
Abstract
Prostate smooth muscle contraction is central in treatment of voiding symptoms in benign prostatic hyperplasia (BPH). Tissues from transurethral resection of the prostate (TURP) and radical prostatectomy (RP) for prostate cancer are widely used to study contractions. However, findings are limited by traumatization in TURP, and uncertain relationship to BPH in RP tissues. This study aims to examine contractions of laser-enucleated tissues. Tissues from holmium/thulium laser enucleation (HoLEP/ThuLEP) and TURP were contracted by KCl, noradrenaline and electric field stimulation (EFS) in an organ bath. Contractions were compared to RP tissues in previous studies. KCl-induced contractions averaged 2.5 mN, 0.7 mN and 3.3 mN in tissues from HoLEP/ThuLEP, TURP and RP, with non-responsive tissues included (2.4% HoLEP/ThuLEP, 37% TURP). Maximum EFS-induced contractions (Emax) averaged 47% of KCl in HoLEP/ThuLEP tissues, 27% in TURP tissues, and 68–235% in 21 previous studies with RP tissues. Emax values for noradrenaline averaged 99.7% in HoLEP/ThuLEP tissues, 56% in TURP tissues, and ranged from 92 to 260% in RP tissues. Preoperative α1-blocker treatment reduced EFS- and noradrenaline-induced contractions, and increased EC50 values for noradrenaline in laser-enucleated, catheterized patients, but not in patients without catheterization. Also, the ex vivo application of α1-blockers increased the EC50 values for noradrenaline and reduced Emax for EFS. Laser-enucleated tissues allow investigation of prostate smooth muscle contraction in medication-refractory voiding symptoms. Different impacts of preoperative α1-blocker treatment on ex vivo contractility in tissues from patients with and without catheterization point to clinically relevant heterogeneity of patients undergoing surgery for BPH.
Similar content being viewed by others

Introduction
Prostate smooth muscle contraction is considered essential in the pathophysiology and medical treatment of voiding symptoms suggestive of benign prostatic hyperplasia (BPH)1,2. Increased prostate smooth muscle tone may contribute to urethral obstruction, resulting in impaired bladder emptying, and finally in symptoms1,2. The α1-adrenoceptor antagonists (α1-blockers), applied for rapid symptom improvement, represent the first line option for medical treatment and are believed to act by inhibition of α1-adrenergic prostate smooth muscle contraction2,3. The phosphodiesterase-5 inhibitor tadalafil is available as an alternative and is believed to improve symptoms by smooth muscle relaxation as well3. Treatment with 5α-reductase inhibitors (5ARI) is recommended for prevention of progression, complications and surgery in BPH3.
However, improvements by available drugs underlay obvious ceilings. The α1-blockers reduce symptom scores by maximally 30–50% and enhance the maximum urinary flow rate (Qmax) by not more than 40%2,3. These improvements are not far from placebos, reducing symptom scores by 10–34%, and increasing the Qmax up to 28%2,3. Tadalafil decreases symptom scores to similar extent as α1-blockers, but does not enhance Qmax in most studies3. During prolonged application 5ARIs may improve symptoms as well, but benefits are hardly or not additive with α1-blockers. Low adherence, attributed to insufficient efficacy and unbalanced side effects accounts for the progression and complications, hospitalization, and finally contributes to high numbers of surgery due to BPH2,3. Surgery often becomes inevitable with progression of BPH and despite drug treatment, in patients with imminent complications but also as last resort treatment for adequate symptom improvement3,4. Transurethral resection of the prostate (TURP) was the standard surgery for BPH for decades, while holmium and thulium laser enucleation of the prostate (HoLEP, ThuLEP) are increasingly established alternatives3,4.
Limited drug efficacy in voiding symptoms suggestive of BPH raised ongoing preclinical research addressing prostate smooth muscle contraction. Currently available drugs and drug candidates were developed based on experimental studies investigating their effects on contractions of prostate tissues in vitro, including human tissues. Tissue models included human tissues from radical prostatectomy (RP) for prostate cancer (PCa), or from TURP. However, TURP tissues have been supposed to be traumatized, by heat-induced denaturation during surgery, while RP tissues are not specifically representative for BPH, and do not cover medication-refractory voiding symptoms in BPH. To assess the potential of samples from laser enucleation for preclinical investigations, this study aims to examine the contractility of prostate tissues from HoLEP and ThuLEP.
Materials and methods
Study design, strategy and aims
This study was carried out in accordance with the Declaration of Helsinki of the World Medical Association and has been approved by the ethics committee of the Ludwig-Maximilians University, Munich, Germany (approval number 22-0608, from 08-10-2022). Informed consent was obtained from all patients. Samples and data were collected and analyzed pseudonymized. This study included two parts. Firstly, tissues were collected from laser enucleation (HoLEP, ThuLEP) and TURP, and randomly assigned to examination of electric field stimulation- (EFS)- and noradrenaline-induced contractions. The primary aims of this part were to explore whether tissues from laser nucleation are still contractile in organ bath experiments, and a comparison to TURP and RP tissues. Experiments with TURP tissues were discontinued after experiments with tissues from 43 patients, as it became obvious that a high percentage did not react to KCl. Experiments with laser-enucleated tissues were continued until tissues from 49 patients were examined with EFS, 59 patients with noradrenaline, and 2 patients with KCl but without showing contractions, all obtained from a total of 85 laser-enucleated patients. Laser-enucleated and TURP samples without reaction to KCl were included in frequency and concentration response curves and for calculation of Emax values, i. e. contractions in these samples were rated as 0 mN at each frequency and each noradrenaline concentration. KCl-induced contractions in samples from laser enucleation and TURP were compared to values from RP tissues in two of our previous study results5,6. Further, the Emax values for EFS and noradrenaline in samples from laser enucleation were compared to Emax values from our previous study results with RP tissues published 2018–20235,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25. EFS- and noradrenaline-induced contractions in laser-enucleated tissues were analyzed for different subgroups, including separation for patients with and without catheterization for urinary retention, and preoperative treatment with α1-blockers, after completion of all experiments.
