.283, 15.445] (P < 0.05), but this relationship was not statistically significant after controlling multiple variables in model 2 and model 3. In the cotinine-exposed group, the OR of NAFLD in the Tertile 3 group was higher in model 2 (OR [95% CI]: 2.410 [1.183, 4.911]) than the model 1 (OR [95% CI]: 1.823 [1.087, 3.057]). The association had a slight decrease when laboratory variables were added (OR [95% CI]: 2.236 [1.050, 4.762]). Whereas, blood Mn was notably linked to NAFLD independent of all the covariates in three models. These results indicated that the risk of NAFLD increased with blood Mn, which was further strengthened by the cotinine exposure.
Subgroup analysis
To further evaluate the role of blood Mn in NAFLD, we performed a subgroup analysis according to gender, race, PIR, and education (Table 5). There was an obvious relationship between blood Mn and NAFLD in subgroups of non-Hispanic White, and less than 9th grade (all P < 0.05). Non-Hispanic White had the highest OR of NAFLD with 1.090 in contrast to the Hispanic, Non-Hispanic Black, and other races. In addition, the participants in the lower education level group were more likely to suffer from NAFLD with statistical significance (P < 0.05) (Table 5).
Discussion
Emerging epidemiological evidence suggested a global surge in the prevalence of NAFLD among children, posing significant public health challenges2,33,34. Recent advancements in research have revealed that an accumulation of liver fat and steatosis occurred as a result of disruptions in lipid metabolism, insulin resistance, and the synergistic influence of genetic and environmental factors, ultimately fostering the progression of non-alcoholic steatohepatitis (NASH) and cirrhosis34. Additionally, a substantial body of statistics indicated that most NAFLD patients are afflicted with obesity, implying a potential association between obesity and the development of NAFLD35. Investigations have further demonstrated that obesity-related complications affect oxidative stress in children, stimulating the advancement of NAFLD through the modulation of pro-inflammatory and anti-inflammatory factors36,37. Animal experiments have substantiated that exposure of the liver to heightened levels of proinflammatory cytokines can induce histological changes that closely mimic NASH38. Consistent with earlier studies, our observations have revealed a significantly larger waist circumference in the NAFLD group compared to the non-NAFLD group.
Furthermore, our findings have unveiled a positive correlation between blood Mn levels and NAFLD. Mn is an essential trace element vital for human development39. However, excessive Mn levels may elevate the risk of immune toxicity across various vertebrate species40. An animal study has demonstrated that Mn injections promote inflammation in mice41. Moreover, Nakata et al. have asserted that high occupational exposure to Mn typically led to a decrease in T-lymphocytes among adult men42. The reduced presence of T regulatory cells (Tregs) has also been observed in animal models and humans with NAFLD43. On the other hand, Mn also plays a crucial role in metabolism. Elevated Mn levels may disrupt mitochondrial function by promoting the production of reactive oxygen species, reducing adenosine-triphosphate production, and modulating membrane permeability44, thereby contributing to oxidative stress and the progression of NAFLD45. These outcomes indicated that Mn exposure may facilitate the development of NAFLD through mediating immune responses and metabolism.
In addition, we also found that cotinine may enhance the association between Mn and NAFLD. Cotinine, a nicotine metabolite with an extended half-life, is frequently employed as an indicator for measuring smoking exposure22. Smoking increases the levels of heavy metals in a patient’s body. SHS also releases heavy metals into the air, including Mn, leading to heavy metal exposure in non-smokers and potentially raising their body levels of heavy metals46. Elevated blood Mn levels can lead to an increase in reactive oxygen species, inhibit adenosine triphosphate production, and alter membrane permeability, thereby disrupting normal mitochondrial function44. Mitochondrial dysfunction causes oxidative stress, which increases the levels of inflammatory cytokines in the body, triggering the “multiple hit” hypothesis and potentially leading to NAFLD8,34,47.
Nevertheless, this study possesses several limitations. Firstly, the data utilized is derived exclusively from the NHANES database, which primarily represents the American population. Secondly, the inherent limitation of NHANES renders no causality. Thirdly, some inflammatory markers are not recorded in the NHANES database, thereby preventing the inclusion of additional relevant indicators for a more comprehensive analysis. However, our study has several advantages. Firstly, the reliability and representativeness are bolstered by the utilization of large sample size and appropriate covariate adjustments. Secondly, the NAFLD diagnosis used in this study was specific to children, fostering credibility. This study paves the way for investigating the underlying mechanism of the modification of cotinine exposure on the relationship between blood Mn levels and pediatric NAFLD.
