
Abstract
Drowning is a major global public health issue with marked variations in incidence, mortality, and disability-adjusted life years (DALYs) across regions, age groups, and sexes. Although previous studies have examined global trends in drowning, few have comprehensively analyzed regional and national disparities while addressing potential reporting biases and confounding factors. Data from the Global Burden of Disease (GBD) Study 2021, focusing on drowning-related incidence, death rates, and DALYs, and examined trends from 1990 to 2021 across various regions and countries. The study used age-standardized rates to assess trends and risk factors associated with drowning. In 2021, there were 856.1 thousand drowning cases globally, leading to 274.2 thousand deaths and 15.7 million DALYs. Age-standardized rates showed significant reductions since 1990: incidence decreased by 51.5% to 11.1, deaths by 60.9% to 3.6, and DALYs by 67.3% to 211.9. Solomon Islands, Belarus, and Ukraine had the highest incidence rates, while Nauru, Central African Republic, and Marshall Islands reported the highest death and DALYs rates. DALYs rates were highest in children aged 0–5 years and declined with age. A negative correlation was observed between SDI and DALYs rates. Key risk factors included occupational injuries (13.2%), high temperature (4.6%), and alcohol use (1.7%), while low temperature had a negative contribution (-10.6%). Despite reductions, drowning remains a major public health issue, especially in low-SDI countries. Targeted interventions addressing Occupational injuries, High temperature and Alcohol use are essential to further reduce drowning-related morbidity and mortality.
Similar content being viewed by others

Introduction
Drowning is a significant global public health concern, causing substantial mortality and morbidity worldwide1. It is not only a major cause of unintentional injury-related deaths but also contributes to long-term disability and socioeconomic burdens, particularly in low- and middle-income countries2. The Global Burden of Disease (GBD) study provides a comprehensive framework for assessing the burden of drowning across different regions and sociodemographic strata3. This study not only identifies disparities and tracks progress over time but also informs targeted interventions.
The magnitude and distribution of drowning-related health outcomes vary widely across regions, countries, and populations. Over the past three decades, significant efforts have been made to implement drowning prevention strategies. Earlier studies indicated a high burden of drowning, particularly in low-income regions, whereas the 2021 findings reflect substantial declines in drowning rates in high-income regions due to improvements in water safety infrastructure, public education, and swimming lessons1. However, regions such as Oceania and Sub-Saharan Africa still face high drowning burdens due to limited infrastructure and preventive strategies2. For instance, drowning disproportionately affects young children and individuals in lower socioeconomic settings, where access to preventive measures and emergency care may be limited3. Furthermore, factors such as occupational hazards, extreme weather conditions, and alcohol use exacerbate the risk in certain populations4. In addition to socioeconomic and environmental determinants, cultural factors play a crucial role in drowning risk. Cultural practices—such as norms around child supervision near water, traditional water-related recreational activities, and attitudes toward alcohol consumption—can significantly modulate exposure to drowning hazards. For instance, in certain regions, a cultural acceptance of unsupervised water play may contribute to the disproportionately high incidence among young children, while in others, gender roles influence the likelihood of engaging in risky water-based occupations. Recognizing these cultural nuances is essential for designing effective, community-specific interventions5,6.
Although significant progress has been made in reducing the global burden of drowning over the past three decades, marked regional and demographic disparities persist. East Asia has seen a larger-than-expected reduction in drowning rates, which can be attributed to several factors: the introduction of public health campaigns promoting water safety, substantial improvements in water infrastructure, and government policies mandating swimming lessons in schools. In particular, the successful implementation of national swimming programs in China, coupled with improvements in safety regulations and public awareness in countries like Japan and South Korea, has contributed to this reduction. Further investigation into the role of socioeconomic development and urbanization in these trends would provide valuable insights into the key drivers of change7. Understanding the evolving trends in incidence, mortality, and disability-adjusted life years (DALYs) attributable to drowning is critical to addressing these inequities8. Additionally, examining the association between drowning burden and the sociodemographic index (SDI), as well as the role of specific risk factors, can guide evidence-based policies and interventions9. In addition to socioeconomic and environmental determinants, cultural factors—such as child supervision practices and attitudes toward alcohol consumption—play crucial roles in shaping drowning risks.
This study aims to provide a detailed analysis of the burden of drowning from 1990 to 2021, using data from the GBD 2021 study. By quantifying trends in incidence, mortality, and DALYs across different regions, age groups, and sexes, and by exploring their relationship with SDI, this study seeks to inform strategies to mitigate the global burden of drowning and promote health equity.