Secondly, tissues from laser enucleation were collected from 21 further patients (not participating in the first part), and examined with EFS or noradrenaline, after the addition of α1-blockers or solvent (controls) in the organ bath. Thus, these experiments were planned and implemented after completion of the first part, as it turned out that laser-enucleated tissues are contractile in the organ bath. This second part was to assess, whether these tissues from laser enucleation are still suitable to examine effects of anticontractile drug candidates.
Holmium and thulium laser enucleation of the prostate
HoLEP enucleation was performed in a three-lobe technique, using the VersaPulse® 100W Holmium Laser (Lumenis Ltd., Yokneam, Israel) with a frequency of 53 Hz and a power setting of 1.2 kJ, or the 150 W CyberHo Holmium laser paired with a 550 micron end-firing laser fiber, utilizing energy settings of 2.0 J per puls and a frequency of 50 Hz. For ThuLEP enucleation, a Dornier Thulio® p-Tm:YAG with 570 micron end-firing disposable fiber was used with energy settings of 1.5 J per puls and a frequency of 50 Hz, resulting in 75 W. Tissue morcellation was performed using dual 5 mm reciprocating hollow metal blades. The same three-lobe technique was used for both the holmium and thulium laser enucleation26. Enucleation of the median lobe started distally and progressed proximally towards the bladder neck. Once detached, the median lobe was pushed into the bladder, and prostatic attachments were released from the bladder neck, allowing the median lobe to fall into the bladder. Enucleation of the lateral lobes proceeded similarly, beginning with the right lateral lobe at the level of the verumontanum. At the 5 o’clock position of the prostate apex, the lateral lobe was detached from the surgical capsule, and pushed into the urinary bladder. Dissection of the left lateral lobe followed a similar protocol, starting at the 7 o’clock position. Identical to the other side, the side flap on the surgical capsule was released using the laser and pushed into the bladder. Tissue morcellation was initiated by the insertion of an offset nephroscope fitted with a soft-tissue morcellator into the bladder, under adequate bladder filling. Tissues were shredded on the circular knife, effectively cutting the adenoma into smaller pieces, which were subsequently suctioned out of the bladder and collected.
Transurethral resection of the prostate
TURP was performed by bipolar resection. Compared to monopolar systems this leads to a lower resection temperature, and consequently to lower thermal damage in the surrounding tissue. Following the insertion of the resectoscope through the urethra, a high-frequency electrical current was used to remove overgrown tissue of the prostate, layer by layer until reaching the surgical capsule. After excess tissue was removed using a glass syringe, blood vessels were sealed to stop bleeding, and the resectoscope was removed.
Data from tissues from radical prostatectomy
For comparison of tissues from TURP and laser enucleation with tissues from RP, Emax values for EFS- and noradrenaline-induced contractions were compiled from control groups in previous studies with RP tissues from our lab (2018–2023)5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25. Emax values were collected from each single experiment, with each value representing the mean of two samples from the same prostate, or the value of a single determination if only one sample was available in an independent experiment. Values were obtained from the control groups of these previous studies and were consequently obtained with solvents (mostly dimethylsulfoxid, DMSO) in varying amounts. Tissues were collected from periurethral zones, as previously described5,6. Conditions for interim storage and transport were similar to conditions for tissues from surgery for BPH in this study, with the exception that tissues from RP were macroscopically inspected and sampled by pathologists.
Organ bath experiments
Collected tissues varied qualitatively between surgeries (Fig. 1). Macerations from laser-enucleation consisted of numerous small tissue shreds (dozens to hundreds per collected sample), with the largest measuring around 0.5–10 × 4 mm in size (Fig. 1). Tissue shreds matching the required size for organ bath experiments (approximately 6 × 3 × 3 mm) were either used directly without further cutting or prepared by cutting largest available shreds. TURP chips were typically larger than shreds from laser-enucleation, with most chips reaching ≥ 1 cm in length, but often including flat or narrow protrusions (Fig. 1). Strips for experiments were prepared from the largest available chips, specifically from interior regions of chunk-like parts and excluding margins (presumed to be most traumatized), extensions and flattened areas.

Tissues collected from HoLEP, TURP and RP. Content of one dish represents the complete sample being collected from one patient. Scale bars are 1 cm.
Organ bath experiments were performed as recently described for RP tissues5,6. Tissue strips were mounted in organ baths, with four chambers per device (model 720 M, Danish Myotechnology, Aahus, Denmark) containing 10 ml Krebs–Henseleit solution (37 °C, pH 7.4) continuously gassed with carbogen (95% O2 and 5% CO2). After adjustment of a stable pretension of 4.9 mN within 45 min5,6, tissues were contracted by 80 mM KCl, by the addition of a 2 M KCl solution. As soon as a maximum plateau contraction was obtained, high molar KCl was washed out, resulting in a new baseline. Subsequently, tissues were used directly for frequency response curves by EFS or concentration response curves for noradrenaline. In the second study part, α1-blockers or solvent (for controls) were added after washout of KCl, and frequency or concentration response curves were constructed 30 min later. With each strip, only one frequency or concentration response curve was recorded.
For construction of frequency and concentration response curves (without α1-blockers or solvent), strips were intuitively allocated to EFS and noradrenaline. Channels showing no reaction to KCl were not further examined by EFS or with noradrenaline, and included to analyses by rating as 0 mN at each frequency and noradrenaline concentration, except of a separate analysis as indicated. From a total of laser-enucleated tissues from 85 patients, 49 were examined by EFS and 59 with noradrenaline. In tissues from two patients, none of the strips contracted with KCl, which were included in data analyses by rating EFS- and noradrenaline-induced contractions as zero, resulting in tissues from 51 patients analyzed for EFS-induced, and from 61 patients analyzed for noradrenaline-induced contractions. Tissues from most patients were assessed by double or multiple determinations. In 46 out of 51 EFS experiments, 2–4 strips were examined per patient, and the remaining five as single determination with only one strip. In 53 out of 61 noradrenaline experiments, again multiple strips were examined per patient (2–4 strips for tissues from 49 patients, 5–8 strips for tissues from 4 patients). From a total of TURP tissues from 43 patients, 7 were examined by EFS and 26 with noradrenaline. In tissues from 16 patients, none of the examined strips contracted with KCl, which were rated as zero for analyses of EFS- and noradrenaline-induced contractions, resulting in TURP tissues from 23 patients analyzed for EFS, and from 42 patients analyzed for noradrenaline. In 21 out of 23 EFS experiments, multiple strips were examined per patient (2–4 strips for tissues from 18 patients, 6–8 strips for tissues from 3 patients). In 41 out of 42 noradrenaline experiments, multiple strips were examined per patient (2–4 strips for tissues from 28 patients, 5–8 strips for tissues from 13 patients).
