
Abstract
Retinoblastoma, the most common intraocular malignancy in children, represents a significant global health challenge, particularly in low- and middle-income countries, where delayed diagnosis and limited access to care persist. Despite advances in diagnostic and therapeutic approaches, disparities in disease burden remain pronounced. Data on retinoblastoma incidence, prevalence, deaths, and disability-adjusted life years (DALYs) from 1990 to 2021 were extracted from the Global Burden of Disease Study 2021. Countries were categorized into 21 regions, with additional classification by Socio-demographic Index. Linear regression analysis was used to estimate the annual percentage change in age-standardized rates, and future trends were projected using a Bayesian age-period-cohort model. The global incidence of retinoblastoma increased from 4674 cases in 1990 to 6,275 cases in 2021, with the age-standardized incidence rate (ASIR) rising from 0.076 (95% UI: 0.049,0.097) to 0.094 (95% UI: 0.058,0.126) per 100,000 population (EAPC 1.35, 95% CI 1.13–1.56). Prevalence similarly grew, reaching 57,333 cases in 2021 (age-standardized prevalence rate (ASPR): 0.861 per 100,000 (EAPC 1.36, 95% CI 1.15–1.57)). Global DALYs and deaths decreased over the study period, indicating improved survival. However, substantial regional disparities remain: Eastern Sub-Saharan Africa persistently bore the highest burden, while Australasia reported minimal cases. Projections for 2035 suggest a modest rise in ASIR (0.102 (95% UI: 0.049–0.156)), ASPR (0.948 (95% UI: 0.482–1.414)), and the age-standardized DALYs rate (4.187 (95% UI: 2.614–5.760)) per 100,000, while the age-standardized death rate is anticipated to slightly decline from 0.042 (95% UI: 0.041–0.043) to 0.039 (95% UI: 0.023–0.055) per 100,000. The findings highlight a dual trajectory: declining mortality and DALYs amid rising incidence and prevalence, signaling improved survival but an increasing burden on healthcare systems. These results underscore the urgency for equitable public health interventions to enhance early detection, treatment accessibility, and long-term care, particularly in high-burden regions. Strategic investment in healthcare infrastructure and targeted policies is essential to mitigate the growing global burden of retinoblastoma.
Similar content being viewed by others


Introduction
Retinoblastoma is a malignant tumor originating in the retina and represents the most common primary intraocular cancer in children under ten years of age1. Without treatment, the disease is almost invariably fatal within one to two years2. Historically, research on retinoblastoma has predominantly focused on clinical and mechanistic aspects, with limited emphasis on its global burden4.However, early diagnosis and timely intervention dramatically improve prognosis, with survival rates exceeding 95% in high-income countries. In contrast, survival rates in low- and middle-income countries remain approximately 50%3. These disparities exacerbate survival inequalities and impose substantial psychosocial and financial burdens on affected families and healthcare systems in resource-limited settings.
Additionally, the COVID-19 pandemic has further magnified these inequities, disrupting healthcare delivery systems worldwide and delaying cancer diagnoses, particularly in low- and middle-income countries5. Reports indicate a reduction in routine screenings, diagnostic imaging, and treatment services for pediatric cancers, including retinoblastoma, during the pandemic6,7. These disruptions have likely contributed to underreporting and poorer outcomes, raising concerns about the long-term impact on childhood cancer care in vulnerable regions. Addressing these gaps requires robust epidemiological assessments that account for pandemic-related challenges and disparities.
Amid global demographic and epidemiological transitions, a comprehensive evaluation of the burden of retinoblastoma utilizing data from the Global Burden of Disease (GBD) 2021 study is both timely and essential. This analysis examines the global, regional, and national burden of retinoblastoma from 1990 to 2021, with projections extending to 2035. By delineating long-term trends and forecasting future trajectories, the study offers critical insights into the efficacy of existing prevention and treatment strategies.
