
Abstract
A nomogram to estimate the risk of linezolid-induced thrombocytopenia in patients with renal impairment is not available. The aim of the study is to develop a nomogram for predicting linezolid-induced thrombocytopenia in patients with renal impairment and to investigate the incremental value of PNU-142300 concentration beyond clinical factors and linezolid trough concentration (Cmin) for risk prediction. Logistic regression was used to identify independent risk factors for linezolid-induced thrombocytopenia in patients with renal impairment and nomograms were established. The performance of the nomograms was assessed in terms of area under the receiver operating characteristic curve (AUROC), net reclassification improvement (NRI), integrated discrimination improvement (IDI) , decision curve analysis (DCA) and calibration. Internal validation and external validation of the nomograms were also performed. Four nomograms were created: nomogram A including total bilirubin, creatinine clearance and concomitant mannitol use; nomogram B containing linezolid Cmin additionally; nomogram C containing total bilirubin, concomitant mannitol use, linezolid Cmin, and PNU142300 concentration; nomogram D including total bilirubin, concomitant mannitol use, and PNU142300 concentration. Nomogram C improved the prediction performance than nomogram A (AUROC 0.881 vs. 0.749; NRI 0.290; IDI 0.226) and nomogram B (AUROC 0.881 vs. 0.812; NRI 0.152; IDI 0.130) in the training cohort. DCA analysis showed that nomogram C yielded a greater net benefit. Compared with nomogram A and nomogram B, nomogram C also showed superior discriminatory efficacy, good calibration and clinical usefulness in the external validation cohort. The nomogram containing PNU-142300 concentration and linezolid Cmin had better predictive capability than that containing linezolid Cmin for predicting linezolid-induced thrombocytopenia in patients with renal impairment.
Similar content being viewed by others
Introduction
Hospital-acquired pneumonia account for a substantial proportion of healthcare-associated infections, leading to high mortality and huge use of health-care resources1. Linezolid is recommended for treating patients with renal impairment and hospital-acquired pneumonia caused by multidrug-resistant Gram-positive organisms2. Nevertheless, its clinical utility is limited by the development of linezolid-induced thrombocytopenia, which may cause increased bleeding events, prolonged hospital stays, elevated hospital costs and increased mortality3,4. It has been reported that patients with renal impairment experienced more frequently linezolid-induced thrombocytopenia than those with normal renal function5,6.Therefore, it is necessary to develop risk models for predicting the occurrence of linezolid-induced thrombocytopenia in patients with renal impairment.
Previous studies have shown that clinical factors, such as baseline platelet level7, urea8, duration of linezolid therapy9, as well as concentration factors, such as linezolid trough concentration (Cmin)10 may be risk factor related to linezolid-induced thrombocytopenia. However, these studies were not focusing exclusively on patients with renal impairment. Recently, the two major metabolites of linezolid, namely hydroxyethyl-glycine metabolite (PNU-142586) and aminoethoxyacetic acid metabolite (PNU-142300), have also been found to be accumulated in patients with renal impairment11. An observational study performed by Wang et al. identified that a concentration ratio of PNU-142300 to linezolid more than 1.31 was the risk factor for predicting linezolid-induced thrombocytopenia using univariate analysis12. To date, the influence of these two metabolites on the development of linezolid-induced thrombocytopenia has not been fully elucidated. Given that the lack of standard substance of PNU-142586 in China, the relationship of linezolid Cmin and PNU-142300 concentration with linezolid-induced thrombocytopenia in critical ill patients was investigated in our prior work by multiple logistic regression analysis13.The pathophysiological characteristics of patients varied substantially between different populations, resulting in altered linezolid disposition14, which may further lead to the diversity of predictors of linezolid-induced thrombocytopenia across the different populations. There are currently limited risk factors for predicting linezolid-induced thrombocytopenia in patients with renal impairment. Furthermore, it remains unclear whether the PNU-142300 concentration adds incremental predictive value to the clinical factors and linezolid Cmin. Nomogram is a suitable tool, which has been widely utilized for quantifying individual risk to make clinical decision15.
