
Abstract
In the field of indoor thermal comfort research, there has been relatively little focus on the thermal comfort of orthopedic patients in indoor diagnostic and treatment spaces. To effectively improve the microclimate of orthopedic indoor treatment spaces in hospitals and provide a comfortable environment for orthopedic patients. This study focused on the thermal comfort of orthopedic patients. Meteorological measurements and questionnaires were conducted in six typical indoor treatment spaces selected from the orthopedic waiting area and ward area of the Northern Campus of Xi’an Honghui Hospital. Based on the survey data, optimization strategies for orthopedic indoor diagnostic and treatment spaces were proposed. Through the analysis of subjective responses from orthopedic patients and measured indoor thermal conditions, it was found that the thermal environment of orthopedic indoor diagnostic and treatment spaces in hospitals could meet the needs of most people (92.3%) in spring. At a Thermal Sensation Vote (TSV) of + 0.21, the occupants in these spaces exhibited the most comfortable state, with a neutral Standard Effective Temperature (SET) range of 13.0 to 22.73 °C and a 90% thermally acceptable SET range of 15.8 to 27.4 °C. Orthopedic patients were more sensitive to changes in the thermal environment compared to healthy individuals, with a neutral SET* of 17.7 °C for orthopedic patients and 21.7 °C for healthy individuals. This study addresses the subjective responses and meteorological factor preferences of orthopedic patients, proposing targeted measures and suggestions for orthopedic treatment spaces in hospitals. Additionally, it provides scientific evidence and practical guidance for the rehabilitation of orthopedic patients and indoor treatment environments in regions of the same latitude.
Similar content being viewed by others
Introduction
Since the 21st century, China has achieved a comprehensive leapfrog development in various high-tech industries, including medical technology, leading to a significant improvement in medical service levels. However, at the same time, patients’ demands for a thermally comfortable hospital environment have also increased. Currently, domestic and foreign scholars’ research on indoor thermal comfort mostly focuses on residential, commercial, and office buildings1, with relatively fewer studies on hospital buildings. Nevertheless, in hospital environments, patients tend to have stricter requirements for indoor thermal environments and a more urgent need for thermally comfortable environments. Especially for orthopedic patients, due to the particularities of their conditions, they face special situations such as difficulty in movement or even prolonged bed rest caused by pain or postoperative recovery. Therefore, orthopedic patients have stricter requirements for the indoor thermal environment in hospitals compared to other populations.
Orthopedic patients are more sensitive to thermal environments due to their pain. Compared to warm environments, cooler environments are more conducive to alleviating patients’ pain. Jennie et al.2 explored that the comfortable temperature for orthopedic ward patients in hospitals during summer is 25 °C, while considering both patients and medical staff, the comfortable temperature is 22.4 °C. Therefore, when predicting the neutral temperature of wards, patients and staff should be considered separately. Pourshaghaghy et al.3 found through research that the average dissatisfaction rate in hospitals during summer is higher than that in winter, indicating that people have a higher acceptance of cold environments. During orthopedic patient recovery, pain can hinder the patient’s recovery process from both physiological and psychological aspects, directly reducing the patient’s sleep quality, affecting their mood, and causing anxiety and tension. A good indoor thermal environment can effectively reduce patients’ pain, accelerate their recovery process, and improve the quality of medical services.
According to scientific research, humans spend approximately 80–90% of their lives indoors, and the indoor thermal environment is closely related to human physical health and emotional stability4. Scholars have found that there are many factors affecting human thermal comfort, and they have conducted in-depth research and analysis on relevant standards5,6,7,8. In addition, some scholars have proposed the “adaptive hypothesis” and constructed a regression equation for neutral temperature and the indoor mean temperature, along with the Standard Effective Temperature (SET) index9,10. However, the Operative Temperature (OT) is currently the most commonly used thermal comfort evaluation index, which is a composite temperature that considers the combined influence of air temperature and mean radiant temperature on human thermal sensation. In 2007, Nilsson et al.11 used CDD software to build a human body model and obtained thermal response results by setting environmental parameters, which were used to study human thermal comfort.
There is a close relationship between the thermal environment of hospitals and patients’ thermal comfort. Hashiguschi et al.12 conducted a thermal comfort survey among patients during the winter in Japan and found that there were differences in the perception of air temperature and relative humidity between patients and healthy individuals. Skoog, Rucy-Lung, and others13,14 investigated the indoor thermal environment for both patients and healthy individuals, finding that the activity levels of patients significantly affect their thermal sensation. Additionally, the health status of individuals also has a considerable impact on patients’ thermal perception. In 2007, Balaras and Mazzacane15,16 conducted a study on the indoor thermal environment in hospital operating rooms. They discovered that the thermal conditions in most of the selected operating rooms did not meet international standards. Furthermore, they found significant differences in the activity intensity of medical staff performing different types of surgeries, indicating that the internationally accepted thermal comfort standards are not suitable for all scenarios. In 2012, A. Pourshaghaghy et al.3 conducted a thermal comfort study in hospital wards, emergency rooms, operating rooms, and laboratories and found no significant difference between the calculated PMV index values and the actual thermal sensation voting results in winter and summer. In the same year, Jamal Khodakarami et al.17 pointed out that thermal comfort in hospitals was closely related to the work efficiency of medical staff. In 2015, Del F S et al.18 based on PMV and Thermal Sensation Vote (TSV), considered the effects of age and gender and found that medical staff preferred warmer environments, and the PMV model could not accurately predict patients’ actual thermal comfort. Women were more likely to feel discomfort in the thermal environment compared to men. Jan et al.19 found that when predicting patients’ average thermal sensation votes, the health status of the subjects should be considered in the PMV model. In 2018, Derks M T H et al.20 studied the thermal neutral temperature of medical staff in Dutch hospitals and found that the thermal neutral temperature of medical staff was lower than that of patients. To meet the overall needs, the thermal environment in different areas should be adjusted in blocks. In the same year, Khalid W et al.21 conducted a survey on thermal comfort in the ward environment in Malaysia and found that the temperature and humidity control in the inpatient ward area did not meet local national standards, and the patients’ health status affected their judgment of thermal environment comfort and their preference for meteorological factors.