Results
Global burden of retinoblastoma in 2021
In 2021, the global incidence and prevalence of retinoblastoma significantly increased compared to 1990. The estimated incidence rose from 4674 cases (95% UI: 3033–5953) in 1990 to 6275 cases (95% UI: 3855–8382) in 2021, with age-standardized incidence rate (ASIR) increasing from 0.076 (95% UI: 0.049,0.097) to 0.094 (95% UI: 0.058,0.126) per 100,000 (annual percentage change (EAPC) 1.35, 95% CI 1.13–1.56) (Table 1). Prevalence also surged from 42,550 cases to 57,333 cases, with age-standardized prevalence rate (ASPR) rising to 0.861 per 100,000 (EAPC 1.36, 95% CI 1.15–1.57) (Supplementary Table S1). Conversely, global disability-adjusted life years (DALYs) and deaths declined during this period. Age-standardized DALYs decreased from 4.540 to 3.654 per 100,000 (EAPC − 0.42, 95% CI − 0.53 to − 0.31), while deaths dropped from 3180 to 2762, with age-standardized deaths rate (ASDR) declining to 0.041 per 100,000 (EAPC − 0.44, 95% CI − 0.55 to − 0.33) (Supplementary Tables S2, S3).
Regional and national burden of retinoblastoma in 2021
In 2021, substantial regional disparities in retinoblastoma burden were observed. Eastern Sub-Saharan Africa had the highest incidence, prevalence, DALYs, and deaths, with 1265 new cases (95% UI: 787–1975) and the highest ASIR at 0.200 per 100,000 (95% UI: 0.124–0.313), despite a declining trend (EAPC − 0.67%, 95% CI: − 0.88 to − 0.45). DALYs rose to 92,696 (95% UI: 61,255–142,472), while deaths reached 1,058 (95% UI: 700–1629) (Table 1, Supplementary Tables S1, S2, S3). In contrast, Australasia reported minimal or no cases, with significant declines across all metrics (Table 1, Supplementary Tables S1, S2, S3).
Nationally, Tokelau had the highest ASIR at 1.192 per 100,000 (95% UI: 0.253–3.860) (Fig. 1A), while Malawi recorded the highest DALYs rate at 34.90 per 100,000 (95% UI: 14.34–77.09) (Fig. 1C), and the highest ASDR at 0.399 per 100,000 (95% UI: 0.164–0.883) (Fig. 1D). Developed countries like Finland and Switzerland showed moderate ASIR with declining trends, while Seychelles, Saint Kitts and Nevis, and Qatar reported significantly lower rates across all metrics (Fig. 1).

The ASIR (A), ASPR (B), age-standardized DALYs rate (C) and ASDR (D) per 100,000 population of retinoblastoma by national in 2021. ASIR age-standardized incidence rate, ASPR age-standardized prevalence rate, DALY disability-adjusted-life-year; ASDR age-standardized deaths rate.
Age and gender disparities in the global burden of retinoblastoma
The 2021 global data reveal significant age- and sex-related variations in the burden of retinoblastoma across pediatric populations (Fig. 2). The neonatal period (0–6 days) consistently exhibited the highest rates across all indicators (Fig. 2), with female neonates showing the highest ASIR at 1.338 per 100,000 (95% UI: 0.653–2.007) compared to 0.726 (95% UI: 0.472–0.995) in males (Fig. 2A). ASPR were similarly elevated among female neonates at 12.172 per 100,000 (95% UI: 5.949–18.263) versus 6.653 (95% UI: 4.324–9.114) in males (Fig. 2B). DALYs were also highest in this group, particularly among females at 56.131 per 100,000 (95% UI: 23.154–84.103) compared to 23.147 (95% UI: 12.191–33.414) in males (Fig. 2C). ASDR followed a similar pattern, with rates of 0.615 per 100,000 (95% UI: 0.252–0.924) in females and 0.253 (95% UI: 0.133–0.366) in males (Fig. 2D).

Trends in the number of incidence cases and ASIR (A), the number of prevalence cases and ASPR (B), the number of DALYs and the age-standardized DALYs rate (C), and the number of deaths and ASDR (D) by age and gender globally. ASIR(A), ASPR(B), the age-standardized DALYs rate(C) and ASDR (D) for females and males are illustrated with red and blue lines, respectively, each accompanied by a 95% confidence interval. Red and blue bars show the actual number of incidence (A), prevalence (B), DALYs (C) and deaths (D) cases, providing a clear visual comparison of age-specific burdens between genders. ASIR age-standardized incidence rate, ASPR age-standardized prevalence rate, DALY disability-adjusted-life-year, ASDR age-standardized deaths rate.