Furthermore, an analysis of how the GBD methodology has evolved would strengthen the understanding of progress and gaps in drowning prevention strategies. Hypothesis-driven questions, such as: "What role have global health initiatives played in mitigating drowning in vulnerable regions?" could provide a clear direction for further investigation into the effectiveness of these strategies.
Methods
Data source
The Global Burden of Disease 2021 study estimated the burden of 376 diseases and injuries and 87 risk factors from 1990 to 2021 in 204 countries and territories and 21 regions. Detailed descriptions of the methodologies have been reported, and fatal and non-fatal estimates have been published (https://vizhub.healthdata.org/gbd-compare/ and https://ghdx.healthdata.org/gbd-results-tool).
Data analysis
Data on the incidence, deaths, and disability-adjusted life years (DALYs) for drowning, along with attributable risk factors, were obtained from the Global Burden of Disease (GBD) 2021 study, which covers 204 countries and territories over the period from 1990 to 2021. Estimates of incidence, deaths, and DALYs were calculated per 100,000 population, with corresponding 95% uncertainty intervals (UIs) derived from posterior distributions. These estimates ensure reliability by incorporating uncertainty and adjusting for incomplete or inconsistent reporting across regions. The statistical methods used in the analysis include Spearman’s rank correlation coefficients to assess the association between sociodemographic index (SDI) levels and age-standardized incidence rates (ASIR) and disability-adjusted life years (DALYs). Additionally, locally weighted scatterplot smoothing (LOWESS) curves were used to model the trends in drowning rates across different regions and SDI levels over time. In order to account for potential inconsistencies or biases in reporting drowning-related deaths across different countries, we performed sensitivity analyses and applied statistical adjustments to correct for incomplete or inconsistent reporting. All data management was performed using Microsoft Excel and R (version 4.4.1)10, and the figures were created using R (version 4.4.1). P-value of less than 0.05 was regarded as statistically significant.
Results
Global
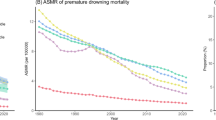
Level In 2021, 856.1 thousand (Table 1) incidence cases of drowning were reported globally, with an age-standardized point incidence of 11.1 per 100,000, a decrease of 51.5% since 1990. Drowning accounted for 274.2 thousands deaths in 2021, with an age-standardized rate of 3.6, a decrease of 60.9% since 1990. In 2021, the number of DALYs for drowning globally was 15.7 million, with an age-standardized rate of 211.9 DALYs per 100,000, a 67.3% decrease since 1990 (Table 1).
Regional level
In 2021, Eastern Europe (21.8), Central Asia (19.0), and East Asia (16.6) had the highest age-standardized point incidences for drowning (per 100,000) , whereas Central Sub-Saharan Africa (5.3), Eastern Sub-Saharan Africa (5.7) and Western Sub-Saharan Africa (5.7),had the lowest (Table 1). Oceania (8.4), Central Sub-Saharan Africa (6.1), and Caribbean (5.1) had the highest age-standardized death rates from drowning in 2021, with the lowest rates in Western Europe (0.6), Australasia (0.8), and High-income North America (1.0) (Table 1). In 2021, Oceania (520.7), Central Sub-Saharan Africa (386.1), and Caribbean (348.1) had the highest age-standardized DALYs rates (per 100,000) whereas Western Europe (29.3), Australasia (45.4), and High-income North America (61.2) had the lowest (Table 1). Figures S1-S3 show the age-standardized point incidence, death, and DALYs rates of drowning, respectively, by sex in 2021 for all regions in the Global Burden of Disease study. No region increased in the age-standardized point incidence of drowning, from 1990 to 2021,and the greatest decreases in East Asia (-57.0%), Eastern Europe (-56.7%) and Tropical Latin America (-56.5%) (Table 1). In the same period, all regions showed a decrease in the age-standardized death rates from drowning, with the largest decreases in East Asia (-73.6%), Southern Latin America (-67.2%), and Central Latin America (-65.5%) (Table 1).The age-standardized DALYs rates decreased in all regions from 1990 to 2021, with the largest decreases in East Asia (-79.7%), Central Europe (-69.5%) and Eastern Europe (-68.4%) (Table 1). Figures S1-S3 show the percentage change, from 1990 to 2021, in age-standardized point incidence, death, and DALYs rates for drowning by sex, respectively.
