
Abstract
Tunneled peripherally inserted central catheters (PICCs) are crucial for delivering long-term intravenous therapies to cancer patients. We compared PICC-related complications among different patient groups and identify potential factors contributing to these complications. A total of 402 cancer patients who received tunneled PICC placement in our hospital were enrolled in this study. We then compared their general data, PICC-related characteristics, pain score and anxiety score, and PICC-related complications. Extravasation length were varied significantly between groups, with the highest length observed in Group A4. Analysis of catheter type showed a predominance of 4Fr and 4 F catheters. Needle size and catheter material used also differed significantly between groups. High-pressure single-lumen catheters were the most common. In addition, pain and anxiety scores were significantly different between the groups, with the A3 group scoring the highest in both areas. There were significant differences between the groups in PICC-related complications, particularly “Difficulty in Removal”, which was significantly higher in the A4 group (7.2%). Attention to differences in gender distribution, BMI, PICC-related characteristics, and pain and anxiety scores in cancer patients in the clinical setting is important in developing an individualized approach to PICC placement.
Similar content being viewed by others

Chemotherapy is a principal treatment modality for cancer patients and can significantly enhance their prognosis. However, the frequent administration of chemotherapeutic agents often causes irritation, increasing the risk of phlebitis in the upper limbs. To prevent these venous complications and preserve the integrity of upper limb veins, clinicians commonly use a peripherally inserted central catheter (PICC), which not only establishes secure and effective venous access but also allows for the dilution of irritant drugs, leveraging the high blood flow rate in large veins1,2.
There has been significant evolution in PICCs since their inception in 1975, originally developed to provide safer and long-term intravenous access for a wide range of therapies3. Traditional non-tunneled PICCs, inserted directly into veins like the basilic, cephalic or brachial in the upper arm, became popular due to their ease of insertion and lower risk of complications than other central lines. However, the frequent use of non-tunneled PICCs has some limitations, such as higher risks of infection and catheter dislodgement, which led to the development of tunneled PICCs to create a subcutaneous tunnel between the insertion and exit sites of the catheter, significantly reducing infection risks and improving catheter stability, thus making them a preferred option in many clinical scenarios4 .
While PICC intervention enhances the safety of drug administration in cancer patients, it may also lead to some complications, such as bloodstream infections, oozing and catheter displacement during and after the insertion, culminating in unplanned extubation and complicating the process of catheter replacement. The risk of catheter-related bloodstream infections (CRBSIs) is significantly higher in patients who have undergone multiple PICC insertions or have a history of bloodstream infections. CRBSIs represent a significant and potentially life-threatening complication of PICC, characterized by their high incidence rate5,6.
Tunneled PICC, which involves creating a subcutaneous tunnel for venous access, represents a safer alternative due to the separation of the insertion site and catheter exit site. This design significantly reduces the likelihood of CRBSIs, oozing, and other associated complications7. In a randomized controlled study conducted by Dai et al.8, the authors compared the effects of tunneled and non-tunneled PICC in 174 participants and reported that the tunneled PICC (experimental group) was superior to the non-tunneled PICC (control group) in several aspects, such as association with a lower incidence of complications during placement, wound oozing, medical adhesive-related skin injury, venous thrombosis, and catheter dislodgement. Additionally, it was more cost-effective in terms of PICC maintenance over 1, 2 and 3 months and concluded that tunneled PICC placement was more effective and could be a preferred method in clinical settings. Moreover, a multicenter retrospective study assessed the safety and effectiveness of a new subcutaneously anchored securement device for tunneled central venous catheters in pediatric oncological patients across three Italian pediatric oncology units using various types of tunneled catheters (cuffed or non-cuffed, centrally, peripherally, or femorally inserted) secured with this device9. The data from 311 catheters showed a low incidence of dislodgment (2.6%) and minimal local pain or inflammation related to the device (1.9%). In addition, the authors reported that the rate of catheter-related bacteremias was also low, with no reported symptomatic catheter-related thrombosis, there was no significant difference in complications among different catheter types or between patients with hematologic versus solid tumors and concluded that the subcutaneously anchored securement device was well-tolerated and effective in preventing catheter dislodgment in pediatric oncological patients, regardless of the catheter type.