As age increased, the 2–4 years age group exhibited the highest burden across all indicators (Fig. 2). The estimated prevalence was 1912 cases (95% UI: 1020–2793) in males and 1,738 cases (95% UI: 798–2549) in females (Fig. 2A), with total prevalence reaching 17,499 cases (95% UI: 9341–25,565) in males and 15,806 cases (95% UI: 7256–23,192) in females (Fig. 2B). The burden of DALYs remained considerable in this cohort, with males accounting for 81,006 cases (95% UI: 42,818–122,752) and females for 75,331 cases (95% UI: 31,604–106,572) (Fig. 2C). Deaths was also significant, with 923 deaths (95% UI: 488–1399) in males and 858 deaths (95% UI: 359–1215) in females (Fig. 2D).
Trends and correlations of retinoblastoma burden by socio-demographic index levels
From 1990 to 2021, global age-standardized incidence and prevalence rates of retinoblastoma increased across all SDI levels, while DALYs and deaths declined (Table 1, Supplementary Tables S1, S2, S3). The most significant changes occurred in high-middle SDI regions, where EAPCs for incidence and prevalence were − 3.58 (95% CI 3.10–4.06) and 3.59 (95% CI 3.11–4.07), respectively, while DALYs and deaths declined with EAPCs of − 2.49 (95% CI − 2.18 to − 2.79) and − 2.77 (95% CI − 2.46 to − 3.09) (Table 1, Supplementary Tables S1, S2, S3). A positive correlation was observed between SDI and both ASIR (r = 0.221, p < 0.001) and ASPR (r = 0.224, p < 0.001), while negative correlations were seen for DALYs (r = − 0.809, p < 0.001) and ASDR (r = − 0.808, p < 0.001) (Fig. 3, Supplementary Fig. S1).

ASIR (A) and ASPR (B) of retinoblastoma by 21 GBD regions and SDI, 1990–2021. ASIR (C) and ASPR (D) of retinoblastoma by 204 countries and SDI, 1990–2021. The solid line represents expected values calculated from SDI and aggregate disease rates. Thirty-two data points per region depict observed rates for each year; the shaded area shows the 95% confidence interval of these expectations. Points above and below the line indicate higher and lower-than-expected disease burdens, respectively. GBD global burden of diseases, injuries, and risk factors study, SDI sociodemographic index, EAPC estimated annual percentage change, ASIR age-standardized incidence rate, ASPR age-standardized prevalence rate, DALY disability-adjusted-life-year.
In 2021, deviations from expected retinoblastoma burden based on SDI were evident in 204 countries. Kenya, Portugal, and Malawi reported higher-than-expected ASIR and ASPR, while Kenya, Tokelau, and Malawi had elevated DALYs and ASDR (Fig. 3, Supplementary Fig. S1). A negative correlation between SDI and DALYs (r = − 0.713, p < 0.001) and ASDR (r = -0.729, p < 0.001) was noted, though no significant correlation was found for incidence (r = − 0.107, p = 0.128) or prevalence (r = − 0.105, p = 0.136).
Global disease burden prediction for retinoblastoma by 2035
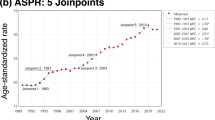
The global Bayesian age-period-cohort (BAPC) model forecasts a modest increase in ASIR, ASPR, and the age-standardized DALYs rate attributable to retinoblastoma over the next 14 years, while ASDR is projected to decline (Fig. 4). Specifically, ASIR is expected to rise from 0.094 per 100,000 (95% UI: 0.092–0.097) in 2021 to 0.102 per 100,000 (95% UI: 0.049–0.156) by 2035 (Fig. 4A). Similarly, ASPR is anticipated to increase from 0.857 per 100,000 (95% UI: 0.850–0.864) in 2021 to 0.948 per 100,000 (95% UI: 0.482–1.414) in 2035 (Fig. 4B). The age-standardized DALYs rate is projected to grow from 3.641 per 100,000 (95% UI: 3.626–3.655) in 2021 to 4.187 per 100,000 (95% UI: 2.614–5.760) by 2035 (Fig. 4C). In contrast, ASDR is expected to slightly decline from 0.042 per 100,000 (95% UI: 0.041–0.043) in 2021 to 0.039 per 100,000 (95% UI: 0.023–0.055) in 2035 (Fig. 4D).