The aim of this study is to develop and validate a nomogram that could identify patients with renal impairment who are at increased risk of linezolid-induced thrombocytopenia and to investigate the incremental value of PNU-142300 concentration over clinical factors and linezolid Cmin for predicting linezolid-induced thrombocytopenia in patients with renal impairment. The nomogram provides superior prediction capacity may assist clinicians in the early identification of patients at risk for linezolid-induced thrombocytopenia and further implementation of strategies to prevent its onset.
Methods
Study population
This prospective investigation was carried out between July 2021 and April 2024 in the Affiliated Suzhou Hospital of Nanjing Medical University and Suzhou Science and Technology Town Hospital. Eligible patients were included if (1) age ≥ 18 years; (2) with renal impairment (creatinine clearance [CrCL] < 60 mL/min); (3); administrated with linezolid for suspected or confirmed infections. The exclusion criteria were: (1) had a baseline platelet count less than 75,000/µl; (2) treated with linezolid for less than one week; (3) platelet count missed at baseline or after linezolid therapy; (4) accompanied by known bleeding disorders; (5) with severe hepatic impairment; (6) underwent renal replacement therapy, hemodialysis or extracorporeal membrane oxygenation. The definition of renal insufficiency was based on the US Food and Drug Administration updated guidance in 201016.The CrCL values were estimated using the Cockroft–Gault formula. The study was approved by the ethical committees of the two hospitals (K-2021-012 and IRB2021042) and all methods were performed in accordance with the relevant guidelines and regulations. Written informed consent was obtained from the patients or legally authorized representatives prior to inclusion in the study.
Dosing regimen and measurement of concentration
Linezolid was administered at a standard dose of 600 mg q12h or 300 mg q12h for patients with renal impairment according to the package label17 and the Sanford guide18. Samples of venous blood serum samples were taken at least 48 h after initiation of linezolid therapy and immediately or 30 min prior to the next dose. Collected blood samples were centrifuged at 4000 g for 10 min and the resulting serum was stored at − 80 °C until further analysis. Simultaneous quantification of linezolid and its metabolite PNU-142300 in human serum was performed by a validated liquid chromatography–tandem mass spectrometry (LC/MS/MS) assay as described previously13. Linezolid and PNU-142300 was extracted from the serum by protein precipitation, using acetonitrile containing a deuterated internal standard (d3-linezolid). The chromatographic separation was achieved on a Acquity UPLC BEH C18 column (1.7 μm, 50 mm×2.1 mm, Waters). The mass spectrometer was operated under multiple reaction monitoring mode with positive electrospray ionization. Quantifying of linezolid and PNU-142300 was validated over the 0.1-50 mg/L concentration range with satisfactory accuracies (− 8.05-8.33%), intra-day precisions (≤ 4.33%) and inter-day precisions (≤ 7.73%). Other details on the determination of linezolid and PNU-142300 are described in the Supplementary methods. Clinicians were free to independently decide whether and how to adjust the dosage regimen based on steady-state Cmin.
Data collection
The following data, such as patient demographic information, clinical characteristics, microbiological information, laboratory values, treatment regimens, linezolid Cmin, and PNU-142300 concentrations were collected from the hospital information system by trained staff at each participating center. Linezolid-induced thrombocytopenia was defined as a platelet count of less than 112,500/µl for patients with baseline platelet count maintained at a normal range, or a ≥ 25% reduction of platelet count from baseline for patients with platelet count below the lower limit of normal at baseline (75000–149000 /µl).
Development and assessment of the prediction models
Multiple imputations with chained equations were applied to estimate the missing data over 10 iterations and the results were pooled by Rubin’s rules. Candidate risk factors associated with the development of linezolid-induced thrombocytopenia were selected based on previous studies and the availability of clinical data. Univariate logistic analysis was performed to evaluate significance of candidate predictor variables and variables with P < 0.05 were stratified into the following categories: clinical risk factors, linezolid Cmin and PNU-142300 concentration. To evaluate whether concentration factors could improve the risk prediction of linezolid-induced thrombocytopenia, four models were established: Model A, all univariately statistically significant clinical variables entered in the multivariate model using a backward stepwise approach; Model B, additionally incorporating linezolid Cmin to the clinical variables; Model C, additionally incorporating linezolid Cmin and PNU-142300 concentrations to the clinical variables; Model D, additionally incorporating PNU-142300 concentrations to the clinical variables.