However, research on tunneled PICC technique as a new catheterization method, especially in cancer patients, remains limited in regard to related complications and risk factors. Thus, we designed this present study to assess and compare patient demographics, catheter characteristics and complication rates among patients receiving tunneled PICCs to enhance our clinical understanding and practice regarding PICC placements, aiming for improved patient care and reduced complication rates.
Materials and methods
Ethics approval and patient consent
This study was approved by the Ethics Committee of Shenzhen Hospital, Tumor Hospital, Chinese Academy of Medical Sciences (Approval No. 2020-47), in compliance with the Declaration of Helsinki. All patients and their families provided signed informed consent, which included detailed information about the tunneling technique, its off-label nature, potential risks, and expected benefits. Specific measures were implemented to ensure transparent communication and patient understanding.
General data
This study enrolled cancer patients who underwent tunneled PICC placement at our hospital between 2020 and 2023.
Inclusion criteria were as follows: (1) Diagnosed with cancer and aged over 18; (2) Ability and willingness to undergo tunneled PICC placement in the upper arm; (3) Could attend regular hospital visits for maintenance until catheter removal; (4) An intact and infection-free insertion site skin at the time of insertion; (5) A suitable upper arm basilic vein for catheter insertion; and (6) Patients and their families who are informed about this study and have signed a consent form.
Exclusion criteria included: (1) Presence of systemic infection or sepsis; (2) Severe coagulation disorders; (3) Local scarring or skin damage on the upper arm, venous sclerosis or cord-like changes; (4) Tumor compression of blood vessels, or superior vena cava syndrome; (5) A history of radiation, venous thrombosis, trauma or vascular surgery on the intended catheter side; and (6) Psychiatric disorders, severe cognitive impairment, or language barriers.
Tunneled PICC placement and grouping
PICC placement prioritized the right arm unless contraindicated. All procedures were performed under ultrasound guidance by trained and certified clinicians following standardized protocols. The catheter’s diameter was maintained at or below 45% of the chosen vessel’s diameter. The intended placement for the catheter tip was the lower third of the superior vena cava or the right atrium junction.
The tunneling technique involved creating a subcutaneous tunnel to separate the catheter’s insertion site from its exit site. This procedure was performed under strict aseptic conditions to minimize infection risks. Following the PICC Zone Insertion Method (ZIM)10, the upper arm was divided into three zones: the red zone (beginning at the medial epicondyle and extending one-third towards the Axillary Line), the green zone (the middle third of the upper arm), and the yellow zone (the upper third of the arm). The procedure involved inserting the catheter into larger veins in the yellow zone and then tunneling it under the skin to establish an exit site in the green zone.
Post-insertion, patients underwent energy subtraction chest X-ray to verify the catheter’s position. Initial dressing changes and catheter maintenance were conducted 48 h after insertion and then every week. These procedures were performed by trained and certified nursing staff.
All patients were divided into five groups (n = 80 per group) based on the length of the subcutaneous tunnel: 2 cm (A1 group), 3 cm (A2 group), 4 cm (A3 group), 5 cm (A4 group), and 6 cm (A5 group). This grouping aimed to assess how tunnel length affects key outcomes, including complication rates, catheter stability, and patient comfort, with shorter tunnels hypothesized to reduce discomfort and procedure time, while longer tunnels were expected to improve stability and lower infection risks. A detailed patient screening flowchart is presented in Fig. 1.

Patient screening flowchart.
Safety measures and documentation
To ensure safety and minimize risks associated with tunneling, the following measures were taken:
-
1.
Real-time ultrasound guidance during catheter insertion and tunneling.
-
2.
Use of catheters with proven flexibility and tensile strength to withstand mechanical stress.
-
3.
