
Abstract
Laryngopharyngeal reflux (LPR) involves the reflux of stomach contents into the upper aerodigestive tract and is often linked to allergic rhinitis (AR), an inflammatory nasal condition. This study investigates the potential association between AR and LPR in Sudanese adults, focusing on individuals with asthma. Analytical, community based cross-sectional study was conducted online (June 11–July 21, 2024) using convenient sampling, which included Sudanese adults aged 18 and older. Validated Arabic versions of the Reflux Symptom Index (RSI) and the Score for Allergic Rhinitis (SFAR) assessed LPR and AR, respectively. Data analysis using SPSS version 26 utilized statistical tests, including univariate analysis and logistic regression, to explore associations. Among our 1,195 participants, a strong positive correlation was found between RSI and SFAR scores (r = 0.595, p < 0.001). Participants with AR were six times more likely to have LPR symptoms (OR = 5.956, p < 0.001). Females and younger adults reported higher rates of both conditions, with family history of allergies, nasal symptoms, and environmental allergen exposure significantly associated with LPR. Asthma, though present in a small subset, did not significantly alter the AR-LPR association. The study highlights a strong association between AR and LPR, particularly in females and younger adults, emphasizing the need for integrated management. Future research should explore asthma’s role in larger cohorts and utilize objective diagnostic tools to establish causality. The findings also stress the importance of increased funding for biomedical research in resource-limited settings like Sudan.
Similar content being viewed by others

Introduction
Laryngopharyngeal reflux (LPR) is the reflux of stomach contents into the upper aerodigestive system without regurgitation or heartburn1. Heartburn and acid regurgitation, especially at night and when lying down, are indications of Gastroesophageal reflux disease2. An endoscopy or pH monitoring can confirm a diagnosis of esophagitis2. The diagnosis of LPR is more intricate and requires both therapeutic strategies and in-depth clinical examination1,3.
Because of its perplexing symptoms, such as hoarseness in voice, throat clearing, and globus pharyngeus, it is difficult to estimate the prevalence of LPR1,2. There are differences between LPR and Gastroesophageal reflux disease (GERD) in terms of diagnosis, therapy, and psychological effects4. Furthermore, the mechanism of LPR is not exclusive to the gastrointestinal tract. Its symptoms can be caused by various factors, including vocal abnormalities, medications, neurogenic conditions, pulmonary issues, smoking, environmental factors, and allergies2.
According to guidelines, people with typical GERD symptoms and no alarm characteristics may benefit from an empirical proton pump inhibitor (PPI) trial2. While an empirical trial of PPIs is feasible for individuals with concurrent esophageal symptoms, upfront ambulatory reflux monitoring is advised for patients with isolated laryngeal symptoms due to the uneven response to empiric PPI therapy in patients with laryngopharyngitis5. It is frustrating that a considerable percentage of patients (30–45%) do not respond well enough to PPI treatment and lifestyle changes3. Notably, according to present recommendations, laryngoscopy alone is insufficient for diagnosing LPR. It is also evaluated using a variety of tests, such as oesophageal manometry, pH, and impedance monitoring to detect non-acidic reflux episodes. More recently, oropharyngeal pepsin testing is also being used to diagnose LPR6.
One of the most prevalent illnesses in the world, allergic rhinitis (AR) is an inflammatory disease that develops in the nasal mucosa as a result of allergen exposure7. Worldwide, the frequency of AR varies from 5 to 22%8. Given their similarities, AR and asthma might be thought of as two equivalent airway illnesses. Several other symptoms are associated with AR, such as rhinorrhea, sneezing, nasal irritation, and nasal congestion or obstruction9.
A limited amount of research has been done that suggests an informal connection between allergic rhinitis and laryngopharyngeal disease, even though patients with asthma present with both of these diseases. Nonetheless, numerous studies have indicated that AR and LPR may be related to one another despite neither having asthma since they share many symptoms related to aerodigestive tract irritation8,10.
Our research aims to explore the potential comorbidity of allergic rhinitis and laryngopharyngeal reflux illness in a general population. We hypothesize that laryngopharyngeal reflux is associated with allergic rhinitis.