Ex vivo effects of α1-blockers were assessed in paired samples, i. e. α1-blockers or solvent were added to tissue strips from the same patient, being examined in the same experiment. Double determinations for the solvent and antagonist group were possible in 30 out of a total of 41 experiments. In the remaining experiments, the amount of available tissues did not allow the filling of two channels for both groups or single samples did not contract with KCl. However, these experiments included three samples per experiment, split to the control and antagonist group.
Agonist- and EFS-induced contractions are expressed as percentage of 80 mM KCl-induced contractions, as this may correct individual variations and heterogeneities, and variables such as strip size or smooth muscle content. Emax values, EC50 values for agonists, and frequencies inducing 50% of the maximum EFS-induced contraction (EF50) were calculated separately for each single experiment by curve fitting27, using GraphPad Prism 6 (GraphPad Software Inc., San Diego, CA, USA). The software sends error messages, if curve fitting is not possible, or if results from curve fitting are suspected as “ambiguous”. In addition, values from curve fitting were checked manually for plausibility, as recommended in the “GraphPad Curve Fitting Guide” (GraphPad Software Inc.). Results in the first study part were marked as “ambiguous” in one EFS and one noradrenaline experiment. Following manual inspection, these values were considered plausible. As curve fitting was not possible with samples without contractions, Emax for these tissues was set to 0 mN. Concentration response curves addressing ex vivo effects of α1-blockers included noradrenaline concentrations up to 3 mM, to allow detection of rightshifts and recovery at high agonist concentrations, and to allow curve fitting in antagonist groups. Consequently, control curves frequently included downhill parts at high agonist concentrations, which had to be excluded in 8 out of 21 experiments with noradrenaline, to allow plausible curve fitting. Values from 2 curves with tamsulosin, one with noradrenaline and one with EFS, were labelled as “ambiguous”, but provided plausible values after the exclusion of untypical values. Data for catheterization were available from 81 and for premedication from 82 out of 85 patients. Contraction data from patients with unavailable clinical data were excluded from group analyses.
Statistical analyses
Data in frequency and concentration response curves are means with standard deviation (SD). Single values in scatter plots are either means from all strips examined per tissue, or are values from each single strip. Group differences and effect sizes in the text are reported as mean differences (MD) with 95% confidence intervals (95% CI). Calculation of MDs and 95% CIs, and statistical analyses were performed using GraphPad Prism 6. Distribution of values within data sets including KCl-induced contractions, Emax, EC50 and EF50 values were assessed by the D’Agostino & Pearson omnibus normality test (alpha = 0.05). Groups showing Gaussian distribution were compared using parametric tests, while non-parametric tests were applied to data sets containing at least one group not passing the normality test. Comparisons of KCl-induced contractions between three groups, and comparisons of previously reported Emax values to Emax values in the current study were performed by Dunn’s multiple comparison after one-way ANOVA with Kruskal Wallis test, allowing comparison of multiple groups without normal distribution. Emax, EC50 and EF50 values in grouping analyses (i. e., between two groups) were compared by unpaired, two-tailed Mann Whitney test if data were not normally distributed in at least one of both groups, and by unpaired, two-tailed t test if data were normally distributed in both groups. Emax, EC50 and EF50 values between paired groups (i. e., with/without ex vivo application of tamsulosin or silodosin) were compared by paired, two-tailed Wilcoxon matched-pairs signed rank test if data were not normally distributed in at least one of both groups, and by paired, two-tailed t test if data were normally distributed in both groups. Comparison of whole frequency and concentration response curves was performed by two-way analysis of variance (ANOVA), without multiple comparison and as data sets included three variables (concentration, contraction, treatment)27. P values < 0.05 were considered significant. P values ≥ 0.05 are not indicated. The present study and analyses show an exploratory design, as typical features of a hypothesis-testing study are lacking, including a clear preset study plan, blinding, or biometric calculation of group sizes28. Consequently, P values reported here are descriptive, but not hypothesis-testing28. While the formation of group sizes was not driven by power calculations, 10 independent experiments per series were consistently found sufficient to detect biologically relevant differences or to detect drug effects in our previous organ bath experiments. Consequently, and as splitting into up to 4 subgroups was intended, while it was anticipated that clinical data would not be available from some patients, experiments with tissues from 50 to 60 patients were aimed with noradrenaline and EFS in part one, and from at least 10 patients per series in part two, without interim analyses.
Results
Potassium-induced contractions
Potassium-induced contractions of laser-enucleated tissues from HoLEP and ThuLEP (n = 85 patients) were higher compared to tissues from TURP (n = 43 patients) (HoLEP/ThuLEP 2.49 mN [2.07–2.92]; TURP 0.72 mN [0.38–1.06]; MD 1.77 mN [0.76–2.78]) (Fig. 2a). Potassium-induced contractions of RP tissues (RP 3.32 mN [3–3.64]; n = 189 patients) were higher compared to HoLEP/ThuLEP tissues (MD 0.83 mN [0.13–1.54]), and compared to TURP tissues (MD 2.6 mN [1.69–3.52]) (Fig. 2a). Included to these analyses are tissues and samples showing no reaction to KCl. In 2 out of 85 tissues from laser enucleation (2.4%), none of the examined single samples responded to KCl, while 16 out of 43 tissues from TURP (37.2%) were completely unresponsive to KCl with each examined sample.

