
Abstract
The burdensome nature of managing type 1 diabetes (T1D) can influence psychological well-being and reduce quality of life (QoL). This pilot study aims to develop and validate a new questionnaire identifying factors impacting the QoL of Australian adults with T1D. Questionnaire development included literature review, pre-testing, semi-structured interviews, expert evaluation, and pilot testing. Questionnaire validation involved an exploratory factor analysis (EFA) to identify the initial factor structure. Confirmatory factor analysis (CFA) determined ___domain validity. Further statistical analysis included convergent, relative, predictive validity, and reliability. The initial questionnaire had 28-items relating to physical, psychological, social, and dietary well-being. CFA revealed ‘psychological’ and ‘social’ items underpinned the four questionnaire domains. The four domains identified were: (1) ‘Coping and Adjusting’ (4-items), (2) ‘Fear and Worry’ (4-items), (3) ‘Loss and Grief’ (3-items), and (4) ‘Social Impact’ (4-items). Significant correlations were revealed between ‘Coping and Adjusting’ and HbA1c (rs = − 0.44, p < 0.01) and ‘Social Impact’ and HbA1c (rs = 0.13, p < 0.01) respectively. Acceptable convergent validity and reliability (test–retest, internal consistency) was observed in all domains. Our study concludes that dietary well-being does not independently impact QoL but is interwoven with psychological factors.
Similar content being viewed by others

Introduction
Destruction of pancreatic beta cells leads to an absolute insulin deficiency resulting in type 1 diabetes (T1D)1. Nine million people worldwide live with T1D, with around 17% under 20 years of age2. In 2024, approximately 141,000 Australians were reported to be living with T1D3. T1D requires constant self-management including frequent monitoring of blood glucose levels (BGLs), daily administration of insulin, meal planning, and physical activity to minimise complications4,5. Continuous self-management and risk of complications may affect psychological well-being, leading to a reduced quality of life (QoL)5,6,7.
To-date, there is no commonly accepted definition of QoL. According to the World Health Organisation QoL is defined as:
“….an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns. It is a broad ranging concept affected in a complex way by the person’s physical health, psychological state, personal beliefs, social relationships, and their relationship to salient features of their environment”8.
In Australia, 41% of adults (≥ 18 years) living with T1D experience diabetes-related psychological issues resulting in suboptimal glycaemia and a reduced QoL9. For Australian adults living with T1D, QoL is influenced by their ability to effectively manage the condition while balancing physical health, psychological well-being, and social participation5,10. Key factors influencing their QoL include glycaemic control, diabetes-related complications (such as cardiovascular disease, retinopathy, nephropathy, and neuropathy), access to healthcare and support, and psychological factors like stress and diabetes distress5,10. Additionally, lifestyle aspects such as dietary well-being, physical activity, financial status, and workplace or social acceptance play critical roles5,11.
Within Australia’s healthcare system, access to diabetes care, technology (e.g., insulin pumps and continuous glucose monitoring), and psychological support can significantly impact QoL10,12. Individuals who receive adequate medical support, education, and community-based assistance often report higher QoL compared to those facing barriers such as financial constraints or healthcare accessibility issues10,12.
Furthermore, nutrition therapy is considered the cornerstone of diabetes management13. Carbohydrate counting is a fundamental skill specifically used by those with T1D in Australia14. Evidence suggests that dietary management using carbohydrate counting can improve both glycaemic control and QoL through increased dietary satisfaction and flexibility15. A meta-analysis of six randomised trials (n = 599) across the UK and Europe, which included both men and women aged 24–51 years with T1D, found that using carbohydrate counting as a dietary strategy did not result in a significant improvement in the QoL for adults with T1D14. However, the QoL questionnaires used in each of the included studies were not specific to T1D adults and lacked a diet and carbohydrate counting skills focus14. Additionally, the dietary aspect of diabetes can be challenging for both patients and clinicians to manage16. Therefore, developing a questionnaire that includes a specific dietary well-being ___domain may provide insight into the effect of diet on QoL. To date, there is no standardised questionnaire to assess the impact of T1D on QoL17. Numerous questionnaires have been developed that include a mixture of dependant variables to assess the influence of all types of diabetes on QoL17. These measures have been developed to better understand how a new intervention, treatment, or clinical practice may affect the QoL of patients living with diabetes18. To our knowledge, there are only two validated T1D specific QoL questionnaires namely, the Diabetes Specific Quality of Life Scale (DSQoLS)4 and the ViDa1 (Vi = of life, Da = of diabetes, 1 = diabetes type 1)5. Firstly, the DSQoLS, developed over 27 years ago, was validated among 657 T1D German adults (42% females, aged 36 ± 11 years) and addresses ‘dietary restriction’ as an aspect related to dietary well-being4. Secondly, the ViDa1 was a cross-sectional study that included 578 Spanish adults with T1D (42% females, aged 35.2 ± 11.9 years) and addressed dietary well-being through aspects such as ‘diet freedom’, ‘diet flexibility’, and ‘carbohydrate counting skills’5. The DSQoLS4 and ViDa15 while reliable and valid, were unsuitable for our study as they lack comprehensive coverage of dietary well-being aspects like flexibility, freedom, and carbohydrate-counting skills15,19, critical to evaluating QoL in adults with T1D. Developed in European contexts, these tools are less relevant to Australia’s unique challenges, such as cultural diversity, Australia’s hot climate, and distinct lifestyle, along with differences in healthcare systems, further limit their applicability20,21,22,23. These tools also fail to integrate physical, psychological, social, and dietary well-being domains holistically, falling short of the broad scope of our study priorities. Additionally, neither questionnaire has been validated for the Australian T1D population, particularly regarding dietary well-being. Finally, as both were originally validated in German or Spanish, their psychometric properties in English cannot be assumed to translate well, which limits their reliability for exclusive use in our research24,25. To evaluate the QoL of individuals with T1D in Australia, these two questionnaires have been adapted to meet this study aims which are to: (1) Develop and pilot a questionnaire incorporating physical, psychological, social, and dietary well-being items relevant to the QoL of adults living with T1D and (2) Validate the questionnaire to determine the QoL domains that impact Australian T1D adults, and in particular if dietary well-being is one of these domains.
Methods
Study design
An exploratory sequential mixed methods, cross-sectional study with a follow-up component for validation purposes was conducted, adhering to the COSMIN (COnsensus-based Standards for the selection of health Measurement INstruments) reporting guidelines26. This study consisted of two phases: phase one involved questionnaire development (literature search/review, pre-testing, semi-structured interviews, expert evaluation, and pilot testing), and phase two focused on questionnaire validation. This study was approved by the Gold Coast Hospital and Health Service Human Research Ethics Committee (HREC) (HREC/2019/QGC/54049) and the University of Canberra (UC) Human Research Ethics Committee (HREC/2019/UC/2223) and complied with the Declaration of Helsinki.