In conclusion, our findings establish a close and positive association between blood Mn levels and pediatric NAFLD, a relationship that can be intensified by cotinine exposure. However, the causal mechanisms and potential pathways necessitate further validation through subsequent studies.
Data availability
All data generated or analysed during this study are included in this supplementary information files.
References
Anderson, E. L. et al. The prevalence of non-alcoholic fatty liver disease in children and adolescents: A systematic review and Meta-analysis. PLoS One 10, e0140908. https://doi.org/10.1371/journal.pone.0140908 (2015).
Brecelj, J. & Orel, R. Non-alcoholic fatty liver disease in children. Med. (Kaunas) 57. https://doi.org/10.3390/medicina57070719 (2021).
Angulo, P. Nonalcoholic fatty liver disease. N Engl. J. Med. 346, 1221–1231. https://doi.org/10.1056/NEJMra011775 (2002).
Muzurovic, E. et al. Non-alcoholic fatty liver disease in children. Curr. Vasc. Pharmacol. 21, 4–25. https://doi.org/10.2174/1570161121666221118155136 (2023).
Nobili, V. et al. NAFLD in children: New genes, new diagnostic modalities and new drugs. Nat. Rev. Gastroenterol. Hepatol. 16, 517–530. https://doi.org/10.1038/s41575-019-0169-z (2019).
Schwimmer, J. B., Pardee, P. E., Lavine, J. E., Blumkin, A. K. & Cook, S. Cardiovascular risk factors and the metabolic syndrome in pediatric nonalcoholic fatty liver disease. Circulation 118, 277–283. https://doi.org/10.1161/CIRCULATIONAHA.107.739920 (2008).
Younossi, Z. et al. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 15, 11–20. https://doi.org/10.1038/nrgastro.2017.109 (2018).
Younossi, Z. M., Corey, K. E. & Lim, J. K. AGA clinical practice update on lifestyle modification using diet and exercise to achieve weight loss in the management of nonalcoholic fatty liver disease. Expert Rev. Gastroenterol. 160, 912–918. https://doi.org/10.1053/j.gastro.2020.11.051 (2021).
Jaishankar, M., Tseten, T., Anbalagan, N., Mathew, B. B. & Beeregowda, K. N. Toxicity, mechanism and health effects of some heavy metals. Interdiscip Toxicol. 7, 60–72. https://doi.org/10.2478/intox-2014-0009 (2014).
Guo, W. et al. Seasonal and spatial variation in dissolved heavy metals in Liaodong Bay, China. Int. J. Environ. Res. Public. Health. 19. https://doi.org/10.3390/ijerph19010608 (2022).
Kim, J. & Lee, K. Changes in urinary cotinine concentrations in non-smoking adults from the Korean National Environmental Health Survey (KoNEHS) II (2012–2014) after implementation of partial smoke-free regulations. Int. J. Hyg. Environ. Health 224, 113419. https://doi.org/10.1016/j.ijheh.2019.113419 (2020).
Lebeaupin, C. et al. Endoplasmic reticulum stress signalling and the pathogenesis of non-alcoholic fatty liver disease. J. Hepatol. 69, 927–947. https://doi.org/10.1016/j.jhep.2018.06.008 (2018).
Alkufi, A. A., Oleiwi, M. H. & Abojassim, A. A. Comparison of Heavy metals in urine samples of smoker and non-smoker persons. Biol. Trace Elem. Res. https://doi.org/10.1007/s12011-024-04097-5 (2024).
Abdulameer Alkufi, A., Hussain Oleiwi, M. & Abid Abojassim, A. Heavy metals in Blood serum of smokers and non-smoking controls. Curr. Anal. Chem. (2024).
Kulikowska-Karpinska, E., Zdanowicz, M. & Galazyn-Sidorczuk, M. [Estimation of copper in the urine of cigarette smokers]. Wiad. Lekc. 70, 697–702 (2017).