Detailed documentation of all procedures, including potential complications such as catheter damage, insertion difficulty, or displacement.
-
4.
Regular postoperative evaluations and follow-up to monitor for complications.
Evaluation indicators
Data collected included age, gender, body mass index (BMI), educational level, history of previous catheter placement, and medical history concerning diabetes and hypertension, along with the type of tumor diagnosed. We also conducted pre-catheterization blood tests, which involved measuring hemoglobin (Hb), white blood cell count (WBC, ×109/L), red blood cell count (RBC, ×109/L), platelets (PLT, ×109/L), prothrombin time (PT, sec), activated partial thromboplastin time (APTT, sec), fibrinogen (Fbg, g/L), and D-Dimer (DD, µg/mL). Characteristics specific to the PICC were also recorded, and the patients were regularly followed up after the initial treatment to record any complications occurring during the period with the catheter.
The quality of the operation for each group was assessed based on several criteria: the one-time success rate of catheter insertion and placement, the duration of catheter placement (measured in minutes), the amount of blood loss following placement, and the duration of catheter use (measured in days).
To evaluate the patients’ anxiety and pain levels after PICC use in each group, two scales were employed: the Hamilton Anxiety Scale (HAMA)11 and the Visual Analogue Scale (VAS)12.
Additionally, complications that occurred both during and after the procedures, such as catheter occlusion, venous thrombosis, infection at the insertion site and catheter displacement, were documented.
Statistical analysis
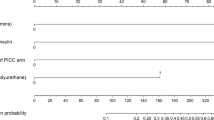
Data analysis was conducted using the SPSS software version 26.0. Quantitative data with normal distribution were presented as mean ± standard deviation (SD), and one-way analysis of variance followed Tukey’s post hoc test was performed to compare the differences among multiple groups. Qualitative data were expressed as numbers (n) or percentages (%), and the chi-square (χ2) test was used for comparative analysis between groups. Cox regression analysis was performed to identify risk factors for postoperative infections in patients. P < 0.05 was considered statistically significant.
Results
General data of patients
In this study, a total of 402 patients were assessed, among which Group A1-5 comprised 76, 80, 80, 83 and 83 cases, respectively. A comprehensive comparative analysis of baseline data among different groups to identify differences or trends in patient characteristics was conducted (Table 1). Despite some variation, there were no statistically significant differences in age observed between the groups (P = 0.109). The distribution of gender among the patient groups showed notable variation. Significant differences in gender distribution were observed among the groups (χ2 = 14.185, P = 0.007). In regard to BMI, Group A2 had the highest mean BMI of 23.08, whereas Group A5 had the lowest mean BMI of 21.81, and the differences in BMI were statistically significant (P = 0.032). Education level was examined to assess the background of the patients. While there were variations in education levels among the groups, the differences were not statistically significant (χ2 = 17.459, P = 0.133).
Previous catheter history was investigated, and we observed that all patient groups had no prior history of catheterization. Medical history, including diabetes and hypertension, was also recorded. While the presence of these conditions varied among the groups, no statistically significant differences were observed. The analysis of tumor types did not yield statistically significant differences (χ2 = 35.372, P = 0.159). Additionally, several laboratory parameters were measured, including Hb, WBC count, RBC count, PLT count, PT, APTT, Fbg and DD and no statistically significant differences were observed in these laboratory values among the patient groups.
Next, we assessed the various characteristics related to PICC placement among different patient groups (Table 2). In regard to catheter placement sites, the right basilic vein was found to be the most common site in all groups. Catheter length, pre-insertion length, catheter tip final position and vessel-to-catheter diameter ratio were measured and showed no significant differences among groups. Extravasation length, a measure of leakage, varied significantly between groups, with the highest length observed in Group A4. Catheter type analysis revealed that 4Fr and 4 F catheters were predominantly used. The needle size and catheter material used also showed significant differences among groups. High-Pressure Single-Lumen catheters were the most common, while High-Pressure Double-Lumen catheters and Bard catheters were less frequent. The number of insertions and catheter dwell time exhibited no significant differences among groups. Pain and anxiety scores were significantly different among groups (P < 0.01), with Group A3 having the highest scores for both (Table 3).