Potassium-induced contractions in tissues from surgery for BPH, and from radical prostatectomy for PCa. Shown are means from each tissue (a) (i.e., values represent means, mostly based on investigation of two or more samples from one tissue), values from each examined tissue sample (b) (i.e., without calculating means for each prostate tissue), and again values from each examined single sample, but with samples showing no reaction to KCl (i. e., 0 mN) being omitted (c). Contractions by 80 mM potassium were induced before proceeding with construction of frequency response curves for EFS, or with concentration response curves for noradrenaline, using tissues from laser enucleation (HoLEP/ThuLEP) or TURP for BPH, or from RP for PCa. Data from RP tissues are from two of our previous studies5,6. Data are shown together with means for each groups (bars), and with P values from Dunn’s multiple comparison test after one-way ANOVA with Kruskal Wallis test.
These differences persisted, if contractions of all single samples were analyzed instead of means of each prostate. Again, the difference between laser-enucleated and RP tissues was smaller (HoLEP/ThuLEP 2.57 mN [2.27–2.87]; RP 3.33 mN [3.1–3.55]; MD 0.76 mN [0.29–1.26]), than the difference between TURP tissues and both other groups (TURP 0.58 mN [0.38–0.77]; MD 2.75 mN [2.12–3.38] vs. RP; MD 1.99 mN [1.37–2.61] vs. HoLEP/ThuLEP) (Fig. 2b). If samples from HoLEP/ThuLEP tissues showing no reaction to KCl (i. e., 0 mN) were excluded (what was done with RP tissues) (Fig. 2c), contractions were again similar between tissues from HoLEP/ThuLEP and RP (HoLEP/ThuLEP 2.99 mN [2.66–3.32]; RP 3.33 mN [3.1–3.55]; MD 0.33 mN [-0.18 to 0.846]), but still substantially lower in TURP tissues. The percentage of single samples without reaction to highmolar KCl amounted to 60% in TURP tissues and 14% in tissues from laser enucleation.
EFS-induced contractions
EFS induced frequency-dependent contractions in laser-enucleated tissues (n = 51 patients) (Fig. 3a). Emax values were calculated by curve fitting and compared to Emax values from control groups (i. e., preincubated with solvents, but without drugs) in our previous studies with RP tissues (2018–2023). Emax values from HoLEP/ThuLEP tissues were not statistically different to Emax values for EFS-induced contractions of RP tissues in 6 from 21 of these previous studies (Fig. 3a). In 15 from 21 of studies with RP tissues, Emax values for EFS-induced contractions were higher compared to Emax values in tissues from HoLEP/ThuLEP (Fig. 3a). With an average Emax of 47% [35–60] of KCl-induced contractions, contractions of HoLEP/ThuLEP tissues ranged lower than Emax values in all studies with RP tissues, but with high overlap and with the closest Emax values in two studies with RP tissues ranging at 68% [49–88] and 69% [55–84] of KCl-induced contractions (Fig. 3a). The variability and range of maximum EFS-induced contractions in RP tissues was high across studies, with the highest Emax values mounting to 235% [150–320] and to 166% [107–224] of KCl-induced contractions (Fig. 3a). With an Emax of 27% [7–48], EFS-induced contractions of TURP tissues were obviously lower compared to laser-enucleated and to RP tissues (Fig. 3a).

EFS- and noradrenaline-induced contractions in tissues from surgery for BPH, and from radical prostatectomy for PCa. Frequency response curves for EFS (a) and concentration response curves for noradrenaline (b) were constructed in tissues from laser enucleation (HoLEP, ThuLEP) and TURP. Emax values were calculated by curve fitting, for EFS (a) and noradrenaline (b). Emax for RP tissues from are from control groups in our previous studies, published from 2018 to 2023. Accordingly, contractions with RP tissues were induced in the presence of different amounts of solvent (mostly DMSO), used in controls for drugs examined in these previous studies, whereas contractions with tissues from laser enucleation and TURP were induced without solvent. Data in frequency and concentration response curves are means with standard deviation (SD). Frequency and concentration response curves were compared by two-way ANOVA. Emax values from RP tissues were compared by one-way ANOVA with Dunn’s test to Emax values from laser-enucleated tissues (grey data sets: p < 0.05 vs. HoLEP/ThuLEP; see supplementary table 1 for details).
Noradrenaline-induced contractions
Noradrenaline induced concentration-dependent contractions in laser-enucleated tissues (n = 60 patients) (Fig. 3b). Emax values were calculated by curve fitting and compared to Emax values from control groups (i. e., preincubated with solvents, but without drugs) in our previous studies with RP tissues (2018–2023). Emax values in tissues from HoLEP/ThuLEP were similar (i. e., not statistically different) to Emax values for noradrenaline-induced contractions of RP tissues in 7 from 20 of these previous studies (Fig. 3b). In the 13 other from 20 of studies with RP tissues, Emax values for noradrenaline-induced contractions were higher compared to Emax values observed with tissues from HoLEP/ThuLEP (Fig. 3b). With an average Emax of 99.7% [85–114] of KCl-induced contractions, contractions of HoLEP/ThuLEP tissues ranged lower than Emax in 19 of the 20 studies with RP tissues, but with high overlap and with the closest Emax values ranging at 92% [71–112] and 118% [103–133] of KCl-induced contractions in two studies with RP tissues (Fig. 3b). The variability and range of maximum noradrenaline-induced contractions in RP tissues was high across studies, with the highest Emax values mounting to 260% [112–407] and to 217% [150–284] of KCl-induced contractions (Fig. 3b). With an Emax of 56% [34–79], noradrenaline-induced contractions of TURP tissues were obviously lower compared to laser-enucleated and to RP tissues (Fig. 3b).