The number of incidence cases of drowning decreased from 1290.5 thousand in 1990 to 856.1 thousand in 2021. East Asia, South Asia, and Southeast Asia had the highest numbers of incident cases in 1990, whereas East Asia, South Asia, and Southeast Asia had the highest numbers in 2021 (table S1). The number of deaths caused by drowning decreased from 516.2 thousand in 1990 to 274.2 thousand in 2021, with East Asia, South Asia and Southeast Asia having the highest numbers of deaths in 2021 (table S2). The number of DALYs due to drowning decreased from 38.3 million in 1990 to 15.7 million in 2021, with East Asia, South Asia and Southeast Asia having the highest numbers of DALYs in 2021 (table S3).
National level
In 2021, the national age-standardized point incidence of drowning ranged from 4.5 to 40.6 cases per 100,000. Solomon Islands (40.6), Republic of Belarus (28.5), and Ukraine (28.4) had the highest age-standardized point incidence of drowning with Republic of Equatorial Guinea (4.5), United Kingdom of Great Britain and Northern Ireland (4.5, and Republic of Italy (4.5) having the lowest estimates (Fig. 1 and table S1). The national age-standardized death rates for drowning in 2021 varied from 0 to 14.4 deaths per 100,000. The highest rates were seen in Republic of Nauru (14.4), Central African Republic (12.0), and Republic of the Marshall Islands (11.8), whereas the lowest rates were found in Principality of Andorra (0), Republic of San Marino (0.2), and Grand Duchy of Luxembourg (0.3) (fig S1 and table S2). In 2021 the national age-standardized DALYs rate of drowning ranged from 0.6 to 817.7 patients per 100,000. The highest rates were seen in Republic of Nauru (817.7), Central African Republic (802.6), and Republic of Niue (801.5) (fig S2 and table S3).

Age standardised point incidence of drowning per 100 000 population in 2021, by country. Created by R (version 4.4.1), ggplot2 (version 3.5.1) [URL: https://ggplot2.tidyverse.org],sf(version1.0-20)[URL:https://r-spatial.github.io/sf/],tmaptools(version3.2)[URL:https://cran.r-project.org/web/packages/tmaptools/index.html],maps(version3.4.2.1)[URL: https://cran.r-project.org/web/packages/maps/index.html].
The percentage change in the age-standardized point incidence, from 1990 to 2021, differed noticeably between countries, with Republic of Vanuatu (15.5%), Kingdom of Lesotho (12.6%), Republic of the Marshall Islands (6.1%) having the largest increases. In contrast, Republic of Estonia (− 70.2%), Turkmenistan (− 67.3%), and Taiwan (Province of China) (− 67.1%) had the largest decreases (table S1) . Over the same period, Republic of Cabo Verde (89.6%), Kingdom of Lesotho (51.6%), and Republic of Zimbabwe (39.8%) had the largest increases in the age-standardized death rate, whereas the largest decreases were found in Republic of Estonia (− 83.5%), People’s Republic of Bangladesh (− 79.3%), and Taiwan (Province of China) (− 78.4%) (table S2). Republic of Niue (60.7%), Tokelau (60.3%), and Republic of Cabo Verde (56.2%) had the largest increases in age-standardized DALYs rate of drowning from 1990 to 2021. In contrast, the greatest decreases during the study period were found in Republic of Estonia (− 86.5%), Republic of Korea (− 86.0%), and Taiwan (Province of China) (− 82.9%) (table S3).
Age and sex patterns
In 2021, the global point incidence of drowning started to decrease in the 0–4 age group and peaked in 0–4 age group Similarly, the number of incident cases was highest in the 0–4 age group, but then decreased with increasing age. The number of incident cases of drowning was higher in women up to age 10–14 years, but drowning was more common in women older than 65 years (Fig. 2). In 2021, the global drowning death rate reached its highest level in 0–4 age group and was higher in men up to age 0–4 years, but drowning was more common in women older than 5 years. The number of deaths was highest in the 0- 4 age groups, for both sexes, after which the numbers decreased with increasing age. The number of deaths caused by drowning was higher in men aged up to 0–89 years (fig S6). In men, the global DALYs rate of drowning increased up to age 0–4 years and then decreased with advancing age, as well as women. Also, the number of DALYs peaked in the 0–4 age groups and was higher in men up to age 0–89 years. (fig S7).

Number of incident cases globally and incidence of drowning per 100 000 population, by age and sex in 2021. Lines indicate incident case with 95% uncertainty intervals for men and women.