Methodology
Study design and participants
An analytic, community-based cross-sectional study was conducted in Sudan between June 11 and July 21, 2024. Participants aged 18 years and older, residing in Sudan, and who completed all items of the Reflux Symptom Index (RSI) questionnaire were included. Recruitment occurred online through various social media apps using targeted posts explaining the study’s purpose.
Sampling
A convenient sampling method was used to collect the data from the community. Data collectors were recruited to send the online form via social media apps. Sample size was calculated using sample size equation for unknown population:
s = sample size. Z = Z score for used confidence interval (95%) = 1.96. P = Probability of the disease = 0.5 (unkonwn). e = margin of error = 0.05. By multiplying the design effect (3x sample size) and adding a non-response rate of 10%, the final sample size is 1268.
Measurements
Data were collected via an online survey, which included demographic information (age, gender, region of residence, income, profession), clinical history items, reflux symptom index (RSI) and score for allergic rhinitis (SFAR). Items to assess the clinical history of the participants included: asthma clinical diagnosis, family history of asthma, history of atopy and their exacerbating factors. Two previously pilotted, validated questionnaires were also administered. The first one was a validated Arabic version of the reflux symptom index (RSI) with cronbach alpha value of 0.728,11, which was employed to assess the likelihood of LPR. The RSI is a self-administered nine-item questionnaire with each item scored on a scale of 0–5, yielding a total score ranging from 0 to 45 points. A cut-off score of 13 or higher suggests possible LPR. The survey also incorporated the Seasonal Allergic Rhinitis (SFAR) tool to evaluate allergic rhinitis symptoms by asking questions about: family history, nose symptoms, eye symptoms and clinical history. SFAR tool aims to determine the prevalence of allergic rhinitis using a cut value of 712 and cronbach alpha of 0.79 (Supplementary file 1). No medical examinations or diagnostic procedures were performed during the study period. The response rate for this survey was 94.2%, based on a total sample size of 1,268 and 1,195 completed responses.
Data analysis
The data were initially collected using Excel and then cleaned using SPSS version 26. Normality test was performed for continuous data, which are: age, reflux symptoms index scale, changes in residency and score for allergic rhinitis, where the Kolmogorov normality test indicates non-normal distribution (P value was <0.001 for all of them), so non-parametric tests were used. Missing value analysis was performed to estimate the missing percentages in all variables which yielded less than 5% in all variables. Then descriptive statistics and frequency tables were used to describe the data. Mann-Whitney test was used to study the differences between age and changes in residency against the reflux symptom index and allergic rhinitis. Chi-squire and Fisher exact tests were used to study the associations between multiple socio-demographic and clinical factors against the reflux symptom index and allergic rhinitis. Spearman’s rho test was used to evaluate the association between allergic rhinitis score and reflux symptom index score. Chi-squire test was also used to study the differences among allergic rhinitis groups and reflux symptoms. Binomial logistic regression was also used to study the factors affecting allergic rhinitis (binary variable), so socio-demographic characteristics with a p-value less than 0.05 and reflux symptoms were selected to enter the model. In all tests p-value of less than 0.05 was indicated as a significant result.
Ehical approval and consent of participants
Ethical approval was obtained from the Ethical Committee of the Ministry of Health, River Nile State. This approval covered all aspects of the study, including participant recruitment, data collection, analysis, publication, and data usage. Informed consent was obtained from all participants before their involvement in the study. All procedures adhered to the principles of the Declaration of Helsinki and complied with relevant guidelines and regulations, including the STROBE guidelines for reporting observational studies.
Results
Socio-demographic characteristics
A sample of 1195 was collected in this study. The median age was 24 ± 7 years. The majority of the participants (63.9%) were females, and more than two-thirds (75.2%) were single. Most of the participants were from: River Nile state (24.7%), Kassala state (17.5%) and North state (15.1%). Almost (83.8%) had a bachelor’s degree, and only 1 participant reported to be illiterate (0.1%). (42.4%) of the participants were from non-medical fields, while the rest were medical field workers from different specialities. More than two-thirds of the participants (67.9%) didn’t work, and only 348 (10.9%) participants indicated family income was insufficient for their needs (Table 1).
Almost quarter of the participants (278,23.3%) reported having positive reflux symptoms indicating LPR symptoms. There was a significant, very low negative association between age and LPR symptoms index scale (r = – 0.90, p-value = 0.002). Females tend to significantly have a higher percentage (26.7%) of LPR symptoms compared to males (17.2%) (p-value<0.001). Moreover, participants who aren’t currently studying in universities reported higher percentages (35.8%) of these symptoms than university students (p-value = 0.042). Marital status, grade, and working status didn’t show any reported significance to LPR (Table 2).