The trends of ASIR (A), ASPR (B), age-standardized DALYs rate (C) and ASDR (D) per 100,000 population of retinoblastoma from 1990 to 2021. ASIR age-standardized incidence rate, ASPR age-standardized prevalence rate, DALY disability-adjusted-life-year, ASDR age-standardized deaths rate.
Moreover, projections suggest a significant escalation in the burden of retinoblastoma between 2021 and 2035 (Fig. 5). The incidence of retinoblastoma is expected to rise from 7468 cases (95% UI: 7,222–7,715) in 2021 to 9138 cases (95% UI: 4363–13,912) by 2035, reflecting an increase of approximately 22.4% (Fig. 5A). Correspondingly, prevalence is projected to grow from 67,626 cases (95% UI: 66,875–68,377) in 2021 to 84,533 cases (95% UI: 42,963–126,104) in 2035, representing an increase of 25.0% (Fig. 5B). The burden of disease, as measured by DALYs, is anticipated to escalate from 287,305 (95% UI: 285,755–288,855) in 2021 to 373,039 (95% UI: 225,724–520,353) in 2035, signifying a rise of 29.8% (Fig. 5C). Deaths is also projected to increase, with deaths expected to rise from 3314 (95% UI: 3157–3471) in 2021 to 3474 (95% UI: 2032–4916) in 2035, marking a 4.8% increase (Fig. 5D).

Trends in the number of incidence (A), prevalence (B), DALYs (C) and deaths (D) cases of retinoblastoma from 1990 to 2021. DALY disability-adjusted-life-year.
Discussion
The 2021 global assessment of retinoblastoma presents a nuanced epidemiological landscape characterized by divergent trends in ASIR, ASPR, the age-standardized DALYs rate and ASDR. The concurrent decline in DALYs and mortality rates for retinoblastoma, despite rising incidence and prevalence, highlights significant advancements in pediatric oncology. These improvements are driven by multifaceted advancements in treatment modalities. Chemotherapy, particularly intravitreal and intra-arterial delivery methods, has enhanced tumor control while minimizing systemic toxicity8. Similarly, the evolution of radiotherapy, exemplified by precision techniques such as proton beam therapy, has enabled effective targeting of retinoblastoma cells with reduced damage to surrounding healthy tissues2. Surgical interventions, including enucleation and globe-salvaging procedures9, have also advanced, supported by improved perioperative care and multidisciplinary approaches, further lowering mortality risks. Enhanced supportive care systems, including advanced diagnostic imaging, genetic counseling, and psychosocial support for families, have contributed to earlier detection and improved adherence to treatment, particularly in high-income countries10,11. Additionally, the integration of comprehensive referral networks and adherence to standardized guidelines, such as those proposed by the International Retinoblastoma Consortium, has been instrumental in achieving superior survival outcomes. This improvement is a critical achievement in pediatric oncology, reflecting global efforts to enhance survival through integrated care pathways and international guidelines that standardize treatment protocols across regions.
Regional disparities in the burden of retinoblastoma remain stark, with Eastern Sub-Saharan Africa bearing the highest burden across all metrics as of 2021. Despite a gradual decline in ASIR and prevalence since 1990, this region continues to report alarmingly high levels of DALYs, alongside a concerning increase in mortality rates. These trends reflect persistent systemic challenges. The high burden in Eastern Sub-Saharan Africa is further exacerbated by socioeconomic inequalities, which restrict access to advanced diagnostic tools and effective therapeutic options12. Limited awareness about early symptoms among caregivers and healthcare workers compounds delays in diagnosis, often resulting in advanced-stage presentations. Additionally, the absence of well-coordinated referral networks and a lack of pediatric oncology expertise impede timely interventions, contributing to the region’s elevated mortality rates and poorer outcomes compared to other regions13. Addressing these disparities requires multifaceted approaches, including the establishment of regional centers of excellence for pediatric oncology, investment in healthcare infrastructure, and targeted community education programs to promote early detection3,14,15.