Association with the sociodemographic index
At the regional level, we found a declined curve between the sociodemographic index and the age-standardized DALYs rate of drowning, from 1990 to 2021. The age-standardized DALYs rate decreased exponentially with increases in sociodemographic index, up to a sociodemographic index of about -0.7. East Asia, Central Sub − Saharan Africa, Southeast Asia, Oceania and Eastern Europe had higher than expected DALYs rates, based on their sociodemographic index11, from 1990 to 2021. In contrast, Eastern Sub − Saharan Africa, Western Sub − Saharan Africa, North Africa and Middle East, Southern Latin America , Central Latin America , Central Europe , Andean Latin America , Tropical Latin America and Western Europe had lower than expected burdens from 1990 to 2021 (Fig. 3).

Age standardised disability adjusted life year (DALY) rates of drowning for the 21 Global Burden of Disease regions by sociodemographic index, 1990–2021. Thirty-two points are plotted for each region and show the observed age standardised DALY rates from 1990 to 2021 for that region. Expected values, based on sociodemographic index and disease rates in all locations, are shown as a solid line.
At the country level, in 2021, the burden of drowning decreased with increasing socioeconomic development up to a sociodemographic index of about -0.56 (fig S3). Countries and territories such as Central African Republic, Republic of Nauru and Republic of Niue had much higher than expected burdens, whereas Luxembourg, San Marino and Andorra had much lower than expected burdens (fig S3).
Risk factors
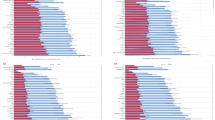
The proportion of DALYs due to drowning that were attributable to individual risk factors differed across the Global Burden of Disease regions12. Globally, occupational injuries (13.2%), high temperature (4.6%) and alcohol use (1.7%) had the highest contributions to DALYs due to drowning.In contrast,low temperature was showing a negative contribution (-10.6%). (Fig. 4). The proportion of DALYs due to drowning that were attributable to occupational injuries and alcohol use were higher in men, whereas the proportion attributed to high temperatures was more prominent among women. (fig S4 and fig S5).

Percentage of DALYs due to drowning attributable to risk factors for 21 GBD regions in 2021.
Discussion
This study offers an extensive analysis of the global, regional, and national drowning burdens from 1990 to 2021, utilizing data from the Global Burden of Disease (GBD) 2021 study. We systematically extracted drowning-related incidence, mortality, and disability-adjusted life years (DALYs) through standardized methodologies, including age-standardization, joinpoint regression, and uncertainty estimation via 95% confidence intervals. These validated techniques, as detailed in prior GBD studies3,7, ensure the reliability and precision of our findings. Key novel insights from this study include the identification of distinct age and sex-specific patterns, with the highest burden observed among children aged 0–4 years. Furthermore, we demonstrated an exponential decline in drowning DALYs with increasing Socio-Demographic Index (SDI), highlighting regions with disproportionately high or low burdens.
We conducted stratified analyses by geographical region, age group, sex, and SDI level. These subgroup analyses facilitated an understanding of variations in drowning trends and allowed us to identify significant differences across regions. For instance, Oceania and Central Sub-Saharan Africa consistently exhibited high drowning burdens, while Western Europe and high-income North America demonstrated significantly lower burdens. Moreover, joinpoint regression analysis confirmed that the observed declines in age-standardized drowning rates from 1990 to 2021 were statistically significant (p < 0.001), reinforcing our interpretation of these trends.
At the regional level, Eastern Europe, Central Asia, and East Asia reported the highest age-standardized incidence rates, whereas Oceania, Central Sub-Saharan Africa, and the Caribbean exhibited the highest death and DALYs rates. Stratified analyses revealed that although occupational injuries, high temperature, and alcohol use were key risk factors globally, their relative contributions varied by region. For instance, in low-income and high-temperature regions, occupational injuries and high ambient temperatures had a greater impact, while alcohol use was relatively more influential in high-SDI countries.Additionally, climate vulnerability plays a pivotal role—rising sea levels and extreme weather events such as floods and cyclones exacerbate drowning risks in island nations like the Solomon Islands and Nauru. In Sub-Saharan Africa, rapid urbanization coupled with insufficient water safety policies, especially in informal settlements, further intensifies drowning risks. These findings underscore the urgent need for targeted interventions addressing both infrastructure gaps and climate adaptation strategies13. In contrast, the low drowning burden observed in Western Europe and high-income North America reflects the success of comprehensive drowning prevention strategies, including public awareness campaigns, swimming education, and robust water safety infrastructure14. However, regions such as Eastern Europe and East Asia presented higher-than-expected drowning burdens, despite improved socioeconomic conditions. This phenomenon has been linked to lingering gaps in water safety regulations, alcohol misuse, and cultural practices surrounding water-related activities15.