Females tend to significantly report a higher percentage (73.6%) of AR compared to males (26.4%) (p-value < 0.001). Moreover, the highest significant percentage of AR was noticed in medical students (40.5%) (p-value = 0.014). There weren’t any associations between AR and age, marital status, or income (Table 3).
Clinical factors contributing to laryngopharyngeal reflux symptoms
There was a significant difference between patients with asthma and patients without it regarding laryngopharyngeal reflux symptoms, with the highest percentage of asthmatic patients having no LPR symptoms (53.5%) (p-value = 0.001). Having a family history of allergy in the nose, chest, or skin was significantly associated with a higher percentage of LPR symptoms compared to those with no history (29.9% vs. 13.6%) (p-value < 0.001). The highest reported type of allergy in the family was chest and nose allergy for the father (56.5%), skin and chest allergy for the mother (62.5%), and skin, nose, and chest allergy for both sons/daughters and siblings (57.1% for both) (p-value < 0.01) (Table 4).
There was a significant association between having a runny nose, sneezing, nasal congestion, and having LPR symptoms (p-value < 0.001). Participants who had nose problems during most of the year (all seasons of the year) had a significantly higher percentage of LPR symptoms (67.1%) compared to those who had nose problems in one month or some months of the year (p-value < 0.001). The allergy-exacerbating factors significantly associated with LPR symptoms were dust, insects, animals, and pollen (p-value < 0.001 for all). However, participants without allergies to any of these factors reported a higher percentage of no LPR symptoms. Participants with a history of allergy had a significantly higher percentage (38.9%) of laryngopharyngeal reflux symptoms (p-value < 0.001), especially among ones who had a positive test in skin or blood tests for allergy (46.5%) (p-value < 0.001). Moreover, having a skin, nose, or chest allergy diagnosis led to a significantly higher percentage of reflux symptoms (p-value < 0.001) (Table 5).
Association between laryngopharyngeal reflux and allergic rhinitis
Participants with allergic rhinitis were found to have significantly six times more laryngopharyngeal reflux symptoms compared to those without rhinitis (OR = 5.956, 95% CI: 4.439–7.992, p-value < 0.001). Among asthmatics, there was no significant difference in LPR symptoms between those with AR and those without (p-value = 0.191). However, in participants without asthma, the significant association between AR and LPR remained present (OR = 5.797, 95% CI: 4.285–7.841, p-value < 0.001).) (Table 6).
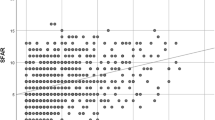
The median score of allergic rhinitis (SFAR) was 5 ± 6. While the median of the laryngopharyngeal reflux symptoms index score (RSI) was 5 ± 12. The correlation matrix was formed between the score of allergic rhinitis (SFAR) and the laryngopharyngeal reflux symptoms index score (RSI). There was a significantly high positive association between allergic rhinitis score and laryngopharyngeal reflux symptoms score (r = 0.595, p-value<0.001). Moreover, a moderate positive association was also reported between the two scales when dividing the sample into asthmatic and non-asthmatic patients (r = 0.50 for asthmatic and 0.59 for non-asthmatic, p-value = 0.001 for asthmatic and < 0.001 for non-asthmatic) (Table 7).
Binomial logistic regression was performed for variables that contribute to allergic rhinitis according to previous univariate analysis. These variables were: gender, faculty, income and laryngopharygeal reflux symptoms. The model has statistically significant results in Omnibus tests (p-value < 0.001) with a Nagelkerke R-squared value of 0.202. Participants with income that is sufficient for basic needs and some additions had significantly 1.6 times less allergic rhinitis compared to those with insufficient income at all (OR = 0.619, C.I = 0.400- 0.956, p-value = 0.031). Moreover, participants with positive laryngopharyngeal reflux symptoms tend to have significantly 5.6 times more allergic rhinitis than ones with negative symptoms (OR = 5.628, C.I = 4.163–7.607, p-value < 0.001) (Table 8).