In contrast, regions such as Australasia report minimal cases of retinoblastoma, reflecting the critical role of robust public health strategies and advanced healthcare infrastructure. Australasian countries, including Australia and New Zealand, have long prioritized universal healthcare coverage, comprehensive newborn screening initiatives, and well-coordinated referral pathways, all of which contribute to early detection and timely management of retinoblastoma16,17. For example, highly integrated cancer registries and specialized pediatric oncology centers in these countries ensure equitable access to diagnostic and therapeutic interventions. Public awareness campaigns and government-subsidized healthcare services further mitigate delays in diagnosis and enhance treatment adherence, leading to consistently high survival rates.
Comparisons with other high-income countries further contextualize Australasia’s success. While North America and Western Europe also demonstrate low retinoblastoma burdens and high survival rates, disparities in health insurance coverage and variations in treatment access occasionally compromise uniform care delivery18. In contrast, Australasian policies emphasize universal accessibility, resulting in fewer care gaps. For instance, Australia’s Medicare system subsidizes critical retinoblastoma treatments, effectively reducing socioeconomic barriers to care. Expanding these successful strategies to low- and middle-income countries could involve implementing scalable interventions, such as subsidized healthcare services, the establishment of regional referral networks, and enhanced training programs for healthcare professionals specializing in pediatric oncology. Adapting these proven policies from Australasia could play a pivotal role in improving global outcomes in retinoblastoma management.
At the national level, Tokelau exhibits the highest ASIR and ASPR, with rising trends likely driven by genetic, environmental, or population factors, highlighting the need for localized research. Malawi, with the highest age-standardized DALYs rate and ASDR, demonstrates the severe impact of limited healthcare resources on disease outcomes. The modest decline in DALYs and mortality suggests current interventions are insufficient to significantly reduce the burden. In contrast, countries like Finland and Switzerland show declining trends with moderate incidence, reflecting effective public health efforts, while low rates in Seychelles and Qatar may be due to smaller populations and favorable healthcare infrastructures19.
The significant age- and sex-related variations in the global burden of retinoblastoma observed in 2021 are likely driven by a multifactorial interplay of biological, genetic, environmental, and healthcare-related factors20. Mutations in the RB1 gene are the primary driver of the disease, with early-onset mutations suggesting prenatal development, particularly in female neonates, who exhibit a higher burden of disease21. Emerging evidence suggests that sex-specific genetic susceptibility, including differences in tumor suppressor gene expression and hormonal pathways, may contribute to the observed disparities. Additionally, epigenetic modifications, such as DNA methylation and histone modifications, could differentially regulate RB1 expression in males and females, amplifying these disparities. These epigenetic influences may be further shaped by environmental exposures, including parental occupational hazards and prenatal factors, which are associated with sporadic cases. Understanding these mechanisms is critical for informing future research into targeted preventive and therapeutic strategies and addressing the sex-based disparities in retinoblastoma outcomes.
As children age, the burden of retinoblastoma remains substantial, with the highest burden observed in the 2–4 years age group. This pattern may reflect the progression of undiagnosed or late-onset cases that become symptomatic over time, underscoring the persistent challenges in early detection and the impact of delayed diagnosis. Disparities in healthcare access, treatment responses, and survival outcomes are particularly pronounced between sexes, with males experiencing higher DALYs and mortality. These differences highlight inequities in disease management and outcomes, further exacerbated by global disparities in healthcare infrastructure. High-income regions benefit from robust screening and treatment programs, enabling timely interventions, whereas lower-income regions often face delays in diagnosis and limited access to effective care, disproportionately increasing the disease burden among older children.