Four nomograms were generated to predict the occurrence of linezolid-induced thrombocytopenia based on the predictive models. The performance of the nomograms was assessed by area under the receiver operating characteristic curve (AUROC), net reclassification improvement (NRI), and integrated discrimination improvement (IDI). Decision curve analysis (DCA) was used to investigate the potential clinical effects of the prediction nomograms by quantifying the net benefits across a range of threshold probabilities. The calibration was evaluated using calibration curve and the Hosmer-Lemeshow test. Internal validation of the nomograms was performed using leave-one-out cross-validation and bootstrap resampling method. The performance of the nomograms for predicting linezolid-induced thrombocytopenia was also evaluated in an external validation cohort in terms of discrimination, calibration, and clinical utility.
Statistical analysis
Categorical variables are expressed as frequencies and percentages, and continuous variables as means and standard deviations or median and interquartile range (IQR), where appropriate. Differences in patient characteristics between groups were assessed using the Pearson chi-square test or Fisher’s exact test for categorical variables and independent t-test or Mann–Whitney U test for continuous variables. The linearity assumption of each continuous variable was confirmed via the Box-Tidwell test. Multicollinearity between variables in all models was checked using the variance inflation factor. The Delong test was used to compare the AUROC between nomogram A, nomogram B , nomogram C and nomogram D. All statistical tests of the hypotheses were two-sided and performed at the significance level of 0.05. All statistical analyses were performed using the SPSS, version 23 (SPSS Inc., Chicago, IL, USA), R programming language (version 4.3.1) and GraphPad Prism (version 9).
Results
Patient characteristics
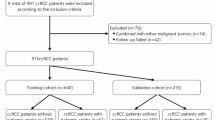
For the training cohort, 310 patients with renal impairment met our inclusion criteria, of whom 84 were excluded and 226 were finally included (Fig. 1). 78 patients with renal impairment from the Suzhou Science and Technology Town Hospital were used for external validation purposes (Fig. S1). The baseline characteristics of patients were comparable between the training and validation cohorts, as displayed in Table 1. In the training and validation cohorts, 10.6% and 11.5% of patients received concomitant mannitol to treat encephaledema, respectively. 76 (33.6%) and 29 (37.2%) patients developed linezolid-induced thrombocytopenia in the training and validation cohorts, respectively.

Flow chart for patient selection in the training cohort.
Risk prediction model development
No multicollinearity was found among the covariates in the models by using the variance inflation factor (all value < 5). As shown in Supplementary Table S1, all univariate statistically significant clinical variables were then included in the multivariate logistic regression analysis, and baseline total bilirubin level, CrCL value and concomitant mannitol use were found to be the independent risk factors for predicting linezolid-induced thrombocytopenia. A clinical prediction model (model A) was finally established by incorporating the three independent clinical risk factors. In model B, linezolid Cmin as well as the risk factors mentioned above were predictive for the occurrence of linezolid-induced thrombocytopenia. In model C, the following variables were predictive for linezolid-induced thrombocytopenia: total bilirubin, concomitant mannitol use, linezolid Cmin and PNU-142300 concentration, whereas CrCL value was not independently predictive. In model D, total bilirubin, concomitant mannitol use, and PNU-142300 concentration were predictive for linezolid-induced thrombocytopenia (Table 2).