Study population and participant recruitment
Study participants were eligible to participate if they were aged ≥ 18 years, living with T1D, and had been diagnosed with T1D for ≥ 1 year. Ineligible participants included people living with other types of diabetes; people who administer insulin using a continuous subcutaneous insulin infusion; those living with a known food allergy; those with a history of an eating disorder; those with a BMI < 18.5 kg/m2, those who are pregnant or planning to conceive; those taking prescription medications, such as phentermine or corticosteroids; individuals with an active medical problem, such as a recent myocardial infarction, stroke or peripheral revascularisation (within 3-months), active treatment of diabetic retinopathy, or recent serious infection (requiring in-hospital treatment or prolonged antibiotic therapy), that may hinder their ability to take part or may potentially affect study outcomes; those for whom written materials may be unsuitable (e.g., vision-impaired or illiterate individuals); those unable to understand English; and those who fail to sign the participant consent form.
Based on previous evidence, a sample size of 25–30 was deemed adequate to undertake questionnaire pre-testing27,28. Following this step, the participant-to-item ratio method was used to calculate the required sample size for pilot testing29. Anthoine et al. (2014) recommended recruiting 5–20 participants per item for psychometric validation studies. In this study, we adopted a participant-to-item ratio of 13:1, derived from rounding a mean ratio of 12.5, resulting in a target sample size of 364 participants. This approach aligns with recommended practices for determining sample sizes when performing factor analysis in the development of newly-created patient-reported outcome measures29,30. Our chosen ratio ensures an acceptable sample size, with participants equalling 13 times the number of items, consistent with 90% of studies using sample sizes of ≥ 100 participants29.
Participant recruitment used convenience-based snowball sampling at a Southeast Queensland university hospital diabetes outpatient clinic from September 2019 to December 2020. Recruitment approaches included social media, hospital waiting area advertisements, and verbal invitations during outpatient appointments. All consenting participants received via email an internet hyperlink to complete the online study consent form, the questionnaire, and provide sociodemographic and clinical details.
Phase one: questionnaire development
Item generation
Literature review
Electronic databases and publication reference lists were explored to identify existing validated T1D QoL questionnaires for use in this study. This literature search yielded 644 records. Following removal of duplicates, 345 article title and abstracts were screened against the eligibility criteria. As a result, 16 questionnaires were eligible for full text review. Of these, two questionnaires were identified as relevant for our study, the DSQoLS4 and ViDa15. Permission to use these questionnaires was sought from the authors through an email request.
One author approved while the other author did not respond after several emails4,5. Supplement 1. provides details on the study’s Population, Intervention, Comparison, Outcomes (PICO) framework, which was used to define the research question as well as the inclusion and exclusion criteria for questionnaire selection. Additionally, it details the systematic search strategy, including key terms or words used and details on the databases searched and the number of articles identified in each. Supplement 2. presents a PRISMA flowchart illustrating the reduction of articles from 644 to 2.
Content and face validity assessment by diabetes experts
The principal researcher [Janine Paul (JP)] reviewed the DSQoLS4 and ViDa15 for content and face validity. Although neither questionnaire fully aligned with our study’s aims, certain items were deemed relevant. Accordingly, seven items from the DSQoLS4, and 16 from the ViDa15 were selected to form a 23-item questionnaire, covering physical, psychological, social, and dietary well-being to ensure relevance to the QoL of adults living with T1D. Content and face validation was then undertaken by a panel of six diabetes experts from the disciplines of dietetics, exercise physiology, nursing, endocrinology, and psychology. All independently assessed whether the 23-items selected from DSQoLS4, and ViDa15 aligned with the study’s aims. One of the experts contributed to the questionnaire development by providing both clinical and lived experience of T1D. All experts agreed on the relevance of these items and identified five additional items not covered in the existing questionnaires, deeming them relevant to our study population. These new items focused on diabetes management equipment i.e., insulin pumps, continuous glucose monitoring, and blood glucose self-management, resulting in a 28-item questionnaire. Inter-rater reliability was evaluated using Gwet’s AC131. The values are interpreted as follows: < 0.00 no agreement, 0.00–0.20 poor, 0.21–0.40 fair, 0.41–0.60 moderate, 0.61–0.80 substantial, and 0.81–1.00 perfect agreement31,32.
Participant pre-testing and content and face validity
Content and face validity was further undertaken by a group of adults living with T1D. Semi-structured interviews were undertaken by JP to obtain participant perspectives (n = 32) of the online questionnaire including length of time to complete, ease of use, and their understanding of its individual items. An opportunity to give additional feedback was provided at this point. Supplement 3. provides the questions used during this process. Interviews were audio-recorded and transcribed verbatim. Codes were identified from the transcriptions by JP and another research team member independently [David Irvine (DI)] then clustered into themes. Participants privacy was protected by assigning pseudonyms, such as ‘Participant 1’, ‘Participant 2’ etc33. Our questionnaire used a 10-point Likert scale (1 = very strongly disagree to 10 = very strongly agree) because existing literature indicates that scales with a greater number of points reduce information loss in data28,34,35. Additionally, a 10-point rating is easy to understand which may enhance the accuracy of the data collected28,34,35.
Pilot testing
A pilot test was conducted to collect data to evaluate the psychometric properties of the 28-item questionnaire. This questionnaire was administered twice, 14-days apart, following recommendations from previous validation studies regarding the ideal timeframe between assessments36. During the second administration, the Diabetes Quality of Life (DQoL)37 and Problem Areas in Diabetes-20 (PAID-20) scales38 were also completed so that relative validity analysis could be undertaken. Participants included in the pre-testing/semi-structured interviews were excluded from pilot testing to reduce potential bias as they would have had prior knowledge of the questions and to ensure the integrity of the validity and reliability analysis39.
Phase two: questionnaire validation
All psychometric validation tests in this study are based on well-established methods for questionnaire validation, previously applied in research4,5,28. Supplement 4. summarises the reliability and validity tests conducted, detailing each test’s purpose and the criteria used for interpretation in this study.
Descriptive statistics
Descriptive statistics, such as means ± SDs or percentages (%), were used to describe sociodemographic and clinical characteristics of participants.
Construct validity
To examine construct validity exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were performed4,5,28. EFA, using maximum likelihood estimation and varimax rotation, was conducted on the completed dataset to identify potential domains among the 28 items based on four QoL domains: physical, psychological, social, and dietary well-being. Sampling adequacy was calculated using the Bartlett sphericity test and the Kaiser–Meyer–Olkin (KMO) index40,41. Statistical analysis was performed using SPSS (version 29)42.