Addressing these disparities requires a multifaceted and equity-driven approach. Strengthening screening programs, particularly in low- and middle-income countries, could enable early detection and intervention, while regionalizing care through specialized retinoblastoma centers and subsidized treatment programs could reduce financial and logistical barriers. Tailored education campaigns in local contexts can further promote public awareness, encourage early diagnosis, and improve treatment adherence. Future research should prioritize the investigation of genetic, environmental, and epigenetic determinants of retinoblastoma to better understand disparities in incidence and outcomes10,12. Moreover, the development and scaling of innovative care delivery models, such as telemedicine and mobile health platforms, alongside implementation science research to identify barriers to adopting evidence-based interventions, are critical to ensuring equitable access to life-saving treatments globally.
The projected increase in the global burden of retinoblastoma by 2035, as indicated by rising ASIR, ASPR, and age-standardized DALYs rate, alongside a modest decline in ASDR, reflects both advancements in healthcare and ongoing challenges. The anticipated rise in incidence and prevalence is likely driven by global population growth and demographic shifts, particularly in regions with high birth rate3. Even modest increases in age-standardized rate can translate into significant absolute numbers of cases. Additionally, improvements in early detection and treatment, especially in high-income countries, have led to better survival rates, contributing to increased prevalence while reducing the severity of disease outcomes, as evidenced by the projected decline in ASDR.
However, the persistent increase in DALYs and the modest rise in deaths suggest that significant disparities in healthcare access and quality continue to exist, particularly in low- and middle-income countries. Delays in diagnosis and limited access to effective treatment in these regions contribute to ongoing morbidity and mortality, leading to a high burden of disease. The modest decline in ASDR, despite rising incidence and prevalence, indicates that healthcare systems are improving in managing retinoblastoma, particularly in reducing mortality. Yet, the overall increase in disease burden underscores the need for enhanced public health efforts, including expanded screening programs, better access to early diagnosis, and more equitable distribution of healthcare resources, to effectively curb the rising incidence and address the long-term impacts of retinoblastoma globally14.
This study provides a comprehensive and longitudinal analysis of the global burden of retinoblastoma from 1990 to 2021, utilizing high-quality data from the GBD 2021 study. The robustness of the data ensures that the findings are both globally representative and regionally insightful, addressing critical disparities in disease burden. Furthermore, the study’s projection of disease metrics to 2035 offers a forward-looking perspective, enabling policymakers to anticipate trends and allocate resources proactively to mitigate the anticipated rise in incidence and prevalence. These strengths position the study as a critical resource for informing global health strategies and targeted interventions in pediatric oncology. Despite its strengths, this study has certain limitations that warrant consideration. While the study acknowledges the potential impact of the COVID-19 pandemic on retinoblastoma detection and care, more detailed quantification and exploration of these disruptions would enhance the contextual understanding of the pandemic’s influence. Furthermore, the emphasis on global and regional trends, while insightful, may obscure critical localized interventions and context-specific challenges, highlighting the importance of tailoring findings to address nuanced regional disparities in retinoblastoma management.
In conclusion, this study delineates the global burden of retinoblastoma, revealing a rising incidence and prevalence over the past three decades, accompanied by notable reductions in DALYs and mortality. However, pronounced regional disparities, particularly in high-burden areas such as Eastern Sub-Saharan Africa, underscore the urgent need for targeted public health strategies. Future research should focus on elucidating the interplay between genetic predisposition and socioeconomic determinants and evaluating the effectiveness of community-based education initiatives and scalable care delivery models, coupled with investments in healthcare infrastructure and innovative interventions, hold the potential to mitigate retinoblastoma’s most severe outcomes and alleviate its burden, particularly in resource-limited settings.
Methods
Data sources
To support the models, the GBD study employs an extensive data acquisition strategy that encompasses systematic reviews, opportunistic searches, and the integration of data from national collaborators22. This iterative and ongoing process is designed to continuously identify and incorporate new sources23. The methodologies and data-seeking approaches underpinning GBD iterations, including GBD 2021, have been comprehensively documented and are accessible via the Global Health Data Exchange query tool (http://ghdx.healthdata.org/gbd-results-tool). For this analysis, data were confined to 2021, as it represents the most recent year with comprehensive and validated estimates available through the GBD framework. The rigorous multi-year data processing and validation cycle ensures the reliability and comparability of estimates across countries and regions.