Construction of the nomograms and evaluation of the predictive performance
Four nomograms were generated to predict the occurrence of linezolid-induced thrombocytopenia based on the prediction models (Fig. 2). Each risk factor was assigned a score, and all scores were then added together to predict the probability of linezolid-induced thrombocytopenia in each patient with renal impairment. Details of the prediction performance for all nomograms in the training cohort are provided in Table 3. Compared with nomogram A, nomogram B and nomogram C both had better discrimination, as demonstrated by significant increases in AUROC (0.812 vs. 0.749; and 0.881 vs. 0.749; respectively), and significant improvement in reclassification with NRI (0.139;95% CI, 0.010–0.268 and 0.290; 95% CI, 0.157–0.424, respectively) and IDI (0.096; 95% CI, 0.052–0.141 and 0.226; 95% CI, 0.165–0.287, respectively). Compared with nomogram B, nomogram C had better discrimination with a significant increase in AUROC to 0.881, and significant improvement in reclassification as assessed by the NRI (0.152; 95% CI, 0.030–0.273) and the IDI (0.130; 95% CI, 0.083–0.178). Compared with nomogram D, AUROC of nomogram C was increased, although the difference was not significant. IDI analysis showed that the discrimination ability of nomogram C was improved in comparison with nomogram D (Fig. 3A). DCA analysis showed significantly greater net benefit of the nomogram C was achieved in comparison with the other nomograms across a wide range of threshold probabilities for predicting linezolid-induced thrombocytopenia (Fig. 3B). The calibration curves and Hosmer-Lemeshow test (P > 0.05) in the training cohort indicated good calibration of the nomograms (Fig. S2 A1-D1).

The nomograms to predict the occurrence of linezolid-induced thrombocytopenia based on the prediction model A (A), model B (B), model C (C) and model D (D).

The ROC curves and DCA curves of predictive nomograms in the training cohort and validation cohort. (A) The ROC curves of predictive nomograms in the training cohort. (B) The DCA curves of predictive nomograms in the training cohort. (C) The ROC curves of predictive nomograms in the validation cohort. (D) The DCA curves of predictive nomograms in the validation cohort.
Validation of the nomograms
The nomogram A, nomogram B, nomogram C and nomogram D achieved an AUROC of 0.731, 0.796, 0.862 and 0.850 using leave-one‐out cross‐validation, respectively. By means of bootstrap method, the AUROC of nomogram A, nomogram B, nomogram C and nomogram D was 0.732, 0.794, 0.867, and 0.855, respectively. The four nomograms were externally validated in an independent cohort. Compared with nomogram A and nomogram B, nomogram C had the highest predictive capability (Fig. 3C), as demonstrated by significant increases in AUROC (0.878 vs. 0.735; and 0.878 vs. 0.795; respectively) and significant improvement in reclassification with NRI (0.345;95% CI, 0.123–0.566 and 0.158; 95% CI, 0.004–0.312, respectively) and IDI (0.243; 95% CI, 0.175–0.311 and 0.129; 95% CI, 0.057-0.200, respectively) (Supplementary Table S2). Moreover, the DCA suggested that the nomogram C provided increased net benefit compared to the nomogram A and nomogram B across a wide range of threshold probabilities in the validation cohort (Fig. 3D). The calibration plots of predicted versus observed probability and Hosmer–Lemeshow test (P > 0.05) also demonstrated good calibration for the nomograms in the external validation cohort (Fig. S2 A2-D2).
Discussion
To the best of our knowledge, this is the first study to evaluate the incremental value of PNU-142300 concentration beyond clinical factors and linezolid Cmin for predicting linezolid-induced thrombocytopenia in patients with renal impairment. Risk discrimination was significantly improved by incorporating PNU-142300 concentration into the nomogram including clinical variables and linezolid Cmin. Our findings suggest that PNU-142300 concentration may be as informative in terms of risk prediction as established clinical risk factors and linezolid Cmin. The nomogram incorporating PNU-142300 concentration, linezolid Cmin and clinical factors may facilitate physicians in identifying patients with renal impairment who are at increased risk of linezolid-induced thrombocytopenia and initiating strategies to prevent its occurrence.