Grouping of EFS-induced contractions of HoLEP/ThuLEP tissues
EFS-induced contractions were similar in tissues from patients without (n = 25) and with catheter (n = 22) (Fig. 4a). In patients receiving preoperative treatment with α1-blockers (n = 21), contractions were by trend (though, not significantly) lower compared to patients without treatment (n = 26) (Emax 68% [41–94] of KCl without α1-blocker, 41% [27–55] with α1-blocker, MD 27% [0–54]) (Fig. 4b). In patients without catheter, contractions were similar in tissues from patients with (n = 17) or without (n = 8) treatment with α1-blockers (Fig. 4c). However, in patients with catheter, contractions were substantially lower in patients with α1-blocker treatment (n = 8), compared to patients without α1-blocker treatment (n = 13) (Fig. 4d). Lower contractions in α1-blocker-treated patients were reflected by decreased Emax values (Emax 64% [36–92] of KCl without α1-blocker, 18% [11–25] with α1-blocker, MD 46% [11–81]) (Fig. 4d). Without α1-blocker treatment, contractions were similar in tissues from patients without (n = 8) and with (n = 13) catheter (Fig. 4e). In patients with α1-blocker treatment, contractions were lower in patients with catheter (n = 8), compared to tissues from patients without catheter (n = 17) (Emax 47% [22–72] of KCl without catheter, 18% [11–25] with catheter, MD 29% [-7 to 65]) (Fig. 4f).

EFS-induced contractions in laser-enucleated tissues, grouped for preoperative catheterization and preoperative treatment with α1-blockers. Data from EFS-induced contractions were grouped as indicated, for preoperative catheterization of patients due to urinary retention (a), for preoperative treatment with α1-blockers (b), or both (c-f). Patients’ data regarding catheterization and medical treatment were available from 47 of a total of 51 patients participating in this series (25 without, 22 with catheter; 26 treated, 21 not treated with α1-blocker). Shown are means ± standard deviation (SD) in frequency response curves, and all single values for Emax and EF50 calculated by curve fitting (each value representing one prostate tissue, examined by single or multiple determinations) together with means (bars). Frequency response curves were compared by two-way ANOVA. Emax and EF50 values were compared by unpaired, two-tailed t test if data were normally distributed in both groups (i. e., EF50 values in (b) and (f)), and by unpaired, two-tailed Mann Whitney test if data were not normally distributed in at least one of both groups (all others). P values ≥ 0.05 are not shown. One EF50 value (labelled by grey color) could not be calculated by curve fitting, as the sample showed no contraction (corresponding to an Emax of 0% of KCl), but was set to the highest applied frequency, i.e. 32 Hz for illustration.
Grouping of noradrenaline-induced contractions in HoLEP/ThuLEP tissues
Noradrenaline-induced contractions were similar in tissues from patients without (n = 31) and with catheter (n = 26) (Fig. 5a). In patients receiving preoperative treatment with α1-blockers (n = 34), contractions were by trend (though, not significantly) lower compared to patients without treatment (n = 24) (Fig. 5b). While Emax values for noradrenaline were similar between both groups, EC50 values for noradrenaline were increased in tissues from patients with α1-blocker pretreatment, compared to tissues from patients without pretreatment (pEC50 6.01 [0.08–0.41] without α1-blocker, 5.44 [0.07–0.34] with α1-blocker, MD 0.57 [0.11–0.54]) (Fig. 5b). In patients without catheter, contractions were similar in tissues from patients with (n = 22) or without (n = 9) treatment with α1-blockers (Fig. 5c). While Emax values were similar between both groups, EC50 values for noradrenaline were increased by trend in tissues with α1-blocker treatment, compared to tissues from patients without treatment (pEC50 5.79 [5.11–6.46] without α1-blocker, 5.48 [5.21–5.745] with α1-blocker, MD 0.31 [-0.4 to 1.02]) (Fig. 5c). In patients with catheter, contractions were substantially lower in patients with α1-blocker treatment (n = 11), compared to patients without α1-blocker treatment (n = 15) (Fig. 5d). Lower contractions in α1-blocker-treated patients were reflected by decreased (though, not significantly) Emax values (122% [94–151] of KCl without α1-blocker, 82% [48–116] with α1-blocker, MD 40% [2–82] of KCl), and by increased EC50 values for noradrenaline (pEC50 6 [5.79–6.2] without α1-blocker, 5.45 [5.23–5.68] with α1-blocker, MD 0.54 [0.28–0.81]) (Fig. 5d). Without α1-blocker treatment, contractions were higher in tissues from patients with catheter (n = 15) compared to tissues from patients without catheter (n = 9) (Fig. 5e). Changes were reflected by Emax values, which were increased by trend (80% [43–116] of KCl without catheter, 122% [94–151] of KCl with catheter, MD 43% [-1 to 86] of KCl), while EC50 values for noradrenaline were similar between both groups (Fig. 5e). In patients with α1-blocker treatment, contractions were similar in tissues from patients without (n = 22) and with (n = 11) catheter (Fig. 5f).

Noradrenaline-induced contractions in laser-enucleated tissues, grouped for preoperative catheterization and preoperative treatment with α1-blockers. Data from noradrenaline-induced contractions were grouped as indicated, for preoperative catheterization of patients due to urinary retention (a), for preoperative treatment with α1-blockers (b), or both (c-f). Patients’ data regarding catheterization were available from 57 patients (31 without, 26 with catheter), and regarding medical treatment from 59 patients (34 treated, 25 not treated with α1-blockers), from a total of 61 patients participating in this series. Shown are means ± standard deviation (SD) in concentration response curves, and all single values for Emax and EC50 calculated by curve fitting (each value representing one prostate tissue, examined by single or multiple determinations) together with means (bars). Concentration response curves were compared by two-way ANOVA. Emax and EC50 values were compared by unpaired, two-tailed t test if data were normally distributed in both groups (i. e., EC50 values in (a) and (e)), and by unpaired, two-tailed Mann Whitney test if data were not normally distributed in at least one of both groups (all others). P values ≥ 0.05 are not shown. One EC50 value (labelled by grey color) could not be calculated by curve fitting, as the sample showed no contraction (corresponding to an Emax of 0% of KCl), but was set to the highest noradrenaline concentration applied in these series, i.e. -4 for illustration.