The original 10-point Likert scale exhibited a non-parametric distribution, limiting its suitability for statistical analysis35,43. To address this, responses were condensed into a 7-point scale, ensuring a more balanced distribution and improved interpretability. The modification preserved key distinctions while reducing extreme response bias, ultimately enhancing the reliability and robustness of the dataset35,43. Furthermore, given that 15% of the dataset had missing values, which could introduce statistical bias, mean imputation was employed to maintain consistency and comparability in participant responses44,45,46.
Following this, EFA was conducted to refine factor structure and enhance interpretability by maximising variance in square loadings across variables41. Initially, six domains were identified through EFA. However, Domain 5, comprised of three items (two dietary well-being and one physical well-being), exhibited poor model fit indices, while Domain 6 contained only one dietary well-being item. Due to these limitations, Domains 5 and 6 were eliminated, resulting in four domains to progress to CFA.
CFA with varimax rotation, was subsequently undertaken using SPSS AMOS (version 29) on the completed dataset (n = 474)47 to evaluate model fit, applying goodness-of-fit indices such as CMIN/DF (χ2/df: 1.0–2.0), Tucker-Lewis index (> 0.90), Comparative Fit Index (> 0.90), and Root Mean Squared Error Approximation (≤ 0.05). The following model fit indices guidelines were considered as sufficient: CFI > 0.90; TFI > 0.90 RMSEA ≤ 0.0548,49,50,51. If RMSEA lower end of the 90% confidence interval (LO90) was equal to zero, then the test of very good fit was supported49,50,51,52,53,54. Model fit was considered acceptable if the majority of goodness-of-fit indices met the ‘acceptable’ cut-off criteria49,50,51,52,53,54. Furthermore, items contributing substantially to a given ___domain were selected based on factor loadings > 0.4055, leading to the removal of nine items during validation. Supplement 5. provides details on all 28-items from the EFA, specifying those retained or removed along with the rationale for each decision.
Convergent validity
Convergent validity was determined from ___domain loadings and calculating both the Average Variance Extraction (AVE) and Composite Reliability (CR) for each ___domain56. AVE ≥ 0.50 reflects acceptable convergent validity, meaning that the latent variable explains more than half of its indicators’ variance57. CR > 0.70 indicates the acceptable degree to which the factor indicators reveal the latent variable56,58.
Relative validity
Item analysis was conducted to evaluate relative validity, as the domains of the selected questionnaires did not align well with the newly formed domains, a method applied in previous studies28,59,60. Our questionnaire was compared with the DQoL37 and PAID-2038 to assess item similarity. Both questionnaires were selected for their rigorous development and validation, making them reliable and accurate tools to assess QoL in individuals living with T1D61,62. They are also commonly used in diabetes research to validate new questionnaires5,63,64. A two-tailed Spearman’s analysis was performed for non-parametric data due to non-normal distribution. Furthermore, to comprehensively evaluate relative validity, the Bland–Altman method was employed to assess systematic bias, with limits of agreement set at ± 2SD from the mean difference65,66. Additionally, linear regression analysis was conducted to determine if the slope of the mean bias (b1) significantly deviated from zero65,66.
Predictive validity
Predictive validity was calculated using a two-tailed Spearman’s correlation (rs) by aligning mean scores of the newly developed questionnaire domains with participants most recent HbA1c (recorded in the past 3 months). Only correlations with p < 0.01 were considered significant. The most recent HbA1c test provides insight into the participants average BGL over the past 2–3 months. This time period is considered a valuable indicator of an individuals’ glycaemic control67. This analysis may help understand the relationship between HbA1c and the newly formed domains to guide diabetes management5,68.
Internal consistency
Internal consistency was measured for each ___domain of the complete dataset (n = 474) using Cronbach’s alpha coefficient. Coefficients above 0.70 were acceptable, 0.80 (good), and 0.90 (excellent)69.
Test re-test reliability
Test re-test reliability was done by administrating our questionnaire twice, with a 14-day interval. The Intraclass Correlation Coefficient (ICC) was calculated36,70. Domains with an ICC below 0.50 indicate poor reliability, between 0.50 and 0.75 moderate reliability, between 0.75 and 0.90 good reliability, and any value above 0.90 indicates excellent reliability71.
Mean scores
The mean scale scores ± SDs of each new ___domain was calculated using the complete dataset. The higher the score, the more closely in line participants were with the new ___domain.
Results
Phase 1: questionnaire development
Item generation
Literature review outcomes
The literature review identified two potential questionnaires for use in this study. While neither was entirely suitable, both contained relevant items related to physical, psychological, social, and dietary well-being, which were adapted to create a 23-item questionnaire. Discussions with six diabetes experts revealed gaps in this questionnaire, leading to the addition of five new items. This resulted in a finalised 28-item questionnaire for pre-testing. Supplement 6. details the adaptations, additions, inclusions, and exclusions of questionnaire items, including the reasons for each decision. Supplement 7. serves as comparative summary of the DSQoLS4, ViDa15, and our questionnaire highlighting the differences. A concluding summary highlights why our questionnaire is unique and suitable option for assessing QoL in Australian individuals with T1D compared to existing DSQoLS4 and ViDa15. Furthermore, Supplement 8. provides the 28-item questionnaire completed by participants (n = 474).
Content and face validity
Inter-rater reliability using Gwet’s AC1 showed almost perfect agreement among the six diabetes experts on the 28-item questionnaire [Gwet’s AC1 = 0.95 (95% CI 0.88–1.00), p < 0.001]. Following expert validation, pre-testing was conducted among 32 participants whose sociodemographic and clinical characteristics are reported in Table 1.
Pre-testing, pilot testing, and validation participants
Pre-testing included 32 participants, while the pilot testing phase was conducted with 474 participants. The validation phase also included 474 participants, all of whom were incorporated into the validation analyses, encompassing EFA, CFA, internal consistency assessment, convergent validity evaluation, predictive validity testing, and mean scores evaluation. For the test–retest reliability and relative validity testing, only 100 participants were included, as the remaining 347 opted not to provide data for these specific tests. Table 1 presents the sociodemographic and clinical characteristics of participants from each phase.
Figure 1. shows the number of participants included for each study phase, and those excluded and the reasons for their exclusion74.

Flow diagram for the number of participants for each study phase. CFA Confirmatory factor analysis, EFA Exploratory factor analysis.
In addition, a flowchart illustrating the process of questionnaire development and validation is presented in Fig. 2.