Linezolid-induced thrombocytopenia occurred in 33.6% and 37.2% of the training cohort and validation cohort, respectively. The result was similar to that reported in Crass et al.’s study5, who found that linezolid-induced thrombocytopenia occurred more frequently among patients with renal impairment. Therefore, early identification of patients with renal impairment treated with linezolid who are at increased risk of linezolid-induced thrombocytopenia is of great importance.
A multivariable logistic regression analysis of clinical variables revealed that higher baseline total bilirubin level, lower CrCL value were associated with an increased risk of linezolid-induced thrombocytopenia, whereas concomitant mannitol use was associated with a lower risk. Consistent with the previous studies5,19,20 conducted in adult or critical ill patients, baseline total bilirubin level was identified as an independent risk factor for predicting linezolid-induced thrombocytopenia. Our study suggested that decreased CrCL was associated with increased odds of developing linezolid-induced thrombocytopenia, which was in agreement with the previous reports in adult Japanese patients21,22.CrCL was found to be a significant covariate affecting linezolid clearance after multiple-dose administration23,24.The clearance of linezolid decreases further as the deterioration of kidney function, which may increase the risk of linezolid-induced thrombocytopenia. Notably, concomitant mannitol use was firstly found to be associated with a reduced risk of linezolid-induced thrombocytopenia in patients with renal impairment in the present study. It might be attributed to the fact that the clearance of linezolid was enhanced in patients with concomitant mannitol use, thereby reducing the likelihood of linezolid-induced thrombocytopenia.
Accumulating evidence has suggested that linezolid Cmin may be a key predictive factor for developing linezolid-induced thrombocytopenia10,25,26, however, few studies evaluated the utility of linezolid Cmin beyond clinical factors to improve risk prediction of linezolid-induced thrombocytopenia in patients with renal impairment. Our findings suggested that the addition of linezolid Cmin to the model that include clinical variables can improve the predictive value of linezolid-induced thrombocytopenia. Several mechanisms responsible for linezolid-induced thrombocytopenia have been proposed, including an increase in the elimination of platelets or inhibition of platelet proliferation27,28,29. Boak et al.30found that the formation of platelet precursor cells was suppressed by 50% when linezolid Cmin exceeded the threshold. Tsuji et al.27 reported that 97% of patients developed linezolid-induced thrombocytopenia via an inhibitory mechanism, rather than simulation of platelet destruction. Hence, it is more likely that increased linezolid exposure may lead to linezolid-induced thrombocytopenia by inhibiting platelet formation.
Relatively few prior studies have evaluated the relationship between PNU-142300 concentration and linezolid-induced thrombocytopenia. Wang et al.12reported that the concentration ratio of PNU-142300 to linezolid exceeding 1.31 was associated with an increased risk of developing linezolid-induced thrombocytopenia. However, only one factor was assessed in the study, other potential significant risk factors were not evaluated by multivariate logistic regression analysis. Our previous research indicated that linezolid-induced thrombocytopenia was independently related to PNU-142300 concentration in critical ill patients by multiple regression analysis13. Nevertheless, the contribution of PNU-142300 concentration to the development of linezolid-induced thrombocytopenia in patients with renal impairment has not been fully explored. After adding the PNU-142300 concentration to the model consisting of linezolid Cmin and clinical variables, the PNU-142300 concentration was found to be independently associated with linezolid-induced thrombocytopenia. The relationship may be partly explained by the chemical structure similarity between linezolid and PNU-142300 (aniline functional group), since the potential myelotoxicity may be predicted from the chemical structure31,32. In addition, CrCL value was not identified as a significant predictor of linezolid-induced thrombocytopenia after PNU-142300 concentration was added to the model consisting of linezolid Cmin and clinical variables. It is suggested that PNU-142300 concentration could be equally or more useful than CrCL value for identifying individuals with renal impairment who are more likely to develop linezolid-induced thrombocytopenia. It may be attributed to the fact that PNU-142300 was also accumulated in patients with renal impairment13, thus increasing the likelihood of occurring linezolid-induced thrombocytopenia.