Ex vivo effects of α1-blockers on contractions in laser-enucleated tissues
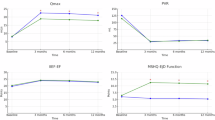
Effects of tamsulosin and silodosin, applied ex vivo in the organ bath, were examined in separate series with laser-enucleated tissues from 21 further patients. Both antagonists caused right shifts of concentration response curves for noradrenaline, increased EC50 values but unchanged Emax values for noradrenaline, and decreased Emax values for EFS (Fig. 6), without that further grouping was required. Tamsulosin increased the EC50 values for noradrenaline, from -6.09 [-6.32 to -5.86] in controls to -4.23 [-5.1 to -3.40] with tamsulosin (MD 1.87 [1.1–2.63] without reducing Emax values, and decreased the Emax for EFS-induced contractions from 91% [61–121] of KCl-induced contractions in controls, to 39% [19–59] with tamsulosin (MD -52% [-90 to -15]) without reducing EF50 values for EFS (Fig. 6a). Silodosin increased the EC50 values for noradrenaline, from -6.38 [-7.02 to -5.75] in controls to -3.89 [-4.64 to -3.13] with tamsulosin (MD 2.499 [1.87–3.13] without reducing Emax values, and decreased the Emax for EFS-induced contractions from 69% [43–95] of KCl-induced contractions in controls, to 28% [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39] with tamsulosin (MD -40% [-71 to -9]) without reducing EF50 values for EFS (Fig. 6b).

Ex vivo effects of α1-blockers on noradrenaline- and EFS-induced contractions of laser-enucleated tissues. Concentration response curves for noradrenaline and frequency response curves for EFS were constructed 30 min after application of solvent (controls) or 100 nM tamsulosin (a) or 100 nM silodosin (b) in tissues from laser enucleation (HoLEP, ThuLEP). Emax, EC50 and EF50 values were calculated by curve fitting. Shown are means ± standard deviation (SD) in concentration and frequency response curves, and all single values for Emax and EC50 calculated by curve fitting (each value representing one prostate tissue, examined by single or multiple determinations) together with means (bars). Concentration and frequency response curves were compared by two-way ANOVA. Emax and EF50 values were compared by paired, two-tailed Wilcoxon matched-pairs signed rank test if data were not normally distributed in at least one of both groups (EF50 values, and Emax values for noradrenaline), and by paired, two-tailed t test if data were normally distributed in both groups (all others). P values ≥ 0.05 are not shown. One EC50 value marked in grey in (b) was calculated around -12, but has been included as -8 for better illustration (P value refers to data set including -12). Data are from n = 11 independent experiments for silodosin and EFS, and n = 10 independent experiments in each of the three other series, with the control and antagonist group in an independent experiment performed with tissue from the same patients, and with the number of experiments equating to the number of patients participating in a series. Experiments were performed with tissues from a total of 21 patients, not being included in other series of this study.
Discussion
To the best of our knowledge, this study is the first to address the smooth muscle contractility of tissues obtained by laser enucleation. Preclinical investigation of prostate smooth muscle contraction was crucial in the development of currently available drugs for treatment of voiding symptoms, including α1-blockers and the phosphodiesterase-5 inhibitor tadalafil. Meanwhile, limitations of these medications became evident2, initiating ongoing searches for novel targets and new candidate compounds, together with attempts to understand the reasons accounting for these limits. Consequently, contraction studies are of continuous interest. The findings of this study identify tissues from laser enucleation as a new model for investigation of prostate smooth muscle contraction, in patients with medication-refractory voiding symptoms in BPH.
Typically, patients selected for surgery for BPH are characterized by severe symptoms, while treatment with α1-blockers is recommended for patients with moderate to severe symptoms3. Ablative surgery is performed if complications of BPH are experienced, but also for adequate relief from lower urinary tract symptoms (LUTS) or postvoid urine in non-responders for medical treatment, or if medical treatment is refused but active treatment requested3,4. Thus, effective medical treatment is not available for these populations. Previous studies addressing prostate smooth contractions either used tissues from TURP or RP for PCa. TURP tissues cover the same or a similar patient group as laser-enucleated tissues. However, their use was often supposed to be limited by heat-induced traumatization, reducing their contractility in vitro. In our hands, TURP tissues were characterized by lower contractions compared to laser-enucleated tissues, and by an exceeding rate of complete non-responsiveness to contractile stimulation. While previous studies obtained results from TURP tissues, also with unquestioned relevance, information about exclusion and percentage of non-contractile tissues was rarely reported. In turn, tissues from RP for PCa, but without previous surgery for BPH were widely used in our previous studies. According to the prevalence of BPH in this age group1, BPH and mild symptoms are likely in these patients, but these tissues from RP do not specifically cover the context of severe or medication-refractory voiding symptoms. As contractions of laser-enucleated tissues approached ranges of contractions seen with RP tissues, without high rates of non-responsiveness due to traumatization by surgery, these tissues may provide a suitable model to study prostate smooth muscle contraction in patients with severe and medication-refractory LUTS. Finally, it allows to correlate in vitro findings with clinical data in the future, while BPH-specific data including international prostate symptom score (IPSS), Qmax or postvoid residual urine volume are not routinely assessed in patients undergoing RP for PCa.
The reasons accounting for the divergent impacts of preoperative α1-blocker treatment, seen between patients with and without catheterization for urinary retention are still elusive at this stage. Pretreatment with α1-blockers resulted in reduced contractions by EFS and noradrenaline in tissues from catheterized patients, but not in tissues from patients without catheterization. Certainly, this difference reflects substantial, yet unknown heterogeneity between both populations, even though both groups receive surgery for BPH. Reasons may include 1) different tissue responsiveness to α1-blockers, 2) different tissue conditions affecting the drug availability in tissues ex vivo, or 3) differences affecting drug metabolism and bioavailability in vivo, and 4) further reasons and combinations. A different tissue responsiveness to α1-blockers could be imparted by divergent receptor expression, or by unknown differences in receptor regulation29. Considering that ex vivo application of α1-blockers caused full effects, without grouping of patients, such differences in tissue responsiveness may be regarded as unlikely to impart the difference seen between catheterized and uncatheterized patients. Nevertheless, this cannot fully be excluded, as the experimental design differed for preoperative and ex vivo application of α1-blockers, including comparison of different patients in one series, but a comparison of paired samples from the same patients in the other series.