Comparison of the incidence of complications among the groups
In analyzing the complications associated with PICC lines across different groups (A1 to A5), significant differences in the occurrence of specific complications were observed (Table 4). Notably, “Difficulty in Removal” significantly varied among the groups, with a marked incidence in Group A4 (7.2%) and a lower occurrence in Group A5 (2.4%), while Groups A1, A2, and A3 reported no such difficulties (overall P = 0.002). Although “Incomplete Removal” and “Skin Damage” were observed, no statistically significant differences were observed across the groups, with a P value of 0.102 for both complications. “Puncture Site Infection” was uniformly low across all groups, showing no significant variation (P = 0.935), similar to the incidence of “Thrombosis” and “Mild Pain at Puncture Site,” which also did not vary significantly. The total complication rate was significantly higher in Group A4 (16.9%) compared to other groups, with Group A5 having a 6% complication rate, indicating a statistically significant difference across the groups (P < 0.001).
Discussion
PICCs are frequently used in clinical tumor treatment to establish venous access, with the common insertion sites including the basilic vein, median cubital vein and cephalic vein, and the catheter diameter being no more than 45% of the vessel’s diameter13. Despite their good utility, PICCs are also associated with significant clinical challenges, such as bloodstream infections and mechanical phlebitis following catheterization. Moreover, as the no. of chemotherapy cycles undergone by the patients increases, the patients’ physical condition often deteriorates, increasing the risk of catheter dislocation and displacement during physical activity, which can lead to unscheduled extubation. In this regard, a prospective cohort study by Krein et al.14 reported that 61.4% of 438 patients experienced at least one complication within 70 days, including serious complications such as bloodstream infections (17.6%) and deep vein thrombosis (30.6%). This high complication rate highlights the challenges associated with conventional PICC use. Comparatively, tunneled PICC, which involves creating a subcutaneous tunnel, offers advantages by separating the insertion and exit sites, reducing infection risks, and enhancing catheter stability15,16. Moreover, the skin’s contraction during movement can compress the insertion point, aiding in controlling oozing17. Therefore, tunneled PICC is particularly beneficial for oncology patients with challenging vascular conditions.
While the tunneling technique offers significant advantages, it is important to acknowledge that this represents an off-label modification to standard PICC placement. Although this technique is not explicitly addressed in the manufacturer’s guidelines, its clinical benefits, including reduced infection rates and improved catheter stability, are supported by multiple studies18,19. However, the lack of manufacturer validation necessitates further research and collaboration to establish standardized guidelines and ensure broader regulatory approval. Additionally, this study implemented strict procedural protocols and informed consent processes to mitigate risks associated with off-label use.
Our analysis revealed that an important finding was the significant variation in gender distribution, with Group A5 having the highest proportion of male patients (65.1%) and Group A4 having the lowest (37.3%). Additionally, we observed statistically significant differences in BMI among the groups, with Group A2 having the highest mean BMI (23.08) and Group A5 having the lowest (21.81). Education levels showed variations among the groups, but they were not statistically significant. Overall, these demographic characteristics provide valuable insights into the study population. The potential clinical impact of these findings lies in the recognition of gender and BMI differences among patients undergoing tunneled PICC placement. Understanding these variations might help healthcare providers tailor their approach to patient care and tunneled PICC management. For instance, male patients in Group A5 had a higher proportion, and their unique physiological characteristics might require specialized attention during placement. Moreover, recognizing the BMI differences, especially in patients with higher BMIs like those in Group A2, could lead to adjustments in catheter size and insertion techniques to ensure safe and effective placement. Additionally, acknowledging these variations may prompt healthcare providers to offer tailored psychological support20, such as counseling or relaxation techniques, to alleviate anxiety and discomfort during the procedure. By individualizing care based on these demographic characteristics, healthcare providers could enhance patient outcomes and overall comfort throughout the tunneled PICC placement process.