The risk model established by Qin et al.33 and Maray et al.34 for predicting linezolid-induced thrombocytopenia achieved an AUROC of 0.795 and an AUROC of 0.80, respectively. However, the prediction models were constructed based on data collected from elderly patients or critically ill patients. By focusing exclusively on patients with renal impairment in the present study, the prediction model comprised of PNU-142300 concentration along with linezolid Cmin and clinical variables exhibited good discrimination ability, with an AUC of 0.881 in the training cohort. The nomograms were built for visualizing the models. Importantly, our study confirmed that the nomogram comprised of PNU-142300 concentration along with linezolid Cmin and clinical variables had better predictive capability than the nomogram comprised of linezolid Cmin and clinical variables in the training cohort and validation cohort, as demonstrated by significant improvements in AUC, NRI and IDI. The nomogram incorporating both linezolid Cmin and PNU-142300 concentration had increased AUROC compared with the nomogram incorporating PNU-142300 concentration without linezolid Cmin, although the difference was not significant. IDI analysis showed the addition of both linezolid Cmin and PNU-142300 concentration significantly improved the discrimination compared to the nomogram comprised of PNU-142300 concentration without linezolid Cmin. in the derivation cohort. It suggested that both linezolid Cmin and PNU-142300 concentration contributed to the development of linezolid-induced thrombocytopenia. Given the limited sample size of the present study, a future prospective study with a larger sample size is warranted to verify the difference of discrimination ability between the nomogram incorporating both linezolid Cmin and PNU-142300 concentration and the nomogram consisting of PNU-142300 concentration without linezolid Cmin. Our findings indicate that incorporating concentration variables, such as linezolid Cmin and PNU-142300 concentration, into clinical risk prediction nomogram may be more helpful in identifying patients with renal impairment at increased risk of linezolid-induced thrombocytopenia and in making risk management decisions to prevent its occurrence.
This study has several limitations. First, the standard substance of PNU-142586 is not available in China so far, therefore, the contribution of PNU-142586 to the development of linezolid-induced thrombocytopenia in patients with renal impairment has not been explored in the present study. Second, the present study was exploratory given the limited sample size in the training cohort, and inclusion of more patients with renal impairment from multi-center are still needed to verify the incremental value of PNU-142300 concentration for predicting linezolid-induced thrombocytopenia. Third, only 78 patients with renal impairment were enrolled in the external validation cohort, and further validation with a larger sample size is still necessary. Fourth, since renal replacement therapy patients were excluded from the present study, there is limited possibility to generalize the predicted nomogram to patients with renal insufficiency who received renal replacement therapy. In future work, the role of PNU-142300 played in other hematologic abnormalities, such as anemia, may also be investigated. In addition, a population pharmacokinetic model of linezolid and PNU-142300 in patients with renal impairment may be developed to characterize the pharmacokinetic parameters and to explore the optimal dosage strategy in this population.
Conclusion
The nomogram comprised of PNU-142300 concentration along with linezolid Cmin and clinical variables had better predictive capability than the nomogram comprised of linezolid Cmin and clinical variables in the training and external validation cohort. The visual nomogram can be utilized by the clinicians to evaluate the risk of linezolid-induced thrombocytopenia in patients with renal impairment and to initiate strategies to prevent its occurrence.
Data availability
The data analyzed in this study are available from the corresponding author on reasonable request.
References
Magill, S. S. et al. Changes in prevalence of Health Care-Associated infections in U.S. hospitals. N Engl. J. Med. 379, 1732–1744 (2018).
Kalil, A. C. et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 Clinical practice guidelines by the infectious diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 63, e61–e111 (2016).
Dai, Y. et al. Analysis of the risk factors of linezolid-related haematological toxicity in Chinese patients. J. Clin. Pharm. Ther. 46, 807–813 (2021).
Kim, H. S., Lee, E., Cho, Y. J., Lee, Y. J. & Rhie, S. J. Linezolid-induced thrombocytopenia increases mortality risk in intensive care unit patients, a 10 year retrospective study. J. Clin. Pharm. Ther. 44, 84–90 (2019).