Divergent tissue conditions may provide plausible explanations for the different impact of preoperative α1-blocker treatment in both groups. BPH may include stromal, glandular and mixed hyperplasia, but their specific contributions to symptoms and drug responsiveness are not understood and have been poorly documented in preclinical and clinical studies30. Similar, prostatic fibrosis is a just recently emerging topic, and may include progressive deposition of extracellular matrix (ECM) compounds31,32,33,34. Drug penetration into tissues may reduce with increasing ECM content, depending on but also independently from vascularization in these tissue parts. This may reduce drug availability in vivo and thus, affect ex vivo contractility. Other factors related to tissue conditions may account as well. Different stromal-epithelial contents may determine the washout of α1-blockers during ex vivo procedures. Washout may be less effective in stromal compartments, and thus in tissues with high stromal content, compared to spongy tissues with high glandular content. With all due caution and if proving true, this may point to impaired washout of α1-blockers during ex vivo handling and thus, to predominant stromal hyperplasia in patients with catheterization (i.e. with urinary retention), and to predominant glandular hyperplasia in patients without. High individual variation in tissue consistency becomes obvious during routine work with TURP and laser ablation, ranging from soft to stiff tissues. In the run-up of the study, it was speculated that α1-blockers in the tissues, resulting from medication for voiding symptoms, will be washed out during surgery, intravesical maceration, transport and storage in custodiol solution, and finally by Krebs-Hensleit solution in the organ bath. Together, different tissue composition by cellular and non-cellular constituents, but also the phenotype of BPH may affect drug penetration and their removal in tissues, and may decide about clinical characteristics including urinary retention. Notably, the observable ex vivo effects from preoperative α1-blocker treatment seen in tissues from catheterized patients prove that the treatment affects prostate smooth muscle contractility, but without improving symptoms or complications, so these patients are evidentially medication-refractory.
Results from application of α1-blockers ex vivo demonstrated that tissues from laser-enucleation are suitable for investigation of drug effects in the context of BPH. Application of α1-blockers in the organ bath still resulted in full potential effects, including increases in EC50 values for α1-adrenergic agonists and recovery at high agonist concentrations. Considering that these patients needed surgery, despite treatment with α1-blockers and despite the effects of α1-blockers ex vivo, this raises the question, of whether inhibition of α1-adrenergic contractions, or smooth muscle contractions at all is a suitable strategy in these patients. For α1-adrenergic contractions, this is not the case. In addition to α1-adrenoceptors, prostate smooth muscle contraction can be induced by endothelins and thromboxane, to the maximum possible force. These non-adrenergic contractions were proposed to maintain full smooth muscle tone and thus, symptoms in medication-refractory LUTS2,35. Consequently, it appears possible that full inhibition of adrenergic contractions is insufficient for clinical effects, even if smooth muscle tone contributes to symptoms. On the other hand, it appears possible as well, that symptom severity is unrelated to smooth muscle contraction, even though this concept has been claimed for decades, but in view that a causative role of bladder outlet obstruction and symptoms has been challenged2.
While technical traumatization had lower effects on contractility in laser-enucleated tissues than in TURP tissues, influences of chopping, maceration and handling can not be fully excluded. TURP has been the gold standard in surgery for BPH for decades3,36. Laser-enucleation still has a niche existence in comprehensive healthcare36,37, but may gain in popularity, reaching a share of 20% in surgeries for BPH performed in France in 2018, and may increasingly replace TURP or emerged as the preferred option in centers with corresponding expertise38,39,40. HoLEP and ThuLEP equally relieve voiding symptoms, with high efficacy and safety41. Heat generation in HoLEP and ThuLEP occurs by absorption of laser radiation by the prostate tissue, leading to heating and vaporization of water within the tissue. Comprehensive data allowing direct comparisons to TURP are limited for laser-enucleation, but heat development and propagation within the prostate and in the suprapubic region appear limited with HoLEP and ThuLEP42,43,44. Ex vivo, increases in temperatures across the instrument shaft and within the enucleation cavity remained below 5 K at any examined irrigation (apart from 0 ml/min), which is insufficient to cause tissue damage43. Injurious temperatures are probably not attained during clinical application45,46. The depth of necrotic zones and tissue coagulation typically varies between studies and conditions for TURP47, and probably for laser enucleation as well, where it may range from 0.1 to 4 mm43,48. Together, higher contractions of laser-enucleated tissues, compared to tissues from TURP may reflect a lower degree of heat-induced traumatization during surgery.
While the observed differences between subgroups are of potential clinical relevance, the study is associated with limitations. The differences between patients with and without catheterization were surprising and obvious, but their investigation was not the primary aim. Thus, the initial, primary endpoint was the contractility in laser-enucleated tissues, in comparison to widely-used human tissue models. Unlike previous studies in which contractions were measured with solvent (as controls for test compounds), contractions were measured without further intervention in the current study. As another limitation, the study design does not take into account that male LUTS include storage symptoms caused by the urinary bladder, in addition to voiding symptoms attributed to BPH, or that conditions similar to voiding symptoms can be caused by an underactive bladder, instead of obstruction. A non-negligible number of patients with voiding symptoms (approximately 50%) also show detrusor overactivity and associated storage symptoms including urgency or frequency49,50. Clinical conditions and etiology of storage symptoms are highly variable, and may include or affect cholinergic voiding contractions of the detrusor, and non-cholinergic detrusor microcontractions initiating the micturition reflex51. Storage symptoms in male mixed LUTS may develop secondary to obstruction or independently from it, and persist after desobstructive surgery. In no case, however, detrusor contractions are induced by α1-adrenoceptors, explaining why storage symptoms are resistant to α1-blockers51. Consequently, symptom resistance to BPH-specific drugs may have been attributed to a certain, though unknown part of the study population, in particular in participants with high initial storage symptom scores, or with an underactive bladder. In fact, definite separation of voiding symptoms caused by obstruction from symptoms resulting from underactive or overactive bladder requires diagnosis by invasive urodynamics, or specific assessment of storage symptom scores3,52. In real world settings, decisions for desobstructive surgery are commonly based on routine care for male LUTS, not including diagnosis by invasive urodynamics49. It has been estimated, that 18–28% of patients undergoing prostate surgery for LUTS have no obstruction53. Symptoms in these patients may be predominantly attributed to bladder malfunction, and the surgery may be potentially unnecessary49,53. Thus, studies using tissues from desobstructive surgery addressing truly medication-refractory voiding symptoms should integrate data from diagnosis for storage symptoms.