In a recent meta-analysis21, a comprehensive examination was conducted to systematically evaluate clinical factors contributing to catheter-related venous thrombosis in cancer patients with PICCs and the findings revealed several significant risk factors for PICC catheter thrombosis in cancer patients, including a history of chemotherapy, tumor type, tumor stage, presence or absence of metastasis and the utilization of specific chemotherapy agents such as fluorouracil, etoposide, platinum drugs, and taxane, suggesting the need for vigilance and closely monitoring of patients. Similarly, another study by Barrigah-Benissan et al.22 assessed the incidence, microbiology and contributing factors associated with PICC-related bloodstream infections (PR-BSI) and identified that the presence of fever and chills as significant independent factors. These studies highlight the importance of close monitoring and individualized interventions to manage PICCs effectively.
Comparatively, the analysis of different malignancies assessed in our study highlights the diversity of tumor types in clinical practice using tunneled PICC. While statistically significant differences in tumor distribution among patient groups were not observed, this diversity underscores the importance of a multidisciplinary approach to patient care. Additionally, the absence of statistically significant differences in tumor distribution suggests a relatively well-balanced representation of cancer types of the assessed study population, minimizing potential confounding variables. The ability to encompass a wide range of malignancies contributes to a comprehensive understanding of the patient population undergoing tunneled PICC placement, aiding healthcare providers and researchers in designing studies, developing treatment protocols, and predicting potential complications associated with specific cancer types23. Overall, this diversity highlights the complexity of cancer care and the need for individualized approaches to optimize patient outcomes.
Moreover, the results of this present study showed that while the right basilic vein was the most common placement site across all groups, we found significant differences in extravasation length, catheter type, needle size, and catheter material. Pain and anxiety scores also differed significantly among groups. These findings suggest that there are variations in PICC-related characteristics that should be considered when planning and executing tunneled PICC placement procedures. Tunneled PICC has been reported to be more stable and superior than traditional PICC24, but the pain score was reported to increase with increased tunnel length. To address this, it is critical to balance the advantages of tunneling with its potential discomfort, and future studies should aim to refine techniques that optimize patient safety and comfort.
From a clinical perspective, the variation in pain and anxiety scores emphasizes the need for psychological support and patient comfort during tunneled PICC placement25,26. By addressing patient-specific factors, healthcare providers can optimize patient comfort and minimize anxiety, which can lead to smoother procedures and potentially fewer complications. Thus, customizing tunneled PICC placement procedures could contribute to a more positive patient experience and improved clinical outcomes.
Additionally, numerous studies27,28 have shown that creating subcutaneous tunnels can significantly lower the rate of catheter-related complications, whereby for tunnels less than 5 cm in length, there could be no need for additional skin incisions or operations, leading to reduced maintenance costs and enhanced patient comfort. Our findings further revealed significant differences in complication rates across groups with varying tunnel lengths. Notably, the incidence of “Difficulty in Removal” was significantly higher in Group A4 (16.9%) and lower in Group A5 (2.4%). In contrast, other complications, such as “Incomplete Removal” and “Skin Damage”, were rare and not significantly different among the groups. The total complication rate was notably higher in Group A4, underscoring the need for careful consideration when selecting tunnel lengths. These findings suggest that while longer tunnels may provide greater stability, they could also pose challenges during catheter removal, warranting a balanced approach based on individual patient needs.
Several limitations should be acknowledged in the present study. Firstly, the retrospective nature of the study design may introduce inherent biases and limit the ability to establish causal relationships. Secondly, this study was conducted in a single-center setting and focused exclusively on oncology patients, which may limit the generalizability of the findings to broader populations, such as pediatric or non-oncology patients. Additionally, while we assessed various patient demographics and PICC-related characteristics, certain confounding factors that could influence outcomes were not included in the analysis. Furthermore, the absence of direct comparison with manufacturer-provided safety data and the lack of formalized training protocols highlight the need for standardization and further investigation. Finally, this study lacks long-term follow-up data to evaluate the durability and safety of tunneled PICC over extended periods. Future research should focus on long-term outcomes to address this limitation and provide a more comprehensive safety profile.