Crass, R. L., Cojutti, P. G., Pai, M. P. & Pea, F. Reappraisal of linezolid dosing in renal impairment to improve safety. Antimicrob. Agents Chemother. 63, e00605-00619 (2019).
Shi, C. et al. Effect of renal function on the risk of thrombocytopaenia in patients receiving linezolid therapy: A systematic review and meta-analysis. Br. J. Clin. Pharmacol. 88, 464–475 (2022).
Kaya Kılıç, E. et al. Risk factors for linezolid-associated thrombocytopenia and negative effect of carbapenem combination. J. Infect. Developing Ctries. 13, 886–891 (2019).
Zhao, X. et al. Prediction of risk factors for linezolid-induced thrombocytopenia based on neural network model. Front. Pharmacol. 15, 1292828 (2024).
Choi, G. W. et al. Risk factors for linezolid-induced thrombocytopenia in patients without haemato-oncologic diseases. Basic. Clin. Pharmacol. Toxicol. 124, 228–234 (2019).
Cazavet, J. et al. Risk factor analysis for linezolid-associated thrombocytopenia in critically ill patients. Eur. J. Clin. Microbiol. Infect. Dis. 39, 527–538 (2020).
Souza, E., Crass, R. L., Felton, J., Hanaya, K. & Pai, M. P. Accumulation of Major Linezolid Metabolites in Patients with Renal Impairment. Antimicrob. Agents Chemother. 64 (2020).
Wang, Y. et al. UPLC-MS/MS assay for the measurement of linezolid and its metabolite PNU-142300 in human serum and its application to patients with renal insufficiency. Front. Pharmacol. 12, 641872 (2021).
Xu, J. et al. Establishment and validation of a risk prediction model incorporating concentrations of linezolid and its metabolite PNU142300 for linezolid-induced thrombocytopenia. J. Antimicrob. Chemother. 78, 1974–1981 (2023).
Lin, B. et al. Expert consensus statement on therapeutic drug monitoring and individualization of linezolid. Front. Public. Health. 10, 967311 (2022).
Zheng, G. et al. Development of a risk prediction model for subsequent infection after colonization with carbapenem-resistant Enterobacterales: A retrospective cohort study. Antimicrob. Resist. Infect. Control 13, 46 (2024).
U.S. Department of Health and Human Services. Guidance for industry pharmacokinetics in patients with impaired renal function-study design, data analysis, and impact on dosing. (2010). https://www.fda.gov/media/78573/download
FDA. Highlights of prescribing information for ZYVOX. (2018). https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/206473s002lbl.pdf
Gilbert, D. N., Chambers, H. F. & Saag, M. S. The Sanford guide to antimicrobial therapy (Antimicrobial Therapy, Inc., 2020).
Rabon, A. D., Fisher, J. P. & MacVane, S. H. Incidence and risk factors for development of thrombocytopenia in patients treated with linezolid for 7 days or greater. Ann. Pharmacother 52, 1162–1164 (2018).
Takahashi, S. et al. Classification tree analysis based on machine learning for predicting linezolid-induced thrombocytopenia. J. Pharm. Sci. 110, 2295–2300 (2021).
Hanai, Y. et al. A retrospective study of the risk factors for linezolid-induced thrombocytopenia and anemia. J. Infect. Chemother. 22, 536–542 (2016).
Hirano, R., Sakamoto, Y., Tachibana, N. & Ohnishi, M. Retrospective analysis of the risk factors for linezolid-induced thrombocytopenia in adult Japanese patients. Int. J. Clin. Pharm. 36, 795–799 (2014).
Sakurai, N. et al. Population pharmacokinetics of linezolid and its major metabolites PNU-142300 and PNU-142586 in adult patients. Pharmacotherapy. 42, 707–715 (2022).
Wu, F. et al. Dosage strategy of linezolid according to the trough concentration target and renal function in chinese critically ill patients. Front. Pharmacol. 13 (2022).