Phase two: questionnaire validation
Construct validity
Sampling adequacy was confirmed with a Kaiser–Meyer–Olkin (KMO) value of 0.88, classified as excellent (≤ 0.50 poor to ≥ 0.90 excellent)41. Additionally, Bartlett’s sphericity test (X2 = 2318.97; df = 105; p < 0.001) supported the appropriateness of factor analysis, demonstrating the suitability of the dataset for further examination40. Fit indices for the four ___domain model was: CMIN/DF = 2.49, GFI = 0.94, TLI = 0.93, CFI = 0.94, RMSEA = 0.056 (CI 90% 0.04–0.06). Based on these values, the sample demonstrated an overall acceptable goodness of fit supporting a four-___domain model consisting of 15-items. The domains are as follows: (1) ‘Coping and Adjusting’ (4-items), (2) ‘Fear and Worry’ (4-items), (3) ‘Loss and Grief’ (3-items), and (4) ‘Social Impact’ (4-items). The four domains and corresponding 15-items are detailed in Supplement 9.
Convergent validity
Convergent validity was measured using the complete dataset (n = 474). The presence of convergent validity was confirmed using composite reliability (CR) and the average variance extracted (AVE). ‘Coping and Adjusting’ showed good convergent validity (AVE 0.52, CR 0.81). Acceptable convergent validity was observed for ‘Fear and Worry’ (AVE 0.45, CR 0.70), ‘Loss and Grief’ (AVE 0.46, CR 71), and ‘Social Impact’ (AVE 0.46, CR 0.77) (Table 2).
CFA revealed the items which converged onto a ___domain with loadings > 0.40 indicating convergent validity as well as discriminant validity. In addition, further analysis to confirm convergent and discriminant validity was undertaken via a series of Chi-square difference tests for each pair of domains in the model75. The analysis showed that no pairs of domains would satisfy one-factor model over a two-factor model confirming convergent and discriminant validity of each ___domain (Supplement 10). The minimum number of items for a ___domain retained was, ≥ 3-items thereby satisfying the criteria for ___domain validity76.
Relative validity
Spearman correlations revealed no significant relationships between the items analysed from the DQoL and PAID-20 scales (Table 3). Relative validity (n = 100) was deemed acceptable, as the mean scores for participants fell within the 95% limits of agreement, as assessed using the Bland–Altman method. The fitted regression line for item 12 of the PAID-20 versus item 12 of the Australian T1D QoL questionnaire was non-significant, indicating no systematic bias between these items (Table 3). However, significant results were observed for the regression lines between item four of the PAID-20 and item 18 of the Australian T1D QoL questionnaire, as well as between item 10 of the DQoL and item 12 of the Australian T1D QoL questionnaire, suggesting systematic bias in these comparisons (Table 3).
Predictive validity
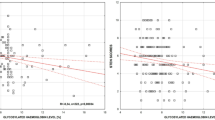
Predictive validity was measured using the complete dataset (n = 474). Our newly developed questionnaire mean scores of ‘Coping and Adjusting’ and ‘Social Impact’ were significantly correlated with participants most recent HbA1c (i.e., within the past 3 month) (rs = − 0.44, p < 0.01 and rs = 0.13, p < 0.01) respectively. ‘Fear and Worry’ and ‘Loss and Grief’ showed no significant correlation with participants most recent HbA1c (rs = 0.09, p = 0.06 and rs = 0.05, p = 0.25) respectively (Table 2).
Internal consistency
Internal consistency was measured for each ___domain of the complete dataset (n = 474). Internal consistency of all the newly developed domains reported good internal consistency (Cronbach’s alpha ≥ 0.70) (Table 2).
Test–retest reliability
Test–retest reliability (n = 100) of ‘Coping and Adjusting’ (ICC = 0.76) and ‘Social Impact’ (ICC = 0.75) showed good test–retest reliability. ‘Fear and Worry’ (ICC = 0.70) and ‘Loss and Grief’ (ICC = 0.72) showed moderate test–retest reliability (Table 2).
Mean scores
Mean scores (n = 474) for each ___domain are reported in Table 2. The higher the score indicated higher agreement to new ___domain.
Discussion
This is the first Australian study to explore dietary well-being as a ___domain of QoL in adults with T1D. It describes the development and pilot validation of a new questionnaire identifying the factors impacting QoL in this cohort. The final T1D QoL questionnaire consisted of 15-items applicable to Australian adults living with T1D. CFA revealed four domains: three ‘psychologically driven’ (1) ‘Coping and Adjusting’, (2) ‘Fear and Worry’, and (3) ‘Loss and Grief’) and one ‘social-driven’ (4) ‘Social Impact’. Each ___domain showed acceptable reliability and validity, with Cronbach’s alpha ≥ 0.70 and acceptable test–retest reliability for domains such as ‘Coping and Adjusting’ (ICC = 0.76) and ‘Social Impact’ (ICC = 0.75).
Previous evidence suggests a connection between diabetes and psychological well-being, impacting self-care behaviours including dietary management and glycaemia4,5,68,77,78. This can affect the risk of diabetes complications, either improving or hampering QoL 4,5,68,77,78. In our study, dietary well-being items revealed multicollinearity with specific ‘psychologically driven’ domains. This might be associated with changes in T1D dietary strategies that our participants may have experienced over the years, such as transitioning from a strict, prescribed regimen to a more patient-oriented, flexible approach. Literature suggests that strict diets can negatively impact psychological well-being and QoL79. A flexible dietary approach, like carbohydrate counting, can positively impact psychological well-being and QoL15. This was demonstrated in a cross-sectional study that included 161 English adults (56% female, aged 40.0 ± 9.0 years), with a diabetes duration of 16.6 ± 9.6 years, and HbA1c of 9.4% ± 1.2, found improved dietary freedom, glycaemic control, treatment satisfaction, and QoL15.
In Australia, a patient-centred, individualised dietary approach is the ‘gold standard’ for individuals with T1D along with carbohydrate counting. The latter can lead to greater dietary freedom and flexibility, supported by level 1 evidence15,80,81. In our study, 86% of pilot testing participants reported using carbohydrate counting, suggesting they experience dietary freedom and flexibility, resulting in a positive relationship with their diet. Our research indicated a negative inverse correlation between HbA1c levels and ‘Coping and Adjusting’ (rs = − 0.44, p < 0.01). However, a positive association between HbA1c and ‘Fear and Worry’ (rs = 0.09, p = 0.06) and ‘Loss and Grief’ (rs = 0.05, p = 0.25) was identified. Both these domains contained dietary well-being related items, highlighting the necessity of evaluating QoL in a clinical setting rather than solely focusing on biomedical markers when formulating treatment strategies4,5,17.