The objectives of this study are to: (1) establish the neutral temperature and neutral temperature range for orthopedic patients and individuals of different age groups; (2) explore the influence of age, gender, and health status on the subjective responses of respondents and their preferences for meteorological factors in indoor environments. Research results can guide the practical renovation work of orthopedic indoor treatment spaces, enhance patients’ healthcare experiences and treatment outcomes, and ultimately promote the improvement of medical and healthcare service quality.
Research methodology
Geographical ___location and climate
According to the climate regions classified by the “Code for Thermal Design of Civil Buildings” (GB 50176 − 1993) issued in China in 1993, Xi’an is located in a cold region with a warm temperate semi-humid continental monsoon climate, featuring distinct seasons and moderate rainfall. Based on Köppen’s climate classification, Xi’an lays at the boundary between the semi-arid (Bsk) and subtropical humid climate zones (Cwa). The questionnaire survey and field measurements were conducted at the northern campus of Xi’an Honghui Hospital (108°9′E, 34°39′N). Xi’an Honghui Hospital is one of the key construction projects in the health and wellness sector of Xi’an, and it is a comprehensive modern hospital integrating medical treatment, education, research, and rehabilitation. With its large scale and substantial number of orthopedic patients, Xi’an Honghui Hospital provides an ideal environment for conducting the questionnaire survey.
Based on the actual medical treatment situation of orthopedic patients, this study selected six locations for meteorological factor data measurement and questionnaire distribution: the joint revision ward area, the bone necrosis and joint reconstruction ward area, the rheumatology and orthopedics ward area, the joint revision waiting area, the bone necrosis and joint reconstruction waiting area, and the rheumatology and orthopedics waiting area. The questionnaire locations are shown in Fig. 1a–d.
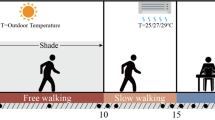
The questionnaire survey and field measurements for this study were conducted from April 8th to April 16th, 2024, and April 18th to April 25th, 2024. The weather conditions during this period are shown in Fig. 1e Weather Condition Chart.

On-site showcase of questionnaire locations and weather condition chart.
Experimental design
This study investigates the indoor thermal comfort of orthopedic patients in the spring season at the northern campus of Xi’an Honghui Hospital through methods such as questionnaire surveys and field measurements.
The physical environment data measured includes: air temperature (\(\:{T}_{a}\)), relative humidity (RH), wind speed (\(\:{V}_{a}\)), and globe temperature (\(\:{T}_{g}\)). The JT2020 multi-function tester is used to record and measure the data for\(\:\:{T}_{a}\), RH,\(\:{\:V}_{a}\), and\(\:{\:T}_{g}\), all instruments were installed at a height of 1.2 m above the ground. With its specific parameters detailed in Table 1. To avoid disrupting the normal diagnosis and treatment work of medical staff and the recovery of patients, the experiment time is set from 10:00 to 16:00 in the inpatient wards and from 10:00 to 12:00 and 14:00 to 16:00 in the waiting areas. A total of six testing sites are established in the selected ward areas and waiting areas, and the data collected from each site during the testing process is presented in Table 2.
Questionnaire survey
In this study, orthopedic patients and healthy people in the experimental sites were selected as the respondents for the questionnaire survey. At the same time of measuring the physical environment data, a questionnaire survey was conducted among the people in the orthopedic indoor diagnosis and treatment space of the hospital. The questionnaire is divided into two parts. The first part includes basic information such as gender, age, blood type, occupation, clothing, and main activities within 20 min. The thermal resistance of the respondents’ clothing is referenced according to the ASHRAE 55 and ISO 7730 standards. The metabolic rate is determined by recording the respondent’s activities, and the activity types are set according to the common activities in orthopedic departments of hospitals.
Data processing
Since TSV (Thermal Sensation Vote) is an ordinal variable, this study employs Spearman’s rank correlation analysis to determine the correlation between participants’ thermal sensation and variables such as air temperature, relative humidity, wind speed, globe temperature, metabolic rate, and clothing thermal resistance. A correlation coefficient greater than 0 is considered a positive correlation, and vice versa for a negative correlation. Generally, an absolute correlation coefficient greater than 0.7 indicates a strong correlation between two variables, an absolute value between 0.4 and 0.7 suggests a moderate-strong correlation, and an absolute value less than 0.2 indicates a weak correlation. R-squared (R²) is the coefficient of determination; the closer R² is to 1, the better the model fits the data.
Mean radiant temperature (\(\:{T}_{mrt}\))
Mean radiant temperature is an important thermal environment parameter, reflecting the influence of radiant heat from surrounding surfaces on the human body. This study calculates the mean radiant temperature according to the ISO 7726 standard. As shown in Eq. 1.
Where \(\:{\upepsilon\:}\:\)is the reflectance of the black globe; D is the diameter of the black globe (In this study\(\:\:{\upepsilon\:}\)= 0.95, D= 0.05 m).
Basic information of the subjects
A total of 670 questionnaires were distributed in this study, with all 670 questionnaires being actually recovered, resulting in an initial response rate of 100%. To identify outliers for each parameter in the collected questionnaires, box plots were utilized. Specifically, if a particular indicator from a questionnaire exceeded the normal range, it was excluded from the analysis during the result interpretation phase22. Ultimately, a total of 643 valid questionnaires were collected during the survey period, representing an effective response rate of 95.97%. The basic information of the respondents in this study is presented in Table 3.
Results
Subjective responses
Thermal sensation vote (TSV) and thermal comfort vote (TCV)
During the questionnaire survey, a total of 643 valid questionnaires were collected, including 429 from patients and 214 from healthy individuals. Among the respondents, 333 were male and 310 were female. There were 274 young respondents, 310 middle-aged respondents, and 59 elderly respondents. The specific TSV and TCV voting results are shown in Fig. 2a–h.
Classified by health status, 176 patients (41.0%) voted for a neutral thermal sensation (TSV = 0). The number of individuals who felt “a little cold” (TSV= -1) and “a little warm” (TSV = + 1) were 15 (3.5%) and 204 (47.55%), respectively. Among the healthy individuals, 110 (51.4%) voted for a neutral thermal sensation (TSV = 0), while 69 (32.2%) and 35 (16.4%) felt “a little warm” (TSV = + 1) and “warm” (TSV = + 2), respectively. Among orthopedic patients, the proportion of individuals feeling thermally uncomfortable (TCV < 0) was significantly higher than that of healthy individuals, reaching 29.4% compared to only 3.3% in the healthy population.