The GBD 2019 analysis revealed significant limitations in the representation of retinoblastoma, particularly in comparison to other pediatric malignancies. This underrepresentation was largely attributable to limited data availability and the relative rarity of the disease. In contrast, the GBD 2021 update has made substantial progress in improving coverage, incorporating more comprehensive data from national cancer registries and specialized studies. These enhancements have significantly advanced the understanding of retinoblastoma’s global burden, providing more accurate estimates of its incidence, prevalence, and outcomes across diverse populations. Such progress is especially critical for rare pediatric cancers like retinoblastoma, which have historically been underrepresented in global health assessments.
In the GBD 2021 study, retinoblastoma is defined as a malignant neoplasm originating from the retina, primarily affecting children under 10 years of age. It is recognized as the most common primary intraocular cancer in this age group. The GBD 2021 dataset is meticulously structured, categorizing countries and territories into seven super-regions and 21 regions based on geographic proximity and epidemiological characteristics. This classification system provides a nuanced understanding of regional health dynamics, facilitating meaningful comparisons across diverse global contexts.
Statistical analysis
This study conducted a secondary analysis of data from the GBD 2021 study, addressing three primary objectives. First, we assessed the burden of retinoblastoma-related conditions in 2021, stratifying the analysis by sex, SDI, and country. The burden was quantified using the number of cases and age-standardized rates, including ASIR, ASPR, DALYs, and ASDR. DALYs, as a comprehensive measure of disease burden, capture the combined impact of premature mortality (years of life lost, YLLs) and non-fatal health outcomes (years lived with disability, YLDs)22. This metric provides a unified framework to compare the burden of retinoblastoma across regions and demographic groups.
Second, we evaluated trends in the burden of retinoblastoma-related conditions from 1990 to 2021. To quantify these trends, we estimate the EAPC in age-standardized rates globally and across subgroups, including sex, SDI, and GBD regions. The relationship between SDI and disease burden was examined using regression analysis, assessing the correlation between SDI values and retinoblastoma-related metrics. SDI, as defined by the GBD study, is a composite index incorporating income, education, and fertility rates, extensively used to adjust for socioeconomic differences across regions. SDI adjustments in this study provided a clearer understanding of how socioeconomic factors contribute to the burden of retinoblastoma. Spearman’s rank correlation coefficient was employed to quantify the strength and direction of these associations. All age-standardized rates were derived from the GBD reference population.
Finally, a BAPC model, incorporating integrated nested Laplace approximations, was used to project the burden of retinoblastoma-related conditions from 2021 to 2035. Projections were reported with 95% confidence intervals to account for the uncertainty of these estimates.
All data collation and statistical analyses were conducted using R software (version 4.0.2).
Data availability
The data that support the findings of this study were obtained from the Global Burden of Disease (GBD) Study 2021. The GBD data are publicly available and can be accessed through the Global Health Data Exchange (GHDx) query tool at https://vizhub.healthdata.org/gbd-results/.
References
Kaliki, S. et al. Clinical presentation and outcome of retinoblastoma based on age at presentation: a review of 1450 children. International Ophthalmology. 40, 99–107 (2020).
Tanveer, S. et al. Advancements in retinoblastoma treatment: Unraveling the potential of intravitreal chemotherapy. Cureus https://doi.org/10.7759/cureus.53012 (2024).
Fabian, I. D. et al. Global retinoblastoma presentation and analysis by national income level. JAMA Oncol. 6(5), 685–695 (2020).
Li, C. et al. Global, regional and national burden due to retinoblastoma in children aged younger than 10 years from 1990 to 2021. BMC Med. 22(1), 604 (2024).
Villain, P. et al. Cross-sectional survey of the impact of the COVID-19 pandemic on cancer screening programs in selected low-and middle-income countries: Study from the IARC COVID-19 impact study group. Int. J. Cancer 149(1), 97–107 (2021).
Dvori, M. et al. Delayed diagnosis and treatment of children with cancer during the COVID-19 pandemic. Int. J. Clin. Oncol. 26(8), 1569–1574 (2021).