Moreover, T1D can significantly impact physical well-being in the form of cardiovascular disease, nephropathy, neuropathy, retinopathy, and hypoglycaemia, resulting in a lower QoL82. After CFA, our questionnaire did not include a physical well-being ___domain. In addition, no physical well-being items were interwoven with any of the newly developed ‘psychologically driven’ domains of our questionnaire. Conversely, a Spanish cross-sectional study (n = 578, 42% female, aged 35.2 ± 11.9 years), with diabetes duration of 18.0 ± 10 years, and a HbA1c of 7.9% ± 1.3) concluded that those with chronic complications experienced poorer glycaemic control, reduced psychological well-being, increased worry about the future, and a lower QoL5.
This connection was not revealed in our study, possibly because over 67% of participants (n = 474 adults, 73% female, aged 42 ± 14.7 years), with diabetes duration of 21.8 ± 14.5 years, and a HbA1c of 7.5% ± 1.4 reported no chronic diabetes complications. The absence of a direct connection to physical well-being may partly result from participant bias, despite the questionnaire’s rigorous development involving diabetes experts and participants. Ideally, both self-reported and clinician-validated assessments would enhance accuracy, but resource and sample size constraints made their inclusion unfeasible in our pilot study. Future research with greater resources could integrate these assessments to improve the evaluation of physical well-being and reduce potential biases.
Furthermore, Australia’s rigorous approach to managing T1D has contributed to positive outcomes, supported by a universal healthcare system, Medicare, which ensures equitable access to essential diabetes services83. The National Diabetes Services Scheme further enhances care with subsidies for diabetes-related products and educational resources84. Strong diabetes education programs and initiatives, such as those offered by Diabetes Australia, promote early diagnosis, and empower individuals to manage their condition effectively. These efforts have improved awareness, reduced complications, and contributed to better QoL for individuals with T1D85,86,87.
Social well-being is linked to the perceived quality of an individual’s relationships88. Positive relationships with family and friends provide essential emotional support, while a lack of support can negatively impact social well-being, leading to feelings of isolation and loneliness88,89,90. This can hinder self-care practices and diabetes health outcomes88,89,90. Furthermore, Pérez-Fernandez et al. (2023) conducted a systematic review of 12 studies, with 10 of the 12 investigating the association between QoL and HbA1c. The authors concluded that individuals with T1D who experience a lack of social support have a reduced QoL and poorer HbA1c levels. Our study found a significant positive correlation with HbA1c and ‘Social Impact’ (rs = 0.13, p < 0.01), consistent with the literature68,91. Given these findings, developing positive social connections and receiving support is important for improving QoL91.
Patients with T1D may benefit from psychological support from diagnosis and throughout their lifespan due to the burdensome nature of managing this disease92. Our findings reinforce the importance of integrating psychosocial support as part of diabetes care to improve glycaemia, self-care practices, dietary management, psychological well-being, reduce complications, and improve QoL77,78,93,94,95.
Our study has several strengths. Firstly, this is the first Australian study to preliminarily explore dietary well-being as a ___domain in adults with T1D. The final T1D QoL questionnaire consisted of 15-items applicable to Australian adults with T1D. Secondly, it reveals that dietary well-being is not an independent factor contributing to QoL of Australian adults with T1D. Instead, dietary well-being is interwoven with psychological well-being, as indicated by the multicollinearity observed between dietary well-being items and the ‘psychologically driven’ domains. Thirdly, the questionnaire had an acceptable fit criterion, with CFA results showing fit indices of CMIN/DF = 2.49, GFI = 0.94, TLI = 0.93, CFI = 0.94, and RMSEA = 0.056 (CI 90% 0.04–0.06). Fourthly, the robustness of the questionnaire was evident as each ___domain demonstrated adequate results for validity and reliability measures. The questionnaire has good internal consistency, with Cronbach’s alpha ≥ 0.70 for all domains, indicating homogeneity of items within the domains. Each ___domain consists of ≥ 3-items, which is recommended for good psychometric properties76. Reliability results indicate that this questionnaire is effective for assessing changes in QoL over time, as demonstrated by the test–retest reliability of ‘Coping and Adjusting’ (ICC = 0.76) and ‘Social Impact’ (ICC = 0.75), which showed good reliability. Finally, our findings highlight the importance of comprehensive psychological care, likely leading to improved health outcomes, dietary management, and QoL of Australian adults with T1D. The significant correlations between HbA1c levels and the domains of ‘Coping and Adjusting’ (rs = − 0.44, p < 0.01) and ‘Social Impact’ (rs = 0.13, p < 0.01) underscore this necessity.
However, the study has limitations. The small sample size and convenience-based sampling limit both causal inferences and generalisability. The participant demographics, including gender distribution (73% female and 27% male) and ethnicity (79.5% identifying as Australian and 9.5% as British), reflect the voluntary nature of participation, which inherently limits balanced representation. While Australia’s multicultural nature72 means that those identifying as Australian may have diverse ethnic backgrounds (e.g., first, second, or third-generation British, European, or other backgrounds), this does not fully mitigate the potential bias in representation. As a result, generalisability may be affected, and broader recruitment in future research would be necessary to enhance representativeness and ensure a more inclusive sample.
Furthermore, the questionnaire is specific to the Australian T1D population and is not accessible to those who are vision or intellectually impaired, speak languages other than English, or have other types of diabetes. While these limitations may affect generalisability, the sample still provides valuable insights, and future research could address these concerns through broader recruitment strategies and enhanced accessibility.
The questionnaire’s brevity makes it useful for developing treatment strategies in busy clinical settings. The correlations observed between HbA1c levels and domains such as ‘Coping and Adjusting’ (rs = − 0.44, p < 0.01) and ‘Social Impact’ (rs = 0.13, p < 0.01) highlight the potential clinical relevance of this questionnaire. Nevertheless, several QoL questionnaires have been developed and validated for individuals living with T2D, such as the Audit of Diabetes-Dependent Quality of Life (ADDQoL), Diabetes Health Profile (DHP), and the EuroQol 5-Dimension (EQ-5D) questionnaire, which assess various domains of QoL and have been widely used in clinical and research settings96,97,98.
Conclusions
This new questionnaire for examining QoL in Australian adults living with T1D includes four domains: three with a ‘psychologically driven’ theme (1) ‘Coping and Adjusting’, (2) ‘Fear and Worry’, and (3) ‘Loss and Grief’, and one with a ‘socially driven’ theme (4) ‘Social Impact’. Dietary well-being items were interwoven with the ‘psychological driven’ domains. This questionnaire has acceptable psychometric properties and test–retest reliability. This questionnaire may help better understand QoL in Australian adults living with T1D. Our findings highlight the importance of comprehensive psychological support to enhance QoL associated with diabetes management and outcomes, as reflected by the significant correlations between HbA1c levels and the identified domains.