When classified by gender, 45.6% of male respondents voted for a “neutral” thermal sensation (TSV = 0). The proportions of those feeling “a little warm” (TSV = + 1) and “warm” (TSV = + 2) were 43.5% and 10.5%, respectively. The proportion of those feeling “a little cold” (TSV= -1) was 1.8%. Among female respondents, 43.2% voted for a “neutral” thermal sensation (TSV = 0). The proportions of those feeling “a little warm” (TSV = + 1) and “warm” (TSV = + 2) were 42.9% and 10.9%, respectively. The proportion of those feeling “a little cold” (TSV= -1) was 2.9%. In terms of thermal comfort voting, 59.7% of males and 60.1% of females rated the thermal environment as moderate or above.
Classified by age, most respondents in all age groups considered the thermal environment to be “neutral” (TSV = 0) or “a little warm” (TSV = + 1). However, 6.7% of elderly respondents felt “a little cold” (TSV= -1), while only 1.6% and 2.9% of middle-aged and young respondents, respectively, felt the same.
The relationship between TSV and TCV in this study is shown in Fig. 2(i). A strong correlation (R^2 = 0.887) was observed between thermal sensation voting and thermal comfort voting in the collected survey questionnaires. When TSV = 0.21, individuals in the orthopedic ward indoor space exhibited the most comfortable state, located on the warm side of the thermal sensation scale. When TCV = 0, the corresponding TSV values were TSV= -0.23 on the cold side and TSV = + 0.64 on the warm side of the thermal sensation scale. This indicates that when TSV falls within the range of -0.23 to + 0.64, the average thermal comfort vote is greater than 0, and individuals in the orthopedic ward indoor treatment space feel comfortable.


Correlation analysis and voting patterns of TSV and TCV among respondents.
Correlation analysis between environmental physical parameters, physiological parameters, and thermal sensation
Studies have shown that the main factors influencing human thermal comfort are air temperature (\(\:{T}_{a}\)), relative humidity (RH), wind speed, globe temperature (\(\:{T}_{g}\)), metabolic rate, and clothing thermal resistance (Clo). Since TSV is an ordinal variable, this study employed Spearman’s correlation analysis to determine the correlation between respondents’ thermal sensation and various factors. The analysis results are presented in Table 4. The results indicate that \(\:{T}_{a}\) and \(\:{T}_{g}\) are the most significant factors influencing respondents’ thermal sensation, with correlation coefficients of R^2 = 0.575** for \(\:{T}_{a}\) and TSV, and R^2 = 0.427** for \(\:{T}_{g}\) and TSV. The correlation coefficient between relative humidity (RH) and TSV is R^2= -0.058**, indicating that RH has the least impact on respondents’ thermal sensation voting.
Thermal benchmark
Neutral SET*
During the study, Spearman’s correlation analysis was employed to analyze the correlation between respondents’ thermal sensation votes (TSV) and the thermal index standard effective temperature (SET), as shown in Fig. 3. The analysis results showed a significant correlation between the two (R^2 = 0.12**). Consequently, we calculated the weighted average TSV corresponding to each 1 °C increment of SET using a linear model. To mitigate the influence of outlier data, we set the minimum sample size for each 1 °C SET* interval group to 3, meaning that data samples with only one or two observations in a 1 °C SET* interval group were excluded due to their lack of representativeness.
-
The linear regression equation between the mean TSV (MTSV) and SET* during the survey period is as follows:
The slope of the regression equation is 0.10. Substituting MTSV = 0 into Eq. (2), the neutral SET* for the indoor diagnostic and treatment space of the Orthopedics Department at the North Campus of Xi’an Honghui Hospital in spring is calculated to be 17.9 °C. Studies have shown that the neutral temperature range is defined as the temperature range where MTSV falls within the interval of -0.5 to + 0.5. By substituting MTSV = + 0.5 and MTSV = -0.5 into Eq. (2), respectively, the range of NSET* for the indoor diagnostic and treatment space of the hospital’s Orthopedics Department is obtained as 13.0 °C to 22.73 °C.

Correlation analysis chart between SET* and MTSV.
Thermal acceptability range (TAR)
According to the ASHRAE 55 standard, the thermal acceptability range refers to the temperature range that is acceptable to at least 80% (normal condition) or 90% (stringent condition) of the population under certain climatic conditions. In this study, the subjects are mainly orthopedic patients. To fully meet the thermal comfort needs of orthopedic patients in the hospital’s indoor environment, a stricter 90% acceptability level is adopted to determine the thermal acceptability range. In the study, we selected 1 °C intervals to calculate the weighted average percentage of thermal unacceptability corresponding to each SET* group and a quadratic polynomial were used for fitting. The results are shown in Fig. 4. Through calculation, it is found that the acceptable SET* range for 90% of people in the orthopedic indoor diagnostic and treatment space of Xi’an Honghui Hospital is 15.8 °C to 27.4 °C.

The relationship between the percentage of thermal unacceptability and SET*.
Preferred temperature
This study analyzed the temperature preference information obtained from the preliminary survey questionnaires using the probit regression model. The dataset was classified based on respondents’ thermal preference votes into three categories: “increase,” “unchanged,” and “decrease.” Subsequently, the “unchanged” data were randomly assigned to the “increase” and “decrease” data groups. It was found that the overall dataset still followed a normal distribution. Finally, the data was grouped by 1 °C SET* intervals and the percentages of “increase” and “decrease” within each group were calculated. The intersection point of the probit models for “increase” and “decrease” represents the preferred temperature. In this study, the preferred temperature in the orthopedic indoor diagnostic and treatment space of Xi’an Honghui Hospital was found to be 15.8 °C, as shown in Fig. 5.

Preferred thermal temperature.
PMV-PPD analysis
Predicted percentage of dissatisfied (PPD)
ISO 7730 recommends using the Predicted Percentage of Dissatisfied (PPD) to determine the percentage of people who are uncomfortable due to the thermal environment, with the value calculated using the PMV regression equation. Based on the above algorithm, the fitting Eq. 3 for PPD in the orthopedic diagnostic and treatment space of Xi’an Honghui Hospital is:
The Predicted Percentage of Dissatisfied (PPD) shows a strong correlation with MTSV (R2 = 0.885), as shown in Fig. 6.