Discussion
Understanding the complex relationships between allergic rhinitis (AR), laryngopharyngeal reflux (LPR), and asthma is crucial given their high prevalence and impact on quality of life5,13,14. Moreover, patients with LPR often present with symptoms that overlap with AR and asthma15, such as chronic cough, throat clearing, and hoarseness of voice, which further hinders precise diagnoses and proper management. We investigated these conditions’ reciprocal relations to better understand their prevalence, associations, and implications, with the primary focus on elucidating the connections between them and exploring potential solutions for management.
The innovative aspect of our study lies in its comprehensive analysis of how AR and LPR intersect, particularly within a young and educated population. With a sample size of 1,195 participants, our study benefits from enhanced statistical power, allowing for more reliable and generalizable results. This large sample size also increases the precision of our estimates and strengthens the validity of the observed associations.
In patients with AR, an increased frequency of swallowing is typically observed, often attributed to throat irritation and posterior nasal drip. This heightened swallowing may also be exacerbated by gastroesophageal reflux. The impact of AR on the nasal mucosa may similarly affect the laryngeal mucosa, resulting in congestion, edema, and excessive mucous secretion, which contribute to the symptoms of LPR10. This shared effect on the mucosal tissues may elucidate the observed association between LPR and AR.
Additionally, GERD and AR are recognized as significant contributors to chronic cough16. Another phenomenon that may explain this association is the identification of Helicobacter pylori within the sinonasal mucosa, despite its primary association with the gastric mucosa, where it is known to promote and contribute to GERD17. Eosinophils, a critical component of allergic inflammation, have also been identified in the esophageal mucosa of patients with GERD18.
The biological mechanisms underlying the association between AR and LPR are multifaceted. A central aspect of this relationship is the concept of shared inflammatory pathways. These pathways activate group 2 innate lymphoid cells (ILC2s), which rapidly produce type 2 cytokines (IL-5, IL-13, and IL-4) in situ. Consequently, ILC2s play a critical role in the initiation and maintenance of type 2 adaptive immune responses, which ultimately lead to immunoglobulin E (IgE) class switching and mucosal inflammation7. This inflammatory environment may extend beyond the nasal cavity to the laryngopharynx, thereby increasing tissue susceptibility to damage induced by reflux. Conversely, in gaseous reflux, pepsin comes into contact with the upper aerodigestive tract (UAT) mucosa, potentially extending as far as the middle ear, and may inflict damage through subsequent episodes of acid reflux19. This bidirectional relationship establishes a potential vicious cycle in which each condition may exacerbate the other.
The educational background of our sample was notably high, with 83.8% holding a bachelor’s degree. This demographic profile is reflective of a young, educated population, which may influence the reported rates of LPR, AR, and associated factors. Females in our research reported a significantly higher percentage of both AR and LPR symptoms compared to males (p < 0.001). Although Pinart et al. found no sex-related difference in AR prevalence among adults, they did observe a female predominance in adolescents20, which may explain the similar trend in our younger sample. The increased prevalence of LPR among females aligns with findings by Liu et al.21. Similarly, Lechien et al. reported that females are more likely than males to experience severe LPR symptoms and related voice disorders22. These findings might be linked to the hormonal differences between males and females. Research shows that estrogens in females can boost humoral responses, autoimmunity, mast cell reactivity, and delayed type IV allergic reactions, while androgens, progesterone, and glucocorticoids may actually dampen the immune response. Essentially, these immune mechanisms can worsen allergies for females. Plus, T-cell responses fluctuate with the menstrual cycle, which hints at how allergic symptoms can change during that time, as well as during pregnancy, while on oral contraceptives, or with hormone replacement therapy23. There are also anatomical differences, like increased laryngeal sensitivity in females, alongside behavioral factors such as how often they seek healthcare, and all of this adds to the disparities.
Notably, our data revealed that younger adults reported significantly higher rates of LPR symptoms than older adults, in contrast to findings by Lechien et al. and others21,22, who observed a positive correlation between LPR incidence and age. This discrepancy may be due to the demographic profile of our sample, which consists predominantly of younger adults. Moreover, socioeconomic factors were found to influence AR prevalence, with participants reporting sufficient income showing a reduced likelihood of developing AR. Perry et al. suggested that lifestyle and environmental exposures associated with lower income may increase the risk of developing asthma and allergy24.