Data availability
Data is provided within the manuscript and supplementary information.
Abbreviations
- AVE:
-
Average variance extraction
- BGL:
-
Blood glucose level
- BMI:
-
Body mass index
- CFA:
-
Confirmatory factor analysis
- CFI:
-
Comparative fit index
- COSMIN :
-
COnsensus-based Standards for the selection of health Measurement INstruments
- CR:
-
Composite reliability
- DQOL:
-
Diabetes quality of life
- DSQoLS:
-
Diabetes specific quality of life scale
- EFA:
-
Exploratory factor analysis
- HbA1c:
-
Glycated haemoglobin
- ICC:
-
Intraclass correlation coefficient
- KMO:
-
Kaiser meyer olkin (index)
- PAID-20:
-
Problem areas in diabetes-20
- QoL:
-
Quality of life
- RMSEA:
-
Root mean squared error approximation
- SD:
-
Standard deviation
- T1D:
-
Type 1 diabetes
- T2D:
-
Type 2 diabetes
- TLI:
-
Tucker lewis index
- ViDa1:
-
Vi = of life, Da = of diabetes, 1 = diabetes type 1
References
DiMeglio, L. A., Evans-Molina, C. & Oram, R. A. Type 1 diabetes. Lancet 391, 2449–2462 (2018).
International Diabetes Federation. Type 1 diabetes. International Diabetes Federation https://idf.org/about-diabetes/type-1-diabetes/ (2024).
National Diabetes Service Scheme. Type 1 diabetes. Diabetes Australia https://www.ndss.com.au/wp-content/uploads/Diabetes-Type-1-1.pdf (2024).
Bott, U., Mühlhauser, I., Overmann, H. & Berger, M. Validation of a diabetes-specific quality-of-life scale for patients with type 1 diabetes. Diabet. Care 21, 757–769 (1998).
Alvarado-Martel, D. et al. ViDa1: The development and validation of a new questionnaire for measuring health-related quality of life in patients with type 1 diabetes. Front. Psychol. 8, 904 (2017).
Wagner, V. M., Müller-Godeffroy, E., Von Sengbusch, S., Häger, S. & Thyen, U. Age, metabolic control and type of insulin regime influences health-related quality of life in children and adolescents with type 1 diabetes mellitus. Eur. J. Pediatr. 164, 491–496 (2005).
Saito, I. et al. Impact of diabetes on health-related quality of life in a population study in Japan. Diabet. Res. Clin. Pract. 73, 51–57 (2006).
World Health Organisation. The World Health Organization Quality of Life Assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 41, 1403–1409 (1995).
Shaw, J. & Tanamas, S. Diabetes: The silent pandemic and its impact on Australia. Baker IDI Heart and Diabetes Institute https://www.diabetesaustralia.com.au/wp-content/uploads/Diabetes-the-silent-pandemic-and-its-impact-on-Australia.pdf (2012).
Speight, J., Browne, J. L., Holmes-Truscott, E., Hendrieckx, C. & Pouwer, F. Diabetes MILES-Australia (management and impact for long-term empowerment and success): Methods and sample characteristics of a national survey of the psychological aspects of living with type 1 or type 2 diabetes in Australian adults. BMC Public Health 12, 1–13 (2012).
Paul, J. et al. Low carbohydrate diets, glycaemic control, enablers, and barriers in the management of type 1 diabetes: A mixed methods systematic review. Diabetol. Metabol. Syndr. 16, 261 (2024).
Australian Institute of Health and Welfare. (Canberra 2021).
American Diabetes Association Professional Practice Committee. 5. Facilitating positive health behaviors and well-being to improve health outcomes: standards of care in diabetes-2024. Diabet. Care 47, S77–S110 (2024).
Bell, K. J., Barclay, A. W., Petocz, P., Colagiuri, S. & Brand-Miller, J. C. Efficacy of carbohydrate counting in type 1 diabetes: A systematic review and meta-analysis. Lancet Diabet. Endocrinol. 2, 133–140 (2014).
DAFNE Study Group. Training in flexible, intensive insulin management to enable dietary freedom in people with type 1 diabetes: Dose adjustment for normal eating (DAFNE) randomised controlled trial. BMJ 325, 746 (2002).
Holt, R. I. et al. The management of type 1 diabetes in adults: a consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabet. Care 44, 2589–2625 (2021).
Speight, J., Holmes-Truscott, E., Hendrieckx, C., Skovlund, S. & Cooke, D. Assessing the impact of diabetes on quality of life: What have the past 25 years taught us?. Diabet. Med. 37, 483–492 (2020).
Palamenghi, L., Carlucci, M. M. & Graffigna, G. Measuring the quality of life in diabetic patients: A scoping review. J. Diabet. Res. 2020, 5419298 (2020).
Sindler, D., Kastovska, B., Dostal, T., Cipryan, L. & Elavsky, S. The effects of carbohydrate-restricted diet on psychological outcomes: A systematic review of randomized controlled trials. Nutr. Rev. 82, 228–239 (2023).
Burrow, S. & Ride, K. Review of diabetes among Aboriginal and Torres Strait Islander people. Australian Indigenous Healthinfonet https://healthinfonet.ecu.edu.au/healthinfonet/getContent.php?linkid=590810&title=Review+of+diabetes+among+Aboriginal+and+Torres+Strait+Islander+people (2016).
National Diabetes Services Scheme. Your guide to managing diabetes when it’s hot. https://www.ndss.com.au/news/managing-diabetes-when-its-hot/ (2024).
Australian Institute of Health and Welfare. Measures of health and health care for Australia and similar countries. Australian Government https://www.aihw.gov.au/reports/international-health-data-comparisons (2024).
Tourism Australia. A handy guide to the Australian lifestyle. Tourism Australia https://www.australia.com/en/facts-and-planning/about-australia/the-aussie-way-of-life.html (2025).
Pisimisis, T. Quality of Life of People with Diabetes Mellitus in Greece (University College London, 2014).
Bradley, C. et al. The development of an individualized questionnaire measure of perceived impact of diabetes on quality of life: the ADDQoL. Qual. Life Res. 8, 79–91 (1999).
Gagnier, J. J., Lai, J., Mokkink, L. B. & Terwee, C. B. COSMIN reporting guideline for studies on measurement properties of patient-reported outcome measures. Qual. Life Res. 30, 2197–2218 (2021).
Paul, J., Jani, R., Davoren, P. & Knight-Agarwal, C. Association between a low carbohydrate diet, quality of life, and glycemic control in Australian adults living with type 1 diabetes: Protocol for a mixed methods pilot study. JMIR Res. Protoc. 10, e25085 (2021).