MTSV与PPD.
PMV-PPD
Based on Professor Fanger’s PMV-PPD model, PMV values were calculated. According to ISO 7730, the PMV index should be within the range of -1 to + 1. The results show that 92.4% of the data falls within this range, as illustrated in Fig. 7. Table 5 presents the PMV and AMV data classified by gender, health status, age, and overall. It was found that the AMV of females is 0.62, with a PMV of 0.60, indicating a close approximation with an error of 0.02. For males, the error is 0.05. When classified by health status, patients have a PMV-AMV error of 0.03, while healthy individuals have virtually no error. In terms of age classification, the error between PMV and AMV is 0.03 for young people and 0.01 for both middle-aged and elderly individuals, indicating relatively small errors.

Distribution of PMV Values.
Analysis of thermal comfort differences among respondents with different health status, gender, and age
Health status
During the questionnaire survey, a total of 429 questionnaires were collected from respondents with orthopedic diseases, and 214 feedbacks were received from healthy individuals. Among the patients, 176 people voted for a neutral thermal sensation (TSV = 0), accounting for 41.0%. There were 15 people who felt “a little cold” (TSV=-1) and 204 people who felt “a little hot” (TSV = + 1), accounting for 3.5% and 47.5% respectively. Among the healthy individuals, 110 people voted for a neutral thermal sensation (TSV = 0), accounting for 51.4%. There were 69 people who felt “a little hot” (TSV = + 1) and 35 people who felt “hot” (TSV = + 2), accounting for 32.2% and 16.4% respectively.
There are differences in thermal perception among respondents with different health conditions. We divided the respondents into two categories: those with orthopedic diseases and healthy individuals. Spearman’s correlation analysis was used to study the relationship between thermal sensation votes (TSV) and the thermal index SET* among respondents with different health conditions. The results showed that there was a significant correlation between TSV and SET* among respondents with different health conditions (orthopedic patients: 0.573; healthy individuals: 0.612). We performed linear fitting of MTSV and SET* for the two groups of respondents with different health conditions, as shown in Fig. 8. The regression equation slope for healthy individuals was 1.42, with a neutral SET* of 21.7 °C; while the regression equation slope for orthopedic patients was 0.09, with a neutral SET* of 17.7 °C. In the equation, y represents MTSV, and x represents SET*.
The linear regression equations for SET* and MTSV among respondents with different health conditions are represented as Eqs. (4) and (5). By substituting MTSV = 0 and MTSV = ± 0.5 into these equations, the neutral SET* and the range of neutral SET* for respondents with different health conditions were obtained, as shown in Table 6.

Correlation between SET* and MTSV for respondents with different health conditions.
Gender differences
Among the respondents, there were 333 males and 310 females. Among the males, 152 voted for a neutral thermal sensation (TSV = 0), accounting for 45.5%. A total of 175 males felt the indoor environment was on the warm side, accounting for 52.5%, with 140 feeling “a little hot” (TSV = + 1) and 35 feeling “hot” (TSV = + 2). Only 6 males felt “a little cold” (TSV=-1). Among the females, 123 voted for a “neutral” thermal sensation (TSV = 0), accounting for 36.9%. There were 133 and 34 females who felt “a little hot” (TSV = + 1) and “hot” (TSV = + 2) respectively, while 20 females felt “a little cold”.
There are differences in thermal perception among respondents of different genders. We adopted Spearman’s correlation analysis to study the correlation between thermal sensation votes (TSV) and the thermal index SET* among respondents of different genders. The results showed that there was a significant correlation between TSV and SET* among respondents of different genders (males: 0.667; females: 0.636). We performed linear fitting of MTSV and SET* for the two groups of respondents with different genders, as shown in Fig. 9. The regression equation slope for males was 0.08, with a neutral SET* of 16.7 °C; while the regression equation slope for females was 0.07, with a neutral SET* of 14.6 °C. In the equation, y represents MTSV, and x represents SET*.
The linear regression equations for SET* and MTSV among respondents of different genders are represented as Eqs. (6) and (7). By substituting MTSV = 0 and MTSV = ± 0.5 into these equations, the neutral SET* and the range of neutral SET* for respondents of different genders were obtained, as shown in Table 7. It was found that both the neutral SET* and the upper and lower limits of the neutral SET* range were lower for females compared to males, indicating that males have stronger tolerance in relatively warm environments compared to females.

Correlation analysis diagram between SET* and MTSV for males and females.
Age differences
The surveyed population included 4 minors, 270 young adults aged 18–40, accounting for 42.6%; 310 middle-aged individuals aged 41–60, accounting for 48.2%; and 59 elderly individuals over 60 years old, accounting for 8.9%. Due to differences in thermal perception among respondents of different ages, we divided the respondents into three categories: young, middle-aged, and elderly. We employed Spearman’s correlation analysis to study the correlation between thermal sensation votes (TSV) and the thermal index SET* among respondents of different age groups. The results showed that there was a significant correlation between TSV and SET* among respondents of different age groups (young: 0.867; middle-aged: 0.618; elderly: 0.353**). We performed linear fitting of MTSV and SET* for the three groups of respondents of different age groups, as shown in Fig. 10. The regression equation slope for the young group was 0.06, with a neutral SET* of 15.2 °C; the regression equation slope for the middle-aged group was 0.05, with a neutral SET* of 12.4 °C; and the regression equation slope for the elderly group was 0.05, with a neutral SET* of 13.6 °C. In the equation, y represents MTSV, and x represents SET*.
The linear regression equations for SET* and MTSV among respondents of different age groups are represented as Eqs. (8), (9), and (10). By substituting MTSV = 0 and MTSV = ± 0.5 into these equations, the neutral SET* and the range of neutral SET* for respondents of different age groups were obtained, as shown in Table 8. The lower limit of the neutral SET* for the youth group is significantly higher than that for the middle-aged and elderly groups. This is attributed to the stronger sensitivity of young people to temperature and their greater ease in perceiving the cool environment in spring. As age increases, the sensitivity to temperature gradually decreases for the middle-aged and elderly, resulting in a significantly larger range of neutral SET* compared to the youth group. Consequently, the middle-aged and elderly have stronger adaptability to thermal environments than the youth.