At the national level, the Solomon Islands, Republic of Belarus, and Ukraine had the highest drowning incidences. In contrast, countries such as Nauru, the Central African Republic, and the Marshall Islands exhibited the highest death and DALYs rates. Notably, despite a significant inverse relationship between SDI and drowning burden, some high-SDI countries still experienced elevated drowning rates, possibly due to cultural practices and gaps in local water safety regulations.Island nations like the Solomon Islands and Nauru face elevated risks due to extensive exposure to open water and insufficient safety measures, while Belarus’s high rates are possibly associated with abundant inland water bodies and underdeveloped water safety policies. These findings highlight the importance of geographic, cultural, and socioeconomic determinants in shaping drowning risks16. Discrepancies in rapidly transitioning nations like the Republic of Korea and Taiwan also suggest that urbanization, public health initiatives, and cultural shifts may have contributed to more significant reductions in drowning burdens than expected17.
This study’s broader implications transcend statistical reporting. By elucidating the multifactorial determinants of drowning—including environmental, cultural, and socioeconomic factors—it offers a valuable evidence base for improving public health outcomes. Tailored interventions, as recommended herein, have the potential to significantly reduce drowning-related morbidity and mortality. Furthermore, the study’s rigorous methodological approach provides essential insights for international organizations and local governments aiming to allocate resources efficiently and implement prevention measures that are sensitive to regional and cultural contexts. This comprehensive approach is crucial in reducing health disparities and enhancing the overall well-being of populations globally.
Analysis by age and sex indicated that drowning incidents and DALYs peaked in children aged 0–4 years. While incident cases were higher in girls up to age 10–14 years, drowning deaths were predominantly observed in young boys, and in older age groups, the patterns reversed18. Overall, men exhibited higher drowning mortality up to age 89, whereas the highest DALYs were recorded in the 0–4 age group across both sexes. This is consistent with previous research, which attributes these trends to developmental immaturity, lack of supervision, and increased exposure to water hazards. Additionally, drowning remains notably more prevalent among men across all age groups, likely due to their greater engagement in high-risk activities and higher alcohol consumption, as observed in previous studies19. Notably, the higher burden seen among older women in certain regions warrants further exploration, as it may reflect region-specific gender roles and water-related activities.
In examining the association with SDI, our results reinforce earlier findings indicating an inverse relationship between drowning burden and socioeconomic development20. Countries with lower SDI scores, particularly in Sub-Saharan Africa and Oceania, exhibit persistently high drowning rates, while high-income regions with higher SDI scores report considerably lower burdens. This study also identifies regional outliers, such as Nauru and the Central African Republic, where disproportionately high drowning burdens exceed expectations based on SDI alone21. These findings underscore the necessity of considering non-SDI-related factors, including environmental, cultural, and policy influences. A robust negative correlation was observed between the Socio-Demographic Index (SDI) and drowning DALYs, although some high-SDI countries still experienced elevated drowning rates, likely due to cultural practices and local water safety policy gaps.
Regarding risk factors, our analysis confirms previous reports highlighting occupational injuries, high ambient temperatures, and alcohol consumption as major contributors to drowning-related DALYs. Climate change is expected to amplify the frequency and severity of extreme weather events, such as floods and hurricanes, which could significantly impact drowning rates. Coastal and low-lying areas, especially in Oceania and Sub-Saharan Africa, are at increased risk due to rising sea levels and more frequent storms. These regions may experience an exacerbation of drowning incidents as climate change contributes to higher water-related fatalities. Interestingly, low ambient temperatures appear to exert a protective effect, likely due to reduced participation in water-related activities during colder periods, highlighting the complex interplay between environmental conditions and drowning risk22. Furthermore, sex-specific differences were observed: while occupational injuries predominantly affect men, high temperatures appear to influence drowning rates more acutely among women.
Our analysis of data from 2019 to 2021 suggests that lockdown measures and movement restrictions during the COVID-19 pandemic were associated with a modest reduction in drowning incidents in some regions. However, the pandemic also induced economic downturns that may have indirectly influenced drowning risk factors, such as increased alcohol consumption, heightened occupational exposures, and deteriorations in mental health. Moreover, healthcare disruptions during the pandemic potentially affected emergency response times and drowning mortality rates.
This study calls for further exploration of sociocultural barriers to drowning prevention, including cultural attitudes toward water safety, risk perception, and gender norms. In many regions, traditional practices regarding child supervision near water or attitudes toward alcohol consumption during aquatic activities contribute to increased drowning risks. Gender norms also influence the likelihood of males and females engaging in high-risk water-based activities. For example, in certain cultures, men are more likely to engage in high-risk occupations like fishing, which increases their exposure to drowning hazards. Addressing these sociocultural factors is essential in designing effective prevention strategies23.