Despite these limitations, our study provides valuable insights into tunneled PICC placement, highlighting the importance of individualized approaches based on patient characteristics. These findings contribute to a growing body of evidence supporting the clinical benefits of tunneled PICCs and highlight the need for future research to optimize placement techniques and improve patient outcomes.
Conclusion
In conclusion, our study provides important insights into the demographics, placement characteristics, associated with tunneled PICCs in oncology patients. Key findings include variations in gender distribution, BMI, and PICC-related characteristics, as well as pain and anxiety scores across different tunnel lengths. These results emphasize the importance of individualized approaches to tunneled PICC placement, balancing patient comfort and procedural safety. While the study has certain limitations, it contributes valuable knowledge to the field of tunneled PICC placement and patient care, warranting further research in this area to optimize clinical practice and patient outcomes.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Gupta, N. et al. Tunneled and routine peripherally inserted central catheters placement in adult and pediatric population: Review, technical feasibility, and troubleshooting. Quant. Imaging Med. Surg. 11 (4), 1619–1627 (2021).
Duwadi, S., Zhao, Q. & Budal, B. S. Peripherally inserted central catheters in critically ill patients—Complications and its prevention: a review. Int. J. Nurs. Sci. 6 (1), 99–105 (2019).
Hoshal, V. L. Jr. Total intravenous nutrition with peripherally inserted silicone elastomer central venous catheters. Arch. Surg. 110 (5), 644–646 (1975).
Saijo, F. et al. A novel technique of axillary vein puncture involving peripherally inserted central venous catheters for a small basilic vein. J. Vasc Access. 19 (3), 311–315 (2018).
Gao, T. et al. Peripherally inserted central catheter-related bloodstream infections in patients with hematological malignancies: A retrospective 7-years single-center study. Am. J. Infect. Control. 50 (10), 1171–1177 (2022).
Pittiruti, M., Pelagatti, F. & Pinelli, F. Intracavitary electrocardiography for tip ___location during central venous catheterization: A narrative review of 70 years of clinical studies. J. Vasc Access. 22 (5), 778–785 (2021).
Maria, K. et al. Implementation of tunneled versus not tunneled peripherally inserted central catheters. J. Vasc Nurs. 37 (2), 132–134 (2019).
Dai, C. et al. Effect of tunneled and nontunneled peripherally inserted central catheter placement: A randomized controlled trial. J. Vasc Access. 21 (4), 511–519 (2020).
Crocoli, A. et al. Safety and effectiveness of subcutaneously anchored securement for tunneled central catheters in oncological pediatric patients: A retrospective study. J. Vasc Access. 24 (1), 35–40 (2023).
Dawson and B.J.J.o.t.A.f.V.A. Robert, PICC Zone insertion MethodTM (ZIMTM): A systematic Approach to Determine the Ideal insertion site for PICCs in the Upper Arm. J. Assoc. Vasc. Access 16(3), 156–165 (2011).
Thompson, E. Hamilton Rating Scale for Anxiety (HAM-A). Occup. Med. (Lond). 65 (7), 601 (2015).
Faiz, K. W. [VAS–visual analog scale]. Tidsskr Nor. Laegeforen. 134 (3), 323 (2014).
Estrada-Orozco, K. et al. Central venous catheter insertion and maintenance: Evidence-based clinical recommendations. Rev. Colomb Obstet. Ginecol. 71(2), 115–162 (2020).
Krein, S. L. et al. Patient-reported complications related to peripherally inserted central catheters: A multicentre prospective cohort study. BMJ Qual. Saf. 28 (7), 574–581 (2019).
Chen, X. et al. Selection of PICC catheter ___location in neonates via evidence-based ACE Star model. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 45 (9), 1082–1088 (2020).