Correlation analysis of SET* and MTSV based on age factors.
Preference of meteorological factors
A total of 643 valid questionnaires were collected during the survey process. Figure 11 shows the preferences of all respondents for the four meteorological factors. Among the respondents, nearly 50% expected the temperature to decrease, while only 2% expected the temperature to increase. The overall results indicate that a cool temperature is more popular in the indoor diagnosis and treatment space of the hospital.
Due to the relatively complex architectural structure of the Northern Campus of Xi’an Honghui Hospital, which was selected as the survey ___location, it is not conducive to air flow. In the survey on wind speed expectations, no respondents expected the wind speed to decrease, but at the same time, nearly 90% of respondents said they expected the wind speed to remain unchanged.

Data chart of respondents’ preferences for meteorological factors.
Gender factor influence
Studies have shown that gender factors can affect people’s preferences for meteorological factors. In this study, the collected preferences for meteorological factors were classified by gender, and the specific data are shown in Fig. 12.
In terms of air temperature preferences, women and men share similar preferences. The proportion of men who expect the temperature to remain unchanged is 52.6%, slightly higher than the 49.7% of women, indicating that men have slightly higher adaptability to warmer environments than women. However, both men and women have nearly 50% of respondents expressing their desire for the temperature to decrease, both preferring a cooler indoor hospital environment.
In the study of relative humidity preferences, nearly 60% of both men and women respondents indicated their preference for the relative humidity to remain unchanged. The proportion of women who hope for the humidity to increase, at 30%, is higher than the 26% of men, indicating that women prefer a more humid indoor hospital environment compared to men.

Data chart of meteorological factor preferences classified by gender.
Impact of health factors
To investigate the influence of health factors on respondents’ preferences for meteorological factors, respondents were classified based on their health status and the data on meteorological factor preferences are presented in Fig. 13. Both healthy individuals and orthopedic patients have nearly 50% of respondents expressing their desire for no change in temperature. However, a significantly smaller proportion of healthy individuals compared to orthopedic patients expect a change in temperature. Among healthy individuals, 43% expect the temperature to decrease, while 49% of orthopedic patients prefer a cooler indoor space.
In terms of preferences for changes in relative humidity and wind speed, healthy individuals and orthopedic patients show similar expectations. When it comes to solar radiation preferences, healthy individuals have more diverse expectations for changes compared to orthopedic patients. While 75% of orthopedic patients indicate their preference for no change in solar radiation intensity, only 53% of healthy individuals express the same desire. Orthopedic patients, who spend longer periods indoors compared to healthy individuals, are less sensitive to changes in solar radiation intensity and have weaker expectations for such changes than healthy individuals.

Data chart of meteorological factor preferences classified by health status.
Impact of age factors
Based on the survey results, Fig. 14 presents the statistical data on the preferences of respondents of different ages for air temperature, relative humidity, wind speed, and solar radiation. Both the elderly and middle-aged populations have more than 50% of respondents expecting changes in indoor air temperature, while the younger population is relatively satisfied with indoor temperatures and has a higher acceptance of relatively warmer indoor thermal environments.
Age factors have a more pronounced impact on respondents’ preferences for relative humidity. Among them, the proportion of elderly respondents expecting the relative humidity to decrease reaches 16%, and the proportion expecting the humidity to increase reaches 29%, both higher than those of the young (7%, 27%) and middle-aged (7%, 23%) populations. The preferences of respondents for wind speed and solar radiation are less affected by age, but the proportion of elderly respondents who wish for an increase in solar radiation is 32%, significantly higher than the 19% and 18% of young and middle-aged respondents, respectively, indicating that the elderly prefer brighter sunshine.

Data chart of meteorological factor preferences classified by age factors.
Thermal environment improvement strategies
This study collected a total of 643 sets of valid data. Only 3.8% of respondents considered the indoor diagnostic and treatment spaces in their hospitals unacceptable, while the vast majority found the indoor physical environment acceptable. Temperature was identified as the most critical factor affecting comfort by 56.3% of respondents, followed by sound at 23.9%. Only 11.9% and 7.6% of respondents considered relative humidity and wind speed, respectively, as key factors influencing their comfort. The survey was conducted during the transitional spring season, with significant fluctuations in outdoor average temperatures. During the survey period, the average indoor temperature in the waiting area exceeded 24 °C, and that in the ward area exceeded 26 °C. More than half of the respondents perceived the indoor environment as relatively warm and expressed a desire for thermal environment improvement. According to the “Code for Design of Heating, Ventilation and Air Conditioning of Civil Buildings” (GB50736-2012), the recommended indoor thermal comfort range for hospital spaces during the summer is 24–26 °C for Level I and 26–28 °C for Level II. However, as the survey was conducted during the transitional season, the average clothing insulation worn by respondents, at 0.613 Clo, was significantly higher than the average summer clothing insulation of 0.3 Clo, necessitating a corresponding reduction in the comfortable indoor air temperature range for hospital spaces. According to hospital building standards, the recommended indoor temperature range is 18–22 °C.
Inpatient department
(1) The indoor public spaces of the orthopedic inpatient department can be improved by increasing the number of operable windows or the opening area of existing windows to enhance indoor air circulation and improve the efficiency of indoor-outdoor air exchange.
(2) Sunshades should be installed on windows. When indoor air temperature is high and outdoor solar radiation intensity is strong, the use of sunshades can effectively reduce the inflow of outdoor heat.
(3) The orthopedic inpatient department’s ward area can grant early access to central air conditioning, allowing patients and their families to proactively adjust indoor temperature and ventilation. During the field research period, the hospital’s central air conditioning was activated after May 1st, and during the survey period, the air conditioning in the wards only had ventilation functions.
(4) The control system of air conditioners beside the beds should be improved, with the addition of smart voice control systems. Due to orthopedic patients’ limited mobility, they often find it difficult to adjust the indoor thermal environment using the air conditioning system without family members present. The addition of a smart voice control system can effectively address this dilemma by allowing patients with limited mobility to adjust the indoor thermal environment.
Waiting area
The waiting area is located on the first floor of the hospital and has significantly more open doors and windows than the inpatient department, resulting in significantly better ventilation. However, the population density in the waiting area is significantly higher than that in the inpatient ward, and the average activity intensity of respondents is 1.07 met, significantly higher than the 0.89 met of the inpatient department.