Oner, F., Mazlumoglu, M. R., Kurt, O., Kurt, N. & Ucuncu, H. Quantification of heavy metals in the nasal turbines of smokers and nonsmokers. Laryngoscope 134, 3562–3567. https://doi.org/10.1002/lary.31400 (2024).
Han, D. H., Lee, H. J. & Lim, S. Smoking induced heavy metals and periodontitis: findings from the Korea National Health and Nutrition examination surveys 2008–2010. J. Clin. Periodontol. 40, 850–858. https://doi.org/10.1111/jcpe.12133 (2013).
Lim, S. S. et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the global burden of Disease Study 2010. Lancet 380, 2224–2260. https://doi.org/10.1016/S0140-6736(12)61766-8 (2012).
Zein, C. O. Clearing the smoke in chronic liver diseases. Hepatology 51, 1487–1490. https://doi.org/10.1002/hep.23694 (2010).
Liu, Y. et al. Active smoking, passive smoking, and risk of nonalcoholic fatty liver disease (NAFLD): A population-based study in China. J. Epidemiol. 23, 115–121. https://doi.org/10.2188/jea.je20120067 (2013).
Kim, N. H. et al. Association between cotinine-verified smoking status and risk of nonalcoholic fatty liver disease. Liver Int. 38, 1487–1494. https://doi.org/10.1111/liv.13701 (2018).
Shen, H., Peng, J. L., Tayarachakul, S. & Liangpunsakul, S. Association between serum cotinine level and prevalence of non-alcoholic fatty liver disease: A cross-sectional study from the Third National Health and Nutrition Examination Survey. J. Investig. Med. 65, 43–48. https://doi.org/10.1136/jim-2016-000213 (2017).
Dearing, B. A., Katz, R. V. & Weitzman, M. Prenatal tobacco and postbirth second-hand smoke exposure and dental caries in children. Commun. Dent. Oral Epidemiol. 50, 130–138. https://doi.org/10.1111/cdoe.12642 (2022).
Abdel Hamed, N. A., Hammad, E. E. M., Salama, R. H., Yassa, H. A. & Awaga, M. M. Secondhand smoke as a risk factor for attention deficit hyperactivity disorder in children. Inhal Toxicol. 31, 420–427. https://doi.org/10.1080/08958378.2019.1705440 (2019).
Elster, A. B. & Kuznets, N.
Environmental tobacco smoke. A hazard to children. Am. Acad. Pediatr. Commun. Environ. Health Pediatr. 99, 639–642 (1997).
Wang, X., Mukherjee, B. & Park, S. K. Associations of cumulative exposure to heavy metal mixtures with obesity and its comorbidities among U.S. adults in NHANES 2003–2014. Environ. Int. 121, 683–694. https://doi.org/10.1016/j.envint.2018.09.035 (2018).
Wan, H. et al. Sex-specific associations of the urinary fourteen-metal mixture with NAFLD and liver fibrosis among US adults: A nationally representative study. Ecotoxicol. Environ. Saf. 248, 114306. https://doi.org/10.1016/j.ecoenv.2022.114306 (2022).
Li, W. et al. Analysis of environmental chemical mixtures and nonalcoholic fatty liver disease: NHANES 1999–2014. Environ. Pollut. 311, 119915. https://doi.org/10.1016/j.envpol.2022.119915 (2022).
Xu, B., Liu, Z., Zhao, J. & Yu, Z. Selenium intake help prevent age-related cataract formation: Evidence from NHANES 2001–2008. Front. Nutr. 10, 1042893. https://doi.org/10.3389/fnut.2023.1042893 (2023).
Flisiak-Jackiewicz, M., Bobrus-Chociej, A., Wasilewska, N. & Lebensztejn, D. M. From nonalcoholic fatty liver disease (NAFLD) to metabolic dysfunction-associated fatty liver disease (MAFLD)-new terminology in pediatric patients as a step in good scientific direction? J. Clin. Med. 10. https://doi.org/10.3390/jcm10050924 (2021).
Caudill, S. P., Schleicher, R. L. & Pirkle, J. L. Multi-rule quality control for the age-related eye disease study. Stat. Med. 27, 4094–4106. https://doi.org/10.1002/sim.3222 (2008).