Johansson, E. et al. Advantages and disadvantages of peripherally inserted central venous catheters (PICC) compared to other central venous lines: A systematic review of the literature. Acta Oncol. 52 (5), 886–892 (2013).
Ryan, C. et al. Protocol for a systematic review and thematic synthesis of patient experiences of central venous access devices in anti-cancer treatment. Syst. Rev. 7(1), 61 (2018).
Li, J. et al. Safety and effectiveness of tunneled peripherally inserted central catheters versus conventional PICC in adult cancer patients. Eur. Radiol. 34(12), 7776–7785 (2024).
Zheng, Y. et al. Comparison on clinical efficacy and adverse reactions between TPICC and ultrasound-guided PICC for advanced tumors: a retrospective study. Med. (Baltim). 103(42), e38130 (2024).
Song, J. & Ma, L. Effect of cognitive behavioral therapy and WeChat-based health education on patients underwent peripherally inserted central catheter line placement. Am. J. Transl Res. 13(12), 13768–13775 (2021).
Ma, S. et al. Clinical factors of PICC-RVT in cancer patients: A meta-analysis. Support Care Cancer. 31(7), 393 (2023).
Barrigah-Benissan, K. et al. Clinical factors associated with peripherally inserted central catheters (PICC) related bloodstream infections: A single centre retrospective cohort. Antimicrob. Resist. Infect. Control. 12(1), 5 (2023).
Conlon, T. W. et al. Development and implementation of a Bedside Peripherally Inserted Central Catheter Service in a PICU. Pediatr. Crit. Care Med. 20(1), 71–78 (2019).
Wang, Y. et al. The influential factors and intervention strategies that engage malignant cancer patients in health-promoting behaviors during PICC line maintenance. Am. J. Transl Res. 13(5), 5208–5215 (2021).
Verma, A. A. et al. Appropriateness of peripherally inserted central catheter use among general medical inpatients: An observational study using routinely collected data. BMJ Qual. Saf. 29(11), 905–911 (2020).
Zambelli, Z. et al. The 2021 NICE guidelines for assessment and management of chronic pain: A cross-sectional study mapping against a sample of 1,000* in the community. Br. J. Pain. 16(4), 439–449 (2022).
Elli, S. et al. Extended subcutaneous route technique: A quick subcutaneous tunnelling technique for PICC insertion. J. Vasc Access. 18(3), 269–272 (2017).
Xiao, M. F. et al. Subcutaneous tunneling technique to improve outcomes for patients undergoing chemotherapy with peripherally inserted central catheters: A randomized controlled trial. J. Int. Med. Res. 49(4), 3000605211004517 (2021).
Acknowledgements
Not applicable.
Funding
This work was supported by Sponsored by National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital & Shenzhen Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Shenzhen (E010421001) and supported by Shenzhen High-level Hospital Construction Fund.
Author information
Authors and Affiliations
Contributions
Siqin Li , Hong Lu and Yanting Ning conceived and designed the study. Siqin Li , Hong Lu and Yanting Ning conducted the study. Shanquan Li and Yazhi Peng contributed to data acquisition. Hui Guo, Tudi Yi and Mengling Wu analyzed the data. Wei Tang, Yong Gao and Xiaohua Fan interpreted the data. Siqin Li , Hong Lu and Yanting Ning edited the manuscript draft. Siqin Li , Hong Lu and Yanting Ning reviewed and edited the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study complied with the Declaration of Helsinki and was approved by the ethics committee of Shenzhen Hospital, Tumor Hospital, Chinese Academy of Medical Sciences (Approval No. 2020-47). The included patients and their families signed the informed consent form.
Consent to participate
This study was approved by the Ethics Committee of our hospital, and all patients and their families provided signed informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, S., Lu, H., Li, S. et al. Impact of subcutaneous tunnel length on infection risk in tunneled PICCs: a study in cancer patient. Sci Rep 15, 5430 (2025). https://doi.org/10.1038/s41598-024-82430-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-82430-7