Jani, R. et al. The picky eating questionnaire and child-reported food preference questionnaire: Pilot validation in Australian-Indian mothers and children 7–12 years old. Food. Qual. Prefer. 99, 104584 (2022).
Anthoine, E., Moret, L., Regnault, A., Sébille, V. & Hardouin, J. B. Sample size used to validate a scale: A review of publications on newly-developed patient reported outcomes measures. Health Qual. Life Outcomes 12, 1–10 (2014).
Nathan, Z. The minimum sample size in factor analysis. https://www.encorewiki.org/display/nzhao (2009).
Gwet, K. L. Handbook of Inter-Rater Reliability: The Definitive Guide to Measuring the Extent of Agreement Among Raters (Advanced Analytics, LLC, 2014).
Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 20, 37–46 (1960).
Charmaz, K. Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis (SAGE Publications, 2006).
Wu, H. & Leung, S. O. Can likert scales be treated as interval scales?: A simulation study. J. Soc. Serv. Res. 43, 527–532 (2017).
Leung, S.-O. A comparison of psychometric properties and normality in 4-, 5-, 6-, and 11-point Likert scales. J. Soc. Serv. Res. 37, 412–421 (2011).
Streiner, D. L., Norman, G. R. & Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use 5th edn. (Oxford University Press, 2014).
DCCT Research Group. Reliability and validity of a diabetes quality-of-life measure for the diabetes control and complications trial (DCCT). Diabet. Care 11, 725–732 (1988).
Welch, G. W., Jacobson, A. & Polonsky, W. H. The problem areas in diabetes scale: an evaluation of its clinical utility. Diabet. Care 20, 760–766 (1997).
Edwards, P. Questionnaires in clinical trials: Guidelines for optimal design and administration. Trials 11, 2 (2010).
Bartlett, M. S. A note on the multiplying factors for various chi square approximations. J. R Stat. Soc. Series B. Stat. Methodol. 16, 296–298 (1954).
Kaiser, H. F. The varimax criterion for analytic rotation in factor analysis. Psychometrika 23, 187–200 (1958).
IBM SPSS Statistics for Windows (version 29.0) (IBM Corp, New York, 2022).
Boone, H. N. Jr. & Boone, D. A. Analyzing likert data. J. Ext. 50, 48 (2012).
Bennett, D. A. How can I deal with missing data in my study?. Aust. N. Z. J. Public Health 25, 464–469 (2001).
Dong, Y. & Peng, C. Y. J. Principled missing data methods for researchers. Springerplus 2, 222 (2013).
Schafer, J. L. & Graham, J. W. Missing data: Our view of the state of the art. Psychol. Methods 7, 147–177 (2002).
Amos (version 29.0) (IBM SPSS, New York, 2023).
Bentler, P. M. & Bonett, D. G. Significance tests and goodness of fit in the analysis of covariance structures. Psychol. Bull. 88, 588–606 (1980).
Browne, M. W. & Cudeck, R. Alternative ways of assessing model fit. Sociol. Methods Res. 21, 230–258 (1992).
Steiger, J. H. Structural model evaluation and modification: an interval estimation approach. Multivariate Behav. Res. 25, 173–180 (1990).
Bentler, P. M. EQS Structural Equations Program Manual (Multivariate Software, 1995).
Hu, L. T. & Bentler, P. M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 6, 1–55 (1999).
Tucker, L. R. & Lewis, C. A reliability coefficient for maximum likelihood factor analysis. Psychometrika 38, 1–10 (1973).
Bentler, P. M. Comparative fit indexes in structural models. Psychol. Bull. 107, 238–246 (1990).
Taherdoost, H., Sahibuddin, S. & Jalaliyoon, N. Exploratory factor analysis; concepts and theory. Adv. Pure Appl. Math. 27, 375–382 (2014).
Fornell, C. & Larcker, D. F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 18, 39–50 (1981).
Cheung, G. W., Cooper-Thomas, H. D., Lau, R. S. & Wang, L. C. Reporting reliability, convergent and discriminant validity with structural equation modeling: A review and best-practice recommendations. Asia. Pac. J. Manag. 41, 745–783 (2023).
Hair, J. F., Ringle, C. M. & Sarstedt, M. PLS-SEM: Indeed a silver bullet. J. Mark. Theory Pract. 19, 139–152 (2011).
Saswati, R. Item analysis of reading comprehension test: A study of test scores interpretation. J. Engl. Lang. Teach. 6, 42–49 (2021).
Sekhon, M., Cartwright, M. & Francis, J. J. Development of a theory-informed questionnaire to assess the acceptability of healthcare interventions. BMC Health Serv. Res. 22, 279 (2022).
Association., A. D. PAID-20: Problem Areas in Diabetes Questionnaire. https://professional.diabetes.org/sites/default/files/media/ada_mental_health_toolkit_questionnaires.pdf ( n.d).
Polonsky, W. H. et al. Assessment of diabetes-related distress. Diabet. Care 18, 754–760 (1995).
Shen, W. et al. Development and validation of the diabetes quality of life clinical trial questionnaire. Med. Care 37, AS45–AS66 (1999).
Burroughs, T. E., Desikan, R., Waterman, B. M., Gilin, D. & McGill, J. Development and validation of the diabetes quality of life brief clinical inventory. Diabet. Spectr. 17, 41–49 (2004).
Bland, J. M. & Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 327, 307–310 (1986).
Xuan, W., Williams, K. & Peat, J. K. Health Science Research: A Handbook of Quantitative Methods (Routledge, 2020).
American Diabetes Association Professional Practice Committee. 6. Glycemic goals and hypoglycemia: standards of Care in diabetes: 2024. Diabet. Care 47, S111–S125 (2024).
Pérez-Fernández, A., Fernández-Berrocal, P. & Gutiérrez-Cobo, M. J. The relationship between well-being and HbA1c in adults with type 1 diabetes: A systematic review. J. Diabet. 15, 152–164 (2023).
Terwee, C. B. et al. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 60, 34–42 (2007).
Kennedy, I. Sample size determination in test-retest and Cronbach alpha reliability estimates. Br. J. Contemp. Educ. 2, 17–29 (2022).
Koo, T. K. & Li, M. Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 15, 155–163 (2016).
Australian Bureau of Statistics. Census Quickstats. https://www.abs.gov.au/census/guide-census-data/about-census-tools/quickstats (2022).
Harris, J., McGee, A., Andrews, F., D’Souza, J. & Sproston, K. The national survey of people with diabetes. NHS Patient Surveys. https://www.nhssurveys.org/Filestore/documents/Diabetes_key_findings_rpt.pdf (2007).
Vandenbroucke, J. P. et al. Strengthening the reporting of observational studies in epidemiology (STROBE): Explanation and elaboration. Ann. Intern. Med. 147, 163–194 (2007).