Arul, J. et al. Challenges in the management of retinoblastoma during nationwide lockdown: An observational study from a retinoblastoma center in South India. Indian J. Med. Paediatr. Oncol. 43(03), 250–254 (2022).
Shields, C. L. et al. Retinoblastoma frontiers with intravenous, intra-arterial, periocular, and intravitreal chemotherapy. Eye 27(2), 253–264 (2013).
Shields, C. L. et al. Diffuse anterior retinoblastoma with globe salvage and visual preservation in 3 consecutive cases. Ophthalmology 123(2), 378–384 (2016).
He, L. Q. et al. Developing clinical cancer genetics services in resource-limited countries: the case of retinoblastoma in Kenya. Public Health Genom. 17(4), 221–227 (2014).
Patenaude, A. F. & Wakefield, C. E. Psychosocial aspects of childhood cancer genetics. In The Hereditary Basis of Childhood Cancer 445–471 (Springer International Publishing, 2021).
Meel, R., Radhakrishnan, V. & Bakhshi, S. Current therapy and recent advances in the management of retinoblastoma. Indian J. Med. Paediatr. Oncol. 33(02), 80–88 (2012).
Lam, C. G. Retinoblastoma as a lens for correctable disparities worldwide. Lancet Glob. Health 10(8), e1074–e1075 (2022).
Byroju, V. V. et al. Retinoblastoma: present scenario and future challenges. Cell Commun. Signal. 21(1), 226 (2023).
Ramírez-Ortiz, M. A. et al. Systematic review of the current status of programs and general knowledge of diagnosis and management of retinoblastoma. Bol. Méd. Del Hosp. Infant. Méx. Engl. Ed. 74(1), 41–54 (2017).
Jullien, S. Vision screening in newborns and early childhood. BMC Pediatr. 21(Suppl 1), 306 (2021).
Wong, E. S. et al. Global retinoblastoma survival and globe preservation: a systematic review and meta-analysis of associations with socioeconomic and health-care factors. Lancet Glob. Health 10(3), e380–e389 (2022).
Goutté, N. et al. Geographical variations in incidence, management and survival of hepatocellular carcinoma in a western country. J. Hepatol. 66(3), 537–544 (2017).
Gallie, B. L. et al. Global issues and opportunities for optimized retinoblastoma care. Pediatr. Blood Cancer 49(S7), 1083–1090 (2007).
Orjuela-Grimm M, Singh N, Bhatt-Carreño S et al. Retinoblastoma: incidence and etiologic factors. Clin. Ophthalmic Oncol. Retinoblastoma. 39–56. (2019).
Mehyar, M. et al. Impact of RB1 gene mutation type in retinoblastoma patients on clinical presentation and management outcome. Hematol. Oncol. Stem Cell Ther. 13(3), 152–159 (2020).
Vos, T. et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet 396(10258), 1204–1222 (2020).
Naghavi, M. et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet, 403(10440), 2100–2132 (2024).
Acknowledgements
We would like to extend our sincere thanks to Hongjun Zhu, Meng Zhao, and Jinxin Zheng for their invaluable contributions to this research. We are also grateful to the Global Burden of Disease project and the Institute for Health Metrics and Evaluation for providing the data used in this study. Additionally, we acknowledge all the healthcare professionals and researchers whose efforts have helped advance our understanding of retinoblastoma.
Author information
Authors and Affiliations
Contributions
Hongjun Zhu: Led the conceptualization, methodology, and manuscript drafting. Accessed and verified the data. Meng Zhao: Conducted investigation, data curation, and analysis. Contributed to manuscript drafting and revisions. Accessed and verified the data. Jinxin Zheng: Contributed to conceptualization, methodology, and data interpretation. Involved in critical manuscript revision. All authors: Participated in study design, data acquisition, analysis, drafting, or revision. Approved the final manuscript. The authors declare that this manuscript, including data, figures, and tables, is original and not under consideration elsewhere.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhu, H., Zhao, M. & Zheng, J. Global, regional, and national burden of retinoblastoma in children aged under 10 years from 1990 to 2021 and projections for future disease burden. Sci Rep 15, 7488 (2025). https://doi.org/10.1038/s41598-025-91289-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-91289-1