Cohen, J. C., Horton, J. D. & Hobbs, H. H. Human fatty liver disease: Old questions and new insights. Science 332, 1519–1523. https://doi.org/10.1126/science.1204265 (2011).
Fang, Y. L., Chen, H., Wang, C. L. & Liang, L. Pathogenesis of non-alcoholic fatty liver disease in children and adolescence: from two hit theory to multiple hit model. World J. Gastroenterol. 24, 2974–2983. https://doi.org/10.3748/wjg.v24.i27.2974 (2018).
Lazo, M. & Clark, J. M. The epidemiology of nonalcoholic fatty liver disease: A global perspective. Semin. Liver Dis. 28, 339–350. https://doi.org/10.1055/s-0028-1091978 (2008).
Ji, Y., Liang, Y., Mak, J. C. W. & Ip, M. S. M. Obstructive sleep apnea, intermittent hypoxia and non-alcoholic fatty liver disease. Sleep. Med. 95, 16–28. https://doi.org/10.1016/j.sleep.2022.04.006 (2022).
Roden, M. Mechanisms of Disease: hepatic steatosis in type 2 diabetes–pathogenesis and clinical relevance. Nat. Clin. Pract. Endocrinol. Metab. 2, 335–348. https://doi.org/10.1038/ncpendmet0190 (2006).
Tomita, K. et al. Tumour necrosis factor alpha signalling through activation of Kupffer cells plays an essential role in liver fibrosis of non-alcoholic steatohepatitis in mice. Gut 55, 415–424. https://doi.org/10.1136/gut.2005.071118 (2006).
Huat, T. J. et al. Metal toxicity links to Alzheimer’s disease and neuroinflammation. J. Mol. Biol. 431, 1843–1868. https://doi.org/10.1016/j.jmb.2019.01.018 (2019).
Wu, Q., Mu, Q., Xia, Z., Min, J. & Wang, F. Manganese homeostasis at the host-pathogen interface and in the host immune system. Semin Cell. Dev. Biol. 115, 45–53. https://doi.org/10.1016/j.semcdb.2020.12.006 (2021).
Seth, P. et al. Early onset of virus infection and up-regulation of cytokines in mice treated with cadmium and manganese. Biometals 16, 359–368. https://doi.org/10.1023/a:1020682716212 (2003).
Nakata, A. et al. Decreases in CD8+ T, naive (CD4 + CD45RA+) T, and B (CD19+) lymphocytes by exposure to manganese fume. Ind. Health 44, 592–597. https://doi.org/10.2486/indhealth.44.592 (2006).
Van Herck, M. A. et al. The differential roles of T cells in non-alcoholic fatty liver disease and obesity. Front. Immunol. 10, 82. https://doi.org/10.3389/fimmu.2019.00082 (2019).
Anagianni, S. & Tuschl, K. Genetic disorders of manganese metabolism. Curr. Neurol. Neurosci. Rep. 19, 33. https://doi.org/10.1007/s11910-019-0942-y (2019).
Li, L. & Yang, X. The essential element Manganese, oxidative stress, and metabolic diseases: Links and interactions. Oxid. Med. Cell. Longev. 2018(7580707). https://doi.org/10.1155/2018/7580707 (2018).
Tang, X. D. & Destaillats, W. Inhalation of trace metals in secondhand and thirdhand tobacco smoke can result in increased health risks. Environ. Sci. Technol. 11, 329–334 (2024).
Fu, D. F. & Chen, B. The relationship between the systemic immune inflammation index and the nonalcoholic fatty liver disease in American adolescents. BMC Gastroenterol. 24, 233. https://doi.org/10.1186/s12876-024-03324-6 (2024).
Author information
Authors and Affiliations
Contributions
L.P.Z. and H.X.W. contributed to the conception and design. L.P.Z. and S.H.L., B.W.Q. contributed to the collection and assembly of data. H.X.W. and J.L.L. analyzed and interpreted the data. All authors wrote and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, Lp., Wei, Hx., Lin, Sh. et al. Cotinine exposure enhances the association of blood manganese and non-alcoholic fatty liver disease in American children: a cross-sectional study. Sci Rep 14, 24593 (2024). https://doi.org/10.1038/s41598-024-75298-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-75298-0