Overall, a strong association (r = 0.595) between AR and LPR was observed. Participants with AR were six times more likely to experience LPR symptoms compared to those without AR (OR = 5.956), an association notably higher than that reported in some previous research8,9, likely due to the greater sample size of our study. This finding is also consistent with previous results that have linked having LPR or AR to an increased risk of having the other due to the inflammatory processes shared between these conditions10,25, and it further reinforces the need for integrated management strategies for patients presenting with both conditions. However, similar to findings from Kakaje et al.8, the presence of AR did not significantly alter the prevalence of LPR symptoms among asthmatic patients, suggesting that asthma may modulate the relationship between rhinitis and LPR, potentially through overlapping or competing mechanisms.
A strong association between a family history of allergies - particularly in the nose, chest, and skin - and the prevalence of LPR symptoms was identified. This suggests that genetic predisposition to allergic conditions may increase susceptibility to LPR, likely due to the inflammatory effects of allergic conditions on the upper airway and potential impact on esophageal function. Environmental allergens such as dust, insects, animals, and pollen were significantly associated with LPR symptoms, emphasizing the role of external triggers in the manifestation of these symptoms. This finding was more solidified by the participants without allergies to these triggers reporting fewer LPR symptoms.
Nasal symptoms such as a runny nose, sneezing, and nasal congestion were significantly linked to LPR symptoms, with those experiencing these symptoms year-round showing a higher prevalence of LPR (67.1%). Similarly, Luk and DelGaudio highlight that chronic rhinosinusitis is associated with an increased risk of LPR26, while Lechien et al. concluded that LPR contributes to the development of recalcitrant chronic rhinosinusitis25.
The majority of asthmatic patients in our study reported an absence of LPR symptoms (53.5%). This finding contrasts with previous studies that have linked asthma to an increased risk of LPR8,27. However, it is important to note that our sample included only 43 subjects diagnosed with asthma (3.5%), which may have limited our ability to detect a significant association between asthma and LPR.
The clinical implications of what we’ve found really highlight the need for integrated care pathways for AR and LPR, especially among women and younger adults. Clinicians ought to use a dual screening approach, tap into environmental modification strategies, and tackle those socioeconomic barriers that often hinder treatment adherence. And when it comes to places like Sudan, where conflict affects everything, focusing on low-cost interventions and community education can really help ease the added burden of these conditions.
Strengths and limitations
This study has several strengths; it included a large and diverse group of participants, as it was conducted outside of a clinical setting and not limited to those who are severely affected. This enhances the study’s external validity. However, this study is not without limitations. The cross-sectional design limits the ability to establish causality, as it only provides a snapshot of associations at a single point in time. Data collection via an online survey excludes individuals without internet access, potentially biasing the sample. Additionally, the generalizability of the results may be affected by demographic factors, such as the overrepresentation of females and the relatively young age of most participants. We also didn’t account for external factors which may contribute to the causality of symptoms such as: dietary habits, smoking and stress. Moreover, the reliance on non-objective diagnostic methods, such as the RSI and the SFAR, may compromise the accuracy of the conclusions. This may introduce subjectivity and the risk of overestimation, as well as recall bias. The use of self-reported tools was chosen for their practicality, cost-effectiveness, and non-invasive nature, enabling the collection of data from a large population.This limitation is particularly relevant given the limited availability of diagnostic resources in Sudan, where research and healthcare are underfunded. Additionally, a lack of local scientific literature in regard to the prevalence, morbidity, and mortality of the conditions studied further challenges the contextualization of our findings.
Recommendations
To enhance the robustness and applicability of future research, several recommendations can be made: Future studies should consider the use of a longitudinal design to better establish causal relationships. Moreover, researchers should utilize alternative data collection methods to reach individuals without Internet access. For example, using face-to-face interviews or community outreach programs to capture a more representative sample and minimize selection bias. Also, efforts should be made to ensure a more diverse demographic representation in future studies. This includes recruiting participants from various states in Sudan, particularly those that are currently safe and have stable Internet access; this would upgrade the generalizability of the findings. Future research should prioritize the use of objective diagnostic methods alongside self-reported measures. Collaborating with healthcare professionals to obtain clinical confirmations would help mitigate issues related to subjectivity and recall bias. Furthermore, advocating for increased funding and resources for biomedical research in Sudan is crucial. Supporting local researchers and healthcare initiatives can help overcome existing barriers and improve the quality of research outcomes. Future studies should also consider the broader healthcare context in Sudan, including the availability of diagnostic resources. Moreover, replication of this study in other countries and age groups can enhance the scientific pool for our findings.Understanding these limitations can inform more effective research designs and interpretations of findings.