Public health implications
Beyond statistical reporting, the implications of our findings for public safety are profound. By identifying specific risk factors and vulnerable populations, our study provides a roadmap for policy-makers to design targeted interventions. Enhanced water safety infrastructure, community-based education, and stringent regulatory measures are essential for reducing drowning-related morbidity and mortality. These interventions not only improve water safety but also contribute significantly to overall public health enhancement.24,25,26:
-
Enhancement of Water Safety Infrastructure: Invest in community-level water safety measures, including barriers, life-saving equipment, and improved signage around water bodies.
-
Community-Based Education Programs: Design and implement culturally tailored water safety and swimming education programs, particularly targeting high-risk groups, such as young children and individuals in high-risk occupations.
-
Regulatory Measures: Enforce policies to control alcohol consumption near aquatic environments and mitigate occupational hazards in industries with significant water exposure.
-
Strengthening Surveillance Systems: Improve data collection and reporting mechanisms to ensure drowning incidences are accurately monitored, enabling timely and targeted public health responses.
These recommendations align with prior research and global guidelines1, aiming to reduce drowning burdens in both high- and low-SDI regions.
Strengths and limitations
This study boasts several strengths, including the use of comprehensive, standardized data from the GBD study, enabling a detailed analysis of drowning incidence, mortality, and DALYs across global, regional, and national levels over three decades27,28,29. The application of robust statistical methods and stratified subgroup analyses represents an innovative approach to contextualizing drowning burdens in relation to socioeconomic development30. The large temporal scope (1990–2021) and age- and sex-specific analyses further enhance the study’s validity. However, several limitations must be acknowledged. The reliance on GBD data may introduce biases due to variability in the quality and completeness of drowning-related reporting across countries and regions, potentially affecting the accuracy of estimates28. Furthermore, while the study identifies key risk factors, causal relationships remain unclear due to the observational nature of the data and the inability to account for all confounding variables31. The exclusion of detailed behavioral, environmental, and policy-related factors limits the contextual understanding of drowning risks. Lastly, the findings may not be fully generalizable to countries or communities with unique sociocultural and environmental contexts, emphasizing the need for further research to validate these results and address knowledge gaps32. These methodological refinements strengthen the reliability of our estimates despite potential reporting biases.
Future research
Future studies should focus on the mechanisms underlying regional and national disparities in drowning burden, particularly the roles of climate change, urbanization, and migration23. Improved surveillance and standardized data collection in low-resource settings are essential to refine estimates. Additionally, predictive models that integrate environmental and behavioral risk factors will be crucial for identifying high-risk populations early33. Evaluations of drowning prevention strategies, including community-based water safety programs and national policy interventions, are essential to sustaining progress in reducing drowning rates26,29. Lastly, further research should explore the sociocultural dynamics that influence drowning risks and prevention efforts26,27.Enhanced surveillance and standardized data collection in low-resource settings are essential. Predictive models incorporating environmental and behavioral risk factors may help identify high-risk populations early. Moreover, rigorous evaluations of community-based water safety programs and national policy interventions are warranted to sustain progress in drowning prevention.
Conclusions
Our findings confirm that drowning remains a multifaceted global public health challenge characterized by pronounced regional disparities, age- and sex-specific vulnerabilities, and an inverse relationship with socioeconomic development. The highest burden is observed among children under 5 years and in regions with limited water safety infrastructure, underscoring the need for comprehensive, context-specific interventions. Effective strategies—including community-based education, improved occupational safety regulations, and culturally sensitive public awareness campaigns—have the potential to significantly reduce drowning-related DALYs. This study provides a roadmap for targeted policies aimed at improving health outcomes across diverse societies, particularly in regions like the Solomon Islands and Nauru, where infrastructure improvements and public education could dramatically reduce drowning rates. Moreover, the findings highlight the critical role of cultural practices and socioeconomic factors in shaping drowning risks, emphasizing the need for a holistic, multi-sectoral approach that integrates structural interventions with behavior change initiatives to reduce global drowning burdens and ensure long-term public health benefits.
Data availability
The datasets analyzed during the current study are available in the IHME (the Institute for Health Metrics and Evaluation) Data ( http://ghdx.healthdata.org/gbd-results-tool ).