(1) The thermal environment of the waiting area can be improved by planting vines such as ivy on the exterior walls to enhance the microclimate of the building’s facade. Greenery not only improves the aesthetics of the walls but also effectively blocks heat in summer without hindering heat transfer in winter, providing shade and cooling during high temperatures.
(2) To improve indoor air circulation and promote heat transfer in the outpatient department, where the space is relatively enclosed and the first-floor hospital structure is complex with multiple corridors affecting air flow; only one entrance and exit connect to the outside for air exchange. Additional operable windows can be installed in partitioned spaces to facilitate air circulation and thus improve the thermal environment in the outpatient area.
(3) To enhance the indoor thermal environment of the outpatient space, introduce moderate greenery into the waiting area. Green plants absorb heat from indoor spaces through transpiration, helping to reduce the temperature in the waiting area. Additionally, green plants release oxygen through photosynthesis, improving indoor air quality.
(4) Improve the selection of flooring materials and the materials and layout of seating. Choose flooring materials with good heat dissipation properties, such as marble, and avoid using materials with high thermal resistance like carpets, which can increase indoor heat. For seating, opt for materials like mesh fabric and linen that are breathable and have excellent heat dissipation properties. Arrange seats with appropriate spacing to ensure air circulation and heat dissipation efficiency.
Discussion
Neutral SET* and neutral SET* range
By comparing this study with other thermal comfort research (Table 9), we found that Xi’an, the surveyed area, has an annual average temperature of 14.6 °C, which is similar to Chongqing’s 16.7 °C. However, the neutral SET* in Chongqing is 3.4 °C higher than that in Xi’an. This indicates that the mixed population in Xi’an is more adapted to relatively cooler thermal environments compared to the mixed population in Chongqing, which demonstrates better tolerance to hot environments.
The neutral SET* in Guangzhou, China, and Bangkok, Thailand, are respectively 7.4 °C and 7.3 °C higher than that in Xi’an. The significant differences in neutral SET* between Guangzhou and Xi’an, as well as Bangkok and Xi’an, can be attributed to their distinct climatic regions. Guangzhou experiences a warm and rainy humid climate with consistently high air temperatures throughout the year, and the local population has adapted to the hot environment, developing strong heat tolerance. Bangkok, on the other hand, experiences high temperatures year-round with rainfall divided into wet and dry seasons, concentrated mainly in the summer. The consistently high temperatures in Guangzhou and Bangkok are the primary reasons for the significant differences in neutral SET* compared to Xi’an. Additionally, differences in the research subjects can also contribute to variations in neutral SET*. The study conducted in Guangzhou targeted pregnant women, while Xi’an’s study involved a mixed population, leading to potentially different thermal perceptions between the two groups.
The neutral SET* range in this study is 13.0 ~ 22.73 °C, which differs significantly from the results of similar studies conducted by Constantinos15 and those in Guangzhou, Chongqing, and Tehran listed in Table 10. We believe that there are two main reasons for this:
(1) The timing of the survey differs. The relevant studies in Guangzhou, Chongqing, and Tehran were conducted during the summer, while this study was conducted in the spring. During the survey period, the average clothing insulation of the respondents in this study was 0.613 Clo, which is much higher than the average clothing insulation level in summer (0.3 Clo). The lower clothing insulation value in summer allows respondents in these three locations to have better tolerance in hot environments, resulting in significantly higher upper and lower limits of their neutral SET* range compared to this study.
(2) Guangzhou and Chongqing are located in different climatic zones from Xi’an. Guangzhou has relatively high temperatures throughout the year, and local residents have lived in hot environments for a long time, developing better adaptability to hot environments, with an overall higher neutral SET* range compared to Xi’an. Chongqing is located in a warm and rainy humid climate zone, with relative humidity significantly higher than Xi’an throughout the year. In summer, it is hot and humid, making it difficult for sweat to evaporate from the skin surface. Local residents who have been exposed to such hot and humid environments for a long time have a higher acceptance of high temperatures compared to Xi’an residents.
PMV and thermal acceptability range
This study found that the predicted percentage of dissatisfaction (PPD) had a strong correlation with the thermal sensation vote (TSV), which was consistent with the results of F. Azizpour’s study18,23,24,25,26. However, there was no significant difference between the predicted mean vote (PMV) and the actual mean vote (AMV), which was consistent with the results of Jan’s study19. By comparing with similar studies, we found that the thermal acceptability range of mixed populations in subtropical hospitals was the highest. The reason may be that the average annual temperature in this region is relatively high, and local residents have better heat tolerance after long-term thermal adaptation. Compared with Xi’an, which has a higher average altitude, the survey subjects in the two studies were mixed populations and medical staff, respectively, with different thermal environment requirements. Medical staffs have higher requirements for thermal comfort in the working environment, so their acceptable range is smaller. To improve the indoor orthopedic treatment spaces in hospitals, architectural design should consider the thermal environment from three aspects: material selection, auxiliary artificial facilities, and plant cultivation, in order to provide a more comfortable thermal environment for users. Planting seasonal plants such as ivy on the exterior walls, cultivating plants with strong transpiration capabilities indoors, and using materials with good heat dissipation properties, such as marble, for surface facilities can effectively enhance the indoor thermal environment.
Regarding relative humidity, more than 60% of respondents hoped that it would remain unchanged. Considering the climatic characteristics of Xi’an, local residents have lived in a relatively dry environment for a long time compared to residents in the southeast coastal areas. Therefore, residents in Xi’an showed a clear preference for dryness over humidity compared to residents in the southeast coastal areas.
Thermal preference vote (TPV)
In this study, it was found that, compared to males; changes in solar radiation intensity were the main meteorological factor affecting females’ thermal perception in the orthopedic ward area of hospitals in spring, with a significantly higher proportion than males. Women, compared to men, prefer cooler, more humid indoor environments with lower solar radiation intensity. Orthopedic patients, compared to healthy individuals, show significant differences in their preferences for temperature and solar radiation. Elderly people have stricter requirements for indoor humidity and, compared to younger and middle-aged individuals, prefer brighter sunlight. In the evaluation of thermal comfort in hospitals, we should focus on factors such as gender and age, which is consistent with the results of S. Del Ferraro’s study25. This study found that gender had a strong influence on the preference for solar radiation, indicating that female respondents had stricter expectations for the solar radiation intensity in their desired environment, while males were more tolerant of the solar radiation intensity in the environment11,27,28. Most of the male and female respondents expressed a desire for the solar radiation intensity to remain unchanged, indicating that the current indoor solar radiation intensity meets the needs of most people29,30.