Conclusion
We identified a strong association between AR and LPR. Individuals diagnosed with AR are six times more likely to report LPR symptoms. Despite a small sample of asthmatic patients, the findings suggest that asthma may affect the AR-LPR relationship through complex and overlapping mechanisms. Factors such as age, gender, socioeconomic status, and environmental allergens were significant, with younger adults showing higher LPR prevalence and females reporting a higher percentage of both AR and LPR symptoms. Genetic predisposition and inflammatory processes were suggested as potential mechanisms.
Addressing the reciprocal relationships between AR, LPR, and asthma can significantly enhance the quality of life for affected individuals, particularly in resource-limited settings like Sudan. Integrated care strategies and continued research are crucial steps toward achieving better patient outcomes and advancing healthcare in similar contexts.
Data availability
The data used and/or analysed during the current study are available from corresponding author upon reasonable request.
References
Snow, G., Dhar, S. I. & Akst, L. M. How to understand and treat laryngopharyngeal reflux. Gastroenterol. Clin. N. Am. 50 (4), 871–884 (2021).
Katz, P. O. et al. ACG clinical guideline for the diagnosis and management of gastroesophageal reflux disease. Am. J. Gastroenterol. 117 (1), 27–56. https://doi.org/10.14309/ajg.0000000000001538 (2022).
Anzić, S. A. et al. Eight weeks of Omeprazole 20 mg significantly reduces both laryngopharyngeal reflux and comorbid chronic rhinosinusitis signs and symptoms: randomised, double-blind, placebo‐controlled trial. Clin. Otolaryngol. 43 (2), 496–501. https://doi.org/10.1111/coa.13005 (2018).
Wong, M. W. et al. Clinical and psychological characteristics in gastroesophageal reflux disease patients overlapping with laryngopharyngeal reflux symptoms. J. Gastroenterol. Hepatol. 34 (10), 1720–1726 (2019).
Liu, K., Krause, A. & Yadlapati, R. Quality of life and laryngopharyngeal reflux. Dig. Dis. Sci. 68 (9), 3527–3533 (2023).
Morice, D. et al. Laryngopharyngeal reflux: is laparoscopic fundoplication an effective treatment? Ann. R Coll. Surg. Engl. 104 (2), 79–87 (2022).
Bousquet, J. et al. Allergic rhinitis. Nat. Rev. Dis. Primers 6 (1), 95 (2020).
Kakaje, A., Alhalabi, M. M., Alyousbashi, A. & Ghareeb, A. Allergic rhinitis, asthma and laryngopharyngeal reflux disease: a cross-sectional study on their reciprocal relations. Sci. Rep. 11 (1), 2870 (2021).
Alharethy, S. et al. Correlation between allergic rhinitis and laryngopharyngeal reflux. Biomed. Res. Int. ;2018, 1–6 (2018).
Kung, Y. M. et al. Allergic rhinitis is a risk factor of gastro-esophageal reflux disease regardless of the presence of asthma. Sci. Rep. 9 (1), 15535 (2019).
Farahat, M., Malki, K. H. & Mesallam, T. A. Development of the Arabic version of reflux symptom index. J. Voice. 26 (6), 814e15–814e19 (2012).
Annesi-Maesano, I. et al. The score for allergic rhinitis (SFAR): a simple and valid assessment method in population studies. Allergy 57 (2), 107–114. https://doi.org/10.1034/j.1398-9995.2002.1o3170.x (2002).
Patel, K. B., Mims, J. W. & Clinger, J. D. The burden of asthma and allergic rhinitis. Otolaryngol. Clin. N. Am. 57 (2), 179–189. https://linkinghub.elsevier.com/retrieve/pii/S0030666523001755 (2024).
Linneberg, A. et al. Burden of allergic respiratory disease: a systematic review. Clin. Mol. Allergy. 14 (1), 12. https://doi.org/10.1186/s12948-016-0049-9 (2016).