References
Global status report on drowning prevention 2024. Geneva: World Health Organization; 2024. Licence: CC BY-NC-SA 3.0 IGO. https://www.who.int/teams/social-determinants-of-health/safety-and-mobility/global-report-on-drowning-prevention, accessed 22 December 2024
Global drowning prevention. Adopted by the United Nations General Assembly, seventy-fifth session, resolution 75/273, 29 April 2021. New York (NY): United Nations; 2021 (https://documents.un.org/ doc/undoc/gen/n21/106/27/pdf/n2110627.pdf, accessed 22 September 2024)
Tan, H. et al. Changes in global burden of unintentional drowning from 1990 to 2019 and its association with social determinants of health: Findings from the global burden of disease study. BMJ Open 13(4), e070772. https://doi.org/10.1136/bmjopen-2022-070772 (2023).
Sindall, R., Mecrow, T. & Queiroga, A. C. Drowning risk and climate change: A state-of-the-art review. Inj. Prev. 28(2), 185–189. https://doi.org/10.1136/injuryprev-2021-044486 (2022).
Cenderadewi, M. & Franklin, R. C. Socio-ecological nature of drowning in low-and middle-income countries: A review to inform health promotion approaches. Int. J. Aquatic Res. Educ. https://doi.org/10.25035/ijare.12.02.06 (2020).
Fralick, M., Denny, C. J. & Redelmeier, D. A. Drowning and the influence of hot weather. PLoS ONE 8(7), e71689. https://doi.org/10.1371/journal.pone.0071689 (2013).
Zhu, W., He, X., San, R., Chen, N. & Han, T. Global, regional, and national drowning trends from 1990 to 2021: Results from the 2021 global burden of disease study. Acad. Emerg. Med. 28(11), 1290–1300. https://doi.org/10.1111/acem.15003 (2024).
Haagsma, J. A., Graetz, N. & Bolliger, I. The global burden of injury: Incidence, mortality, disability-adjusted life years and time trends from the global burden of disease study 2013. Injury. Prev. 22(1), 3–8. https://doi.org/10.1136/injuryprev-2015-041616 (2016).
Tan, H. et al. Change in global burden of unintentional drowning from 1990 to 2019 and its association with social determinants of health: findings from the global burden of disease study. BMJ Open 13(4), e070772. https://doi.org/10.1136/bmjopen-2022-070772 (2023).
Singh, A. V. et al. Investigating tattoo pigments composition with UV-Vis and FT-IR spectroscopy supported by chemometric modelling. Curr. Anal. Chem. 20, e15734110316443. https://doi.org/10.2174/0115734110316443240725051037 (2024).
Singh, A. V. et al. Sustainable bioinspired materials for regenerative medicine: balancing toxicology, environmental impact, and ethical considerations. Biomed. Mater. https://doi.org/10.1088/1748-605X/ad85bb (2024).
Chandrasekar, V., Mohammad, S., Aboumarzouk, O., Singh, A. V. & Dakua, S. P. Quantitative prediction of toxicological points of departure using two-stage machine learning models: A new approach methodology (NAM) for chemical risk assessment. J. Hazard Mater. https://doi.org/10.1016/j.jhazmat.2024.137071 (2025).
Franklin, R. C. et al. The burden of unintentional drowning: global, regional, and national estimates of mortality from the global burden of disease 2017 Study. Inj. Prev. https://doi.org/10.1136/injuryprev-2019-043484 (2020).
Peden, A. E., Franklin, R. C. & Leggat, P. A. Fatal intentional drowning in Australia: A systematic literature review of rates and risk factors. PLoS ONE 15(5), e0231861. https://doi.org/10.1371/journal.pone.0231861 (2020).
Jagnoor, J., Gupta, M., Christou, A. & Ivers, R. Challenges in documenting non-fatal drowning disability in Bangladesh: A community-based survey. Int. J. Environ. Res. Public Health. 18(18), 9738. https://doi.org/10.3390/ijerph18189738 (2021).
Moradi-Lakeh, M. et al. Trend of socio-demographic index and mortality estimates in Iran and its neighbors, 1990-2015; findings of the global burden of diseases 2015 study. Arch. Iran. Med. https://doi.org/10.34172/aim.2017.10 (2017).
Lin, Z. et al. Changes in global burden of unintentional drowning from 1990 to 2019 and its association with social determinants of health: Findings from the global burden of disease study 2019. BMJ Open 13(4), e070772. https://doi.org/10.1136/bmjopen-2022-070772 (2023).
Davies, M. T. & Duckett, M. E. A student’s introduction to global health. Springer International Publishing https://doi.org/10.1007/978-3-031-66563-9 (2024).