Atuahene-Gima, K. Resolving the capability–rigidity paradox in new product innovation. J. Mark. 69, 61–83 (2005).
Field, A. Discovering Statistics Using IBM SPSS Statistics 5th edn. (SAGE Publications, 2017).
Kalra, S., Jena, B. N. & Yeravdekar, R. Emotional and psychological needs of people with diabetes. Indian J. Endocrinol. Metab. 22, 696–704 (2018).
Resurrección, D. M., Navas-Campaña, D., Gutiérrez-Colosía, M. R., Ibáñez-Alfonso, J. A. & Ruiz-Aranda, D. Psychotherapeutic interventions to improve psychological adjustment in type 1 diabetes: A systematic review. Int. J. Environ. Res. Public Health 18, 10940 (2021).
Laurenzi, A. et al. Effects of carbohydrate counting on glucose control and quality of life over 24 weeks in adult patients with type 1 diabetes on continuous subcutaneous insulin infusion: A randomized, prospective clinical trial (GIOCAR). Diabet. Care 34, 823–827 (2011).
Smart, C. E. et al. ISPAD clinical practice consensus guidelines 2018: Nutritional management in children and adolescents with diabetes. Pediatr. Diabet. 19, 136–154 (2018).
National Health and Medical Research Council. A guide to the development, implementation and evaluation of clinical practice guidelines. NHMRC https://www.nhmrc.gov.au/sites/default/files/images/a-guide-to-the-development-and-evaluation-of-clinical-practice-guidelines.pdf (1998).
Lloyd, C. E. & Orchard, T. J. Physical and psychological well-being in adults with type 1 diabetes. Diabet. Res. Clin. Pract. 44, 9–19 (1999).
Australian Government Department of Health and Aged Care. About Medicare. https://www.health.gov.au/topics/medicare/about (2022).
Australian Government Department of Health and Aged Care. National Diabetes Services Scheme (NDSS). https://www.health.gov.au/our-work/national-diabetes-services-scheme-ndss (2023).
Diabetes Australia. Early diagnosis of T1D. https://www.diabetesaustralia.com.au/issue/supporting-early-diagnosis-type-1-diabetes/ (2025).
Diabetes Australia. Education and events. https://www.diabetesaustralia.com.au/education-and-events/ (2025).
Parliament of Australia. Chapter 4 - Screening, diagnosing and managing diabetes and obesity. https://www.aph.gov.au/Parliamentary_Business/Committees/House/Health_Aged_Care_and_Sport/Inquiry_into_Diabetes/Report/Chapter_4_-_Screening_diagnosing_and_managing_diabetes_and_obesity?form=MG0AV3&form=MG0AV3 (n.d.).
Luo, D., Cai, X., Wang, H., Wang, Y. & Xu, J. The role of peer social relationships in psychological distress and quality of life among adolescents with type 1 diabetes mellitus: A longitudinal study. BMC Psychiatry 24, 270 (2024).
Villaécija, J., Luque, B., Castillo-Mayén, R., Farhane-Medina, N. Z. & Tabernero, C. Influence of family social support and diabetes self-efficacy on the emotional wellbeing of children and adolescents with type 1 diabetes: A longitudinal study. Children 10, 1196 (2023).
Pérez-Fernández, A., Fernández-Berrocal, P. & Gutiérrez-Cobo, M. J. The relationship between emotional intelligence and diabetes management: A systematic review. Front. Psychol. 12, 754362 (2021).
Gredig, D. & Bartelsen-Raemy, A. Diabetes-related stigma affects the quality of life of people living with diabetes mellitus in Switzerland: Implications for healthcare providers. Health Soc. Care. Commun. 25, 1620–1633 (2017).
Chew, B.-H., Shariff-Ghazali, S. & Fernandez, A. Psychological aspects of diabetes care: Effecting behavioral change in patients. World J. Diabet. 5, 796–808 (2014).
Efthymiadis, A., Bourlaki, M. & Bastounis, A. The effectiveness of psychological interventions on mental health and quality of life in people living with type 1 diabetes: A systematic review and meta-analysis. Diabetol. Int. 13, 513–521 (2022).
Young-Hyman, D. et al. Psychosocial care for people with diabetes: A position statement of the American Diabetes Association. Diabet. Care 39, 2126–2140 (2016).
Nicolucci, A. et al. Diabetes attitudes, wishes and needs second study (DAWN2TM): Cross-national benchmarking of diabetes-related psychosocial outcomes for people with diabetes. Diabet. Med. 30, 767–777 (2013).
Bradley, C. The audit of diabetes-dependent quality of life (ADDQoL). Health Psychology Research http://www.healthpsychologyresearch.com/Admin/uploaded/Guidelines/addqol18_userguidelines_rev24jan05a.pdf (2014).
Meadows, K., Abrams, C. & Sandbak, A. Adaptation of the Diabetes Health Profile (DHP-1) for use with patients with type 2 diabetes mellitus: Psychometric evaluation and cross-cultural comparison. Diabet. Med. 17, 572–580 (2000).
Herdman, M. et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 20, 1727–1736 (2011).
Acknowledgements
The authors would like to thank all the patients who participated in the study and David Irvine (credentialled diabetes educator nurse) for assistance with participant recruitment and interview transcription support. Dr Dean Vuksanovic for his psychology expertise, advice, and guidance throughout the questionnaire development and validation process. The Gold Coast University Hospital library staff are acknowledged for their support throughout the study. In addition, Associate Professor Tim Schlub, Associate Professor Mark Jones, and Dr Ian Hughes are gratefully acknowledged for their statistical support and advise at various stages of the study.
Funding
The authors declare that no funds, grants, or other support were received for the submitted work.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and data analysis was performed by JP. Assistance with data analysis and interpretation was provided by M Abu Saleh (MAS). The first draft of the manuscript was written by JP and all authors [Catherine R. Knight-Agarwal (CKA), MAS, Peter Davoren (PD), and Rati Jani (RJ)] commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the Gold Coast Hospital and Health Service (GCHHS) Human Research Ethics Committee (HREC) (HREC/2019/QGC/54049) and the University of Canberra (UC) Human Research Ethics Committee (HREC/2019/UC/2223).
Consent to participate and publish
Written informed consent was obtained from all study participants. Additionally, all participants have given written consent for this manuscript to be submitted for journal publication.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Paul, J., Knight-Agarwal, C.R., Saleh, M.A. et al. Development and validation of a questionnaire to assess quality of life in Australian adults with type 1 diabetes: a pilot psychometric study. Sci Rep 15, 22462 (2025). https://doi.org/10.1038/s41598-025-06420-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-06420-z