Lechien, J. R. et al. Evaluation and management of laryngopharyngeal reflux disease: state of the Art review. Otolaryngol–head Neck Surg. 160 (5), 762–782. https://doi.org/10.1177/0194599819827488 (2019).
Sharma, S., Hashmi, M. F. & Alhajjaj, M. S. Cough. In StatPearls (StatPearls Publishing, 2025). http://www.ncbi.nlm.nih.gov/books/NBK493221/.
Nikakhlagh, S. et al. Determining the role of helicobacter pylori in chronic sinus infections using the polymerase chain reaction. Jundishapur J. Microbiol. 8 (3), e20783 (2015).
Spechler, S. J. Gastroesophageal reflux disease and eosinophilic esophagitis. Gastroenterol. Hepatol. (N Y). 15 (2), 111–113 (2019).
Liu, D., Qian, T., Sun, S. & Jiang, J. J. Laryngopharyngeal reflux and inflammatory responses in mucosal barrier dysfunction of the upper aerodigestive tract. JIR 13, 1291–1304 (2021).
Pinart, M. et al. Sex-related allergic rhinitis prevalence switch from childhood to adulthood: a systematic review and meta-analysis. Int. Arch. Allergy Immunol. 172 (4), 224–235. https://doi.org/10.1159/000464324 (2017).
Liu, Z. et al. Characteristics of laryngopharyngeal reflux in patients of different genders and ages. J. Voice. 2022, 0892199722003873 (2022).
Lechien, J. R. et al. Influence of age and sex on clinical and therapeutic features of laryngopharyngeal reflux. Otolaryngol–head Neck Surg. 166 (3), 468–476. https://doi.org/10.1177/01945998211020284 (2022).
Nowak-Wegrzyn, A., Ellis, A. & Castells, M. Sex and allergic diseases. Ann. Allergy Asthma Immunol. 122 (2), 134–135 (2019).
Perry, T. T., Grant, T. L., Dantzer, J. A., Udemgba, C. & Jefferson, A. A. Impact of socioeconomic factors on allergic diseases. J. Allergy Clin. Immunol. 153 (2), 368–377 (2024).
Lechien, J. R., Saussez, S. & Hopkins, C. Association between laryngopharyngeal reflux, gastroesophageal reflux and recalcitrant chronic rhinosinusitis: a systematic review. Clin. Otolaryngol. 48 (4), 501–514. https://doi.org/10.1111/coa.14047 (2023).
Luk, L. & DelGaudio, J. Chapter 3-Laryngopharyngeal reflux in chronic rhinosinusitis: evidence-based practice. Evid.-Based Clin. Pract. Otolaryngol. (2018).
Hamdan, A. L. et al. Laryngopharyngeal symptoms in patients with asthma: a cross-sectional controlled study. Clin. Respiratory J. 10 (1), 40–47. https://doi.org/10.1111/crj.12179 (2016).
Author information
Authors and Affiliations
Contributions
Ahmed Ali contributed to conceptualization, study design, data analysis, writing – original draft, supervision, and correspondence. Mohammed Aldirdiri was involved in methodology and writing – review & editing. Mohammed Abdalgader contributed to validation and writing – review & editing. Nusaiba Hassan participated in data collection, survey design, and writing. Filza Khan contributed to methodology, data interpretation, and writing. Fatima Hussein was involved in data collection, survey administration, and writing. Rayan Hamid⁷ contributed to data collection, survey design, and writing. Mifrah Sherwani participated in data analysis and writing. Mohamed Elbadawi contributed to data collection and validation. Leina Elomeiri was involved in methodology and writing – review & editing. Shahad Elbadawi contributed to data collection and validation. Saba El-Bashir participated in data collection and survey design. Azza Mohammed contributed to data collection and validation. Abdelrahman Idris was involved in data collection and survey administration. Eibaa Syed contributed to data collection and validation. Leina Osman participated in data collection, survey design, and writing. Alaa Hussien contributed to data collection, validation, and writing. Esra Eltayeb was involved in data collection and survey administration.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ali, A., Elbadawi, M.H., Aldirdiri, M. et al. Investigating allergic rhinitis effects on laryngopharyngeal reflux in Sudanese people during the Sudanese armed conflict. Sci Rep 15, 23443 (2025). https://doi.org/10.1038/s41598-025-07517-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-07517-1