Cenderadewi, M., Franklin, R. C., Peden, A. E. & Devine, S. Fatal intentional drowning in Australia: A systematic review. PLoS ONE 15(5), e0231861. https://doi.org/10.1371/journal.pone.0231861 (2020).
Zhu, W. et al. Global, regional, and national drowning trends from 1990 to 2021: Results from the 2021 global burden of disease study. Academic Emerg. Med. 30(1), 37–48. https://doi.org/10.1111/acem.15003 (2023).
Leilei, D., Pengpeng, Y., Haagsma, J. A. & Ye, J. Injury mortality and DALY estimates in China, 1990–2017. Lancet Public Health. 4(9), e449–e459. https://doi.org/10.1016/S2468-2667(19)30125-2 (2019).
Li, C. et al. Global burden of all cause-specific injuries among children and adolescents from 1990 to 2019: A prospective cohort study. Int. J. Surg. 12(4), e560-569. https://doi.org/10.1097/JS9.0000000000001131 (2024).
Sindall, R. et al. Drowning risk and climate change: A state-of-the-art review. Inj. Prev. 28(2), 185–191. https://doi.org/10.1136/injuryprev-2021-044486 (2022).
Cenderadewi, M., Devine, S. G. & Peden, A. E. Burden of unintentional drowning in Indonesia: Insights from the global burden of disease study 2019. Inj. Prev. https://doi.org/10.1136/ip-2024-045274 (2024).
Peden, A. E., Mason, H. M., King, J. C. & Franklin, R. C. Examining the relationship between heatwaves and fatal drowning: a case study from Queensland Australia. Inj. Prev. 30(1), 7–13. https://doi.org/10.1136/ip-2023-044938 (2024).
Tian, M. et al. Burden of unintentional drowning in China from 1990 to 2019: Findings from the global burden of disease 2019 study. Inj. Prev. https://doi.org/10.1136/ip-2023-045089 (2024).
Jagnoor J, Peden AE. Injuries as a global health risk factor: Causes, burden, and prevention. In handbook of global health. Springer https://doi.org/10.1007/978-3-030-45009-0_41 2021
Guevarra, J. P., Peden, A. E., Orbillo, L. L. & Uy, M. R. S. Z. Preventing child drowning in the Philippines: The need to address the determinants of health. Children 8(1), 29. https://doi.org/10.3390/children8010029 (2021).
Gupta, M., Christou, A. & Ivers, R. Q. Challenges in documenting non-fatal drowning disability in Bangladesh: A community-based survey. Int. J. Environ. Res. Public Health. 18(18), 9738. https://doi.org/10.3390/ijerph18189738 (2021).
Willcox-Pidgeon, S. M., Franklin, R. C., Leggat, P. A. & Devine, S. Identifying a gap in drowning prevention: high-risk populations. Inj. Prev. 26(3), 279–288. https://doi.org/10.1136/injuryprev-2019-043432 (2020).
Hidden depths: the global investment case for drowning prevention. Geneva: World Health Organization; 2023 (https://iris.who.int/bitstream/ handle/10665/371701/9789240077720-eng. pdf?sequence=1, accessed 30 September 2024).
Li C, Jiao J, Hua G, et al. A systematic analysis of DALYs for injury burden: Insights into drowning trends from the Global Burden of Disease study. Injury Epidemiology. https://doi.org/10.1186/s40621-024-00467-3.
Peden, A. E. et al. Drowning prevention challenges and opportunities: an exploratory study of perspectives of delegates from ASEAN nations. PLoS ONE 19(6), e0304138. https://doi.org/10.1371/journal.pone.0304138 (2024).
Acknowledgements
The authors highly appreciate the great work by the Global Burden of Disease Study 2021 collaborators.
Author information
Authors and Affiliations
Contributions
Zhongyong Xie designed the study. Zhongyong Xie, Wenmin Luo,Wei Du collected and analyzed the data. Zhongyong Xie, Wenmin Luo,Wei Du wrote the manuscript. Zhongyong Xie, Zhihua Huang,Qifeng Ran edited the manuscript and provided valuable suggestions for study design and data analysis. Zhongyong Xie supervised the project. All authors have approved the final version of this paper.
Corresponding author
Ethics declarations
Competing interest
The authors declare no competing interests.
Ethical approval
The data in this study were anonymized before its use. All methods were carried out in accordance with relevant guidelines and regulations.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xie, Z., Huang, Z., Ran, Q. et al. Global burden of drowning and risk factors across 204 countries from 1990 to 2021. Sci Rep 15, 10916 (2025). https://doi.org/10.1038/s41598-025-95486-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-95486-w