Through field research, we found that most elderly people who desired changes in humidity had some chronic diseases, and changes in relative humidity could affect their perception of pain. Therefore, the elderly were more sensitive to changes in humidity, and their humidity expectations varied. When adjusting the indoor humidity environment, it should be regulated in different zones.
Innovations
The present paper features three main innovations as follows:
(1) The experimental time was selected during the transitional season of spring. Existing research on thermal comfort primarily focuses on winter and summer, with a lack of corresponding studies on the transitional seasons of spring and autumn. Although spring and autumn are relatively more comfortable compared to winter and summer, they still pose various climatic issues that need to be addressed urgently.
(2) Orthopedic patients were chosen as the primary subject of study in this paper. Due to pain, limited mobility, and other factors, orthopedic patients have more specific and stringent thermal environment needs compared to healthy individuals. Existing research primarily focuses on thermal comfort for all patient groups, with few studies specifically targeting orthopedic patients.
(3) The study was conducted at the Northern Campus of Xi’an Honghui Hospital, located in a cold region of China. Current research on thermal comfort in hospital spaces for patients is concentrated in economically developed areas such as the southeast coast, with fewer studies in cold regions and a lack of relevant datasets.
Limitations and future work
This study has certain limitations, mainly manifested in the following points:
(1) The study did not consider individual differences such as height, weight, and metabolic activities, which may have an impact on thermal comfort in orthopedic indoor treatment spaces at hospitals. These individual factors could be significant in influencing indoor thermal comfort and should be further explored and analyzed in future research.
(2) When providing strategies for enhancing the thermal environment design, there is a lack of data information on the practical application of relevant measures in the Xi’an area. In the future, we hope to continuously track the improvement of the indoor thermal environment, which can provide more precise data support and theoretical basis for the design of orthopedic indoor treatment spaces in hospitals.
Conclusion
This study mainly adopts the methods of field measurement and questionnaire survey to investigate the thermal perception of people in the orthopedic waiting area and ward area of the Northern Hospital District of Xi’an Honghui Hospital. The thermal comfort evaluation of respondents in the typical indoor space of the orthopedic department of the hospital was collected through questionnaires. Based on the collected thermal comfort evaluation and measured physical environment data of the indoor diagnosis and treatment space of the orthopedic department of the hospital, the thermal environment of the indoor diagnosis and treatment space of the hospital was further analyzed, and the design improvement strategies of the thermal environment of the indoor diagnosis and treatment space of the hospital were proposed. The main conclusions are as follows:
(1) In the transitional season of spring, The results indicate that, 92.3% of respondents considered the thermal environment of the indoor diagnosis and treatment space of the orthopedic department of the hospital to be acceptable (-1 ≤ TSV ≤ + 1). However, 42.5% of respondents felt that the indoor thermal environment was “a little warm” (TSV = + 1).
(2) In spring, most respondents voted for “neutral” or “a little warm” for thermal sensation, accounting for 92.3%. It was found that there was a strong correlation between the thermal comfort vote (TCV) and the thermal sensation vote (TSV) (R2 = 0.887). When TSV = + 0.21, people in the indoor diagnosis and treatment space of the orthopedic department of the hospital reached the most comfortable state. When TSV = -0.23 and TSV = + 0.64, TCV = 0, within the range of -0.23 to + 0.64 for TSV, the corresponding average TCV was greater than 0, and people in the indoor diagnosis and treatment space of the orthopedic department of the hospital felt comfortable.
(3) Ta (R2 = 0.575) and Tg (R2 = 0.427) were the most important factors affecting people’s thermal sensation in the indoor diagnosis and treatment space of the orthopedic department of the hospital. Met (R2= -0.013) had the least impact on thermal sensation.
(4) In the indoor diagnosis and treatment space of the orthopedic department of Xi’an Honghui Hospital, the neutral SET* was 17.9 °C. The neutral SET* range was 13.0 ~ 22.73 °C. The 90% SET* thermal acceptability range was 15.8 ~ 27.4 °C.
(5) Gender, age, and health status all affected thermal sensation. Orthopedic patients were more sensitive to changes in the thermal environment than healthy people and preferred cooler environments, with a neutral SET* of 17.7 °C compared to 21.7 °C for healthy people. Males had better adaptability to hot environments than females, with a neutral SET* of 16.7 °C compared to 14.6 °C for females. Young people were more sensitive to temperature changes than middle-aged and elderly people, with a neutral SET* range of 7.5 ~ 23 °C compared to 3.7 ~ 21.9 °C for middle-aged people and 3.8 ~ 23.2 °C for elderly people.
(6) 56.5% of respondents believed that temperature was the most important indicator affecting their evaluation of the indoor environment. Age, gender, and health status all influenced people’s preferences for meteorological factors.
Data availability
The datasets generated during and/or analyzed during the current study are publicly available. If you require the relevant data for this study, please contact the corresponding author Guangmeng Bian (Email: [email protected]).
Abbreviations
- AMV:
-
Actual mean vote
- ASHRAE:
-
American Society of Heating Refrigerating and Air conditioning Engineer
- Clo:
-
Clothing thermal resistance
- ISO:
-
International Organization for Standardization
- MET:
-
Metabolic equivalence of task
- MTSV:
-
Mean thermal sensation vote
- PPD:
-
Predict percentage of dissatisfactory
- PMV:
-
Predict mean vote
- RH:
-
Relative humidity
- TCV:
-
Thermal comfort vote
- TSV:
-
Thermal sensation vote
- SET:
-
Standard effective temperature
- Ta :
-
Air temperature
- Tg :
-
Globe temperature
- Tmrt :
-
Mean radiant temperature
- Va :
-
Wind speed
References
Guo, J. et al. Assessing the winter indoor environment with different comfort metrics in self-built houses of hot-humid areas: does undercooling matter for the elderly? Build. Environ. 263, 111871–111871 (2024).
Skoog, J., Fransson, N. & Jagemar, L. Thermal environment in Swedish hospitals summer and winter measurements. Energy Building. 37, 872–877 (2005).