Cheng, C. N. et al. Impact of high plasma concentrations of linezolid in Taiwanese adult patients- therapeutic drug monitoring in improving adverse drug reactions. J. Formos. Med. Assoc. 120, 466–475 (2021).
Kawasuji, H. et al. Proposal of initial and maintenance dosing regimens with linezolid for renal impairment patients. BMC Pharmacol. Toxicol. 22, 13 (2021).
Tsuji, Y. et al. Population pharmacokinetics and pharmacodynamics of linezolid-induced thrombocytopenia in hospitalized patients. Br. J. Clin. Pharmacol. 83, 1758–1772 (2017).
Pascoalinho, D., Vilas, M. J., Coelho, L. & Moreira, P. Linezolid-related immune-mediated severe thrombocytopenia. Int. J. Antimicrob. Agents. 37, 88–89 (2011).
Bernstein, W. B., Trotta, R. F., Rector, J. T., Tjaden, J. A. & Barile, A. J. Mechanisms for linezolid-induced anemia and thrombocytopenia. Ann. Pharmacother. 37, 517–520 (2003).
Boak, L. M. et al. Clinical population pharmacokinetics and toxicodynamics of linezolid. Antimicrob. Agents Chemother. 58, 2334–2343 (2014).
Wu, F. et al. Dosage strategy of linezolid according to the trough concentration target and renal function in chinese critically ill patients. Front. Pharmacol. 13, 844567 (2022).
Crivori, P., Pennella, G., Magistrelli, M., Grossi, P. & Giusti, A. M. Predicting myelosuppression of drugs from in silico models. J. Chem. Inf. Model. 51, 434–445 (2011).
Qin, Y., Chen, Z., Gao, S., Shen, Y. & Ye, Y. Development and validation of a risk prediction model for linezolid-induced thrombocytopenia in elderly patients. Eur. J. Hosp. Pharm. 31, 94–100 (2024).
Maray, I. et al. Linezolid induced thrombocytopenia in critically ill patients: Risk factors and development of a machine learning-based prediction model. J. Infect. Chemother. 28, 1249–1254 (2022).
Acknowledgements
The authors would like to thank all the clinicians and nurses for their assistance in carrying out this study.
Funding
This work was supported by the Suzhou Science and Technology Project (SKJYD2021170, SKJYD2021171, SKJYD2021172); Jiangsu Pharmaceutical Association Hospital Pharmacy Research Project (H202109, A202228, SY202304-3, H202334); Jiangsu Research Hospital Association for Precision Medication (JY202203, JY202204, JY202212); Suzhou Pharmaceutical Association Hospital Pharmacy Research Project (Syhky202313, Syhky202312); Suzhou Special Technical Project for Diagnosis and Treatment of Key Clinical Diseases (LCZX202112); Gusu Talent Program (GSWS2022069) and Collaborative Innovation Project of Gusu School of Nanjing Medical University (GSKY20240207); Clinical Research Fund of Nanjing Medical University (2024KF0237); Drug Safety Research Project by Adverse Drug Reactions Journal (ADR2024MS21); China Medical and Health Development Foundation (202427).
Author information
Authors and Affiliations
Contributions
HZ and LT have contributed equally to this work.HZ established the prediction models and wrote the manuscript; LT designed the study; ZZ performed the study; JX revised the manuscript; YY supervised the study; QZ helped in data collection and data interpretation; YY performed the biological analysis; CZ drew the graphs; LD was responsible for statistical analysis; LS, JL, JL and YZ participated in data collection.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent for publication
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhao, H., Tang, L., Zhuang, Z. et al. A nomogram incorporating linezolid and metabolite concentrations for predicting linezolid induced thrombocytopenia in patients with renal impairment. Sci Rep 14, 26064 (2024). https://doi.org/10.1038/s41598-024-77768-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-77768-x
Keywords
This article is cited by
-
Development and validation of a nomogram to predict linezolid-induced thrombocytopenia in hospitalized adults
BMC Pharmacology and Toxicology (2025)
-
Nomogram for the prediction of valproic acid induced platelet decline: a nested case–control study
Scientific Reports (2025)