Pourshaghaghy, A. & Omidvari, M. Examination of thermal comfort in a hospital using PMV–PPD model. Appl. Ergon. 43(6), 1089–1095 (2012).
Rupp, R. F., Vásquez, N. G. & Lamberts, R. A review of human thermal comfort in the built environment. Energy Build. 105, 178–205 (2015).
Buratti, C. & Ricciardi, P. Adaptive analysis of thermal comfort in university classrooms: correlation between experimental data and mathematical models. Build. Environ. 44(4), 674–687 (2008).
Nishi, Y. & Gagge, A. P. Effective temperature scale useful for hypobaric and hyperbaric environments. Aviat. Space Environ. Med. 48(2), 97–107 (1977).
Po, F. Assessment of Mans thermal comfort in practice. Br. J. Ind. Med. 30(4), 313–324 (1973).
Fantozzi, F. & Lamberti, G. Determination of thermal comfort in indoor sport facilities located in moderate environments: an overview. Atmosphere 10(12) (2019).
Humphreys, M. A. The optimum diameter for a Globe thermometer for use indoors*. Ann. Occup. Hyg. 20(2), 135–140 (1977).
Gagge, A. P. The war years at the aeromedical lab: Wright field (1941-46). Aviat. Space Environ. Med. 57(10 Pt 2), A1–A6 (1986).
Nilsson, H. O. Thermal comfort evaluation with virtual manikin methods. Build. Environ. 42(12), 4000–4005 (2006).
Hashiguchi, N. et al. Thermal environment and subjective responses of patients and staff in a hospital during winter. J. Physiol. Anthropol. Appl. Hum. Sci. 24(1), 111–115 (2005).
Skoog, J., Fransson, N. & Jagemar, L. Thermal environment in Swedish hospitals. Energy Build. 37(8), 872–877 (2004).
Hwang, R-L., Lin, T-P., Cheng, M. J. & Chien, J. H. Patient thermal comfort requirement for hospital environments in Taiwan. Build. Environ. 42, 2980–2987 (2007).
Balaras, C. A., Dascalaki, E. & Gaglia, A. HVAC and indoor thermal conditions in hospital operating rooms. Energy Build. 39(4), 454–470 (2006).
Mazzacane, S. A survey on the thermal conditions experienced by a surgical team. Indoor Built Environ. 16(2), 99–109 (2007).
Khodakarami, J. & Nasrollahi, N. Thermal comfort in hospitals - A literature review. Renew. Sustainable Energy Reviews. 16(6), 4071–4077 (2012).
Del Ferraro, S. et al. A field study on thermal comfort in an Italian hospital considering differences in gender and age. Appl. Ergon. 50, 177–184 (2015).
Verheyen, J. et al. Thermal comfort of patients: objective and subjective measurements in patient rooms of a Belgian healthcare facility. Build. Environ. 46(5), 1195–1204 (2010).
Derks, M. T. H. et al. Understanding thermal comfort perception of nurses in a hospital ward work environment. Build. Environ. 140, 119–127 (2018).
Khalid, W. et al. Investigation of comfort temperature and thermal adaptation for patients and visitors in Malaysian hospitals. Energy Build. 183, 484–499 (2018).
Sari-Sarraf, V. et al. Effects of carbohydrate beverage ingestion on the salivary IgA response to intermittent exercise in the heat. Int. J. Sports Med. 32(9), 659–665 (2011).
Azizpour, F. et al. Thermal comfort assessment of large-scale hospitals in tropical climates: A case study of university Kebangsaan Malaysia medical centre (UKMMC). Energy Build. 64, 317–322 (2013).
Yao, R., Li, B. & Liu, J. A theoretical adaptive model of thermal comfort – Adaptive predicted mean vote (aPMV). Build. Environ. 44(10), 2089–2096 (2009).
Binarti, F. et al. A review of outdoor thermal comfort indices and neutral ranges for hot-humid regions. Urban Clim. 31, 100531–100531 (2020).
Kristian, F. The indoor thermal comfort indexes PMV and PPD. Springer Int. Publishing 83–135 (2024).
Ukey, R. & Rai, A. C. Envelope retrofits for enhancing thermal comfort in detached houses in hot semi-arid Climatic conditions: A year-long monitoring and simulation study. Build. Environ. 257, 111536 (2024).
Xue, W. et al. Developing a novel personal thermoelectric comfort system for improving indoor occupant’s thermal comfort. J. Building Eng. 84, 108561 (2024).
Moldovan, F. & Moldovan, L. Indoor air quality in an orthopedic hospital from Romania. Toxics 12(11) (2024).
Wang, F. et al. Field Evaluation of Thermal Comfort and Indoor Environment Quality for a Hospital in a Hot and Humid Climate (HVAC&R Research, 2012).
Author information
Authors and Affiliations
Contributions
Tianyi Sun participated in the design and optimization of the research methodology, the collection and analysis of experimental data, and the verification of research data and results to draw scientific conclusions. She also conducted the visualization of the research results, creating charts to display the data, and translated the paper. Aimei Luo contributed to the revision of the paper, assisted in data analysis, and created charts to present the data. Yuhao Lu was involved in the experiments and wrote the first draft of the paper, including the introduction, methods, and results sections. Meng Zhen participated in the editing and review of the paper, providing suggestions for revisions. Yuanyuan Zhang was involved in the experimental design and editing of the paper, as well as giving suggestions for modifications. Guangmeng Bian provided guidance on the experimental methods, participated in the design and optimization of the research methods, directed the team’s work to ensure the research was conducted as planned, and reviewed and edited the final version of the paper, offering suggestions for revisions. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
All methods were implemented according to relevant guidelines and regulations, and achieved the desired effects. This research was approved by School of Architecture and Art, Hebei University of Architecture and Honghui Hospital Affiliated to Xi’an Jiaotong University. The ethical approval number for medical biological research is 202409043. Before conducting the experiment, the research team had informed participants that the experiment was anonymous and aiming at academic research. This study confirming that written informed consent was obtained from all subjects and/or their legal guardian(s).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Sun, T., Luo, A., Lu, Y. et al. Research on indoor thermal comfort of orthopedic patients in hospital. Sci Rep 15, 9053 (2025). https://doi.org/10.1038/s41598-025-93245-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-93245-5