Conclusions
Smooth muscle contractions are intact in laser-enucleated prostate tissues, allowing investigation of prostate smooth muscle contraction in the context of medication-refractory voiding symptoms. Other than in TURP tissues, intrasurgical tissue traumatization does not limit investigation of contractility. Impacts of preoperative α1-blocker treatment divergently affected ex vivo contractility in tissues from patients with and without catheterization, reflecting fundamental differences in tissue conditions between patients with and without urinary retention. Heterogeneity in BPH differentially affects the risk for urinary retention in both subgroups, by unknown factors and despite shared surgery by laser-enucleation.
Data availability
All data that support the findings of this study are included in this published article. Raw data are available from the corresponding author upon reasonable request.
References
Lepor, H. Pathophysiology, epidemiology, and natural history of benign prostatic hyperplasia. Rev. Urol. 6(Suppl 9), S3–S10 (2004).
Hennenberg, M. & Michel, M. C. Adrenoceptors in the Lower Urinary Tract. Handb. Exp. Pharmacol. https://doi.org/10.1007/164_2023_678 (2023).
Gravas, S. et al. Summary Paper on the 2023 European Association of Urology Guidelines on the Management of Non-neurogenic Male Lower Urinary Tract Symptoms. Eur. Urol. 84, 207–222. https://doi.org/10.1016/j.eururo.2023.04.008 (2023).
Magistro, G. & Stief, C. G. Surgery for benign prostatic obstruction. Lancet 396, 5–7. https://doi.org/10.1016/S0140-6736(20)31287-3 (2020).
Hu, S. et al. Selective inhibition of neurogenic, but not agonist-induced contractions by phospholipase A(2) inhibitors points to presynaptic phospholipase A(2) functions in contractile neurotransmission to human prostate smooth muscle. Neurourol. Urodyn. 42, 1522–1531. https://doi.org/10.1002/nau.25242 (2023).
Hu, S. et al. Organ-specific off-target effects of Pim/ZIP kinase inhibitors suggest lack of contractile Pim kinase activity in prostate, bladder, and vascular smooth muscle. Naunyn. Schmiedebergs Arch. Pharmacol. 397, 1219–1231. https://doi.org/10.1007/s00210-023-02664-6 (2024).
Huang, R. et al. Concentration-dependent alpha1-adrenoceptor antagonism and inhibition of neurogenic smooth muscle contraction by mirabegron in the human prostate. Front. Pharmacol. 12, 666047. https://doi.org/10.3389/fphar.2021.666047 (2021).
Huang, R. et al. Inhibition of alpha(1)-adrenergic, non-adrenergic and neurogenic human prostate smooth muscle contraction and of stromal cell growth by the isoflavones genistein and daidzein. Nutrients https://doi.org/10.3390/nu14234943 (2022).
Huang, R. et al. Inhibition of human prostate smooth muscle contraction by the inhibitors of protein kinase C, GF109203X, and Go6983. Prostate 82, 59–77. https://doi.org/10.1002/pros.24248 (2022).
Huang, R. et al. Antagonism of alpha(1)-adrenoceptors by beta(3)-adrenergic agonists: Structure-function relations of different agonists in prostate smooth muscle contraction. Biochem. Pharmacol. 202, 115148. https://doi.org/10.1016/j.bcp.2022.115148 (2022).
Liu, Y. et al. Inhibition of growth and contraction in human prostate stromal cells by silencing of NUAK1 and -2, and by the presumed NUAK inhibitors HTH01-015 and WZ4003. Front. Pharmacol. 14, 1105427. https://doi.org/10.3389/fphar.2023.1105427 (2023).
Spek, A. et al. Purinergic smooth muscle contractions in the human prostate: estimation of relevance and characterization of different agonists. Naunyn Schmiedebergs Arch. Pharmacol. 394, 1113–1131. https://doi.org/10.1007/s00210-020-02044-4 (2021).
Tamalunas, A. et al. Lenalidomide and pomalidomide inhibit growth of prostate stromal cells and human prostate smooth muscle contraction. Life Sci. 281, 119771. https://doi.org/10.1016/j.lfs.2021.119771 (2021).
Tamalunas, A. et al. Inhibition of human prostate stromal cell growth and smooth muscle contraction by thalidomide: A novel remedy in LUTS?. Prostate 81, 377–389. https://doi.org/10.1002/pros.24114 (2021).
Tamalunas, A. et al. Inhibition of human prostate and bladder smooth muscle contraction, vasoconstriction of porcine renal and coronary arteries, and growth-related functions of prostate stromal cells by presumed small molecule galpha(q/11) inhibitor, YM-254890. Front. Physiol. 13, 884057. https://doi.org/10.3389/fphys.2022.884057 (2022).
Tamalunas, A. et al. Permixon(R), hexane-extracted Serenoa repens, inhibits human prostate and bladder smooth muscle contraction and exerts growth-related functions in human prostate stromal cells. Life Sci. 308, 120931. https://doi.org/10.1016/j.lfs.2022.120931 (2022).
Herlemann, A. et al. Inhibition of smooth muscle contraction and ARF6 activity by the inhibitor for cytohesin GEFs, secinH3, in the human prostate. Am. J. Physiol. Renal. Physiol. 314, F47–F57. https://doi.org/10.1152/ajprenal.00125.2017 (2018).
Li, B. et al. The STK16 inhibitor STK16-IN-1 inhibits non-adrenergic and non-neurogenic smooth muscle contractions in the human prostate and the human male detrusor. Naunyn Schmiedebergs Arch. Pharmacol. 393, 829–842. https://doi.org/10.1007/s00210-019-01797-x (2020).
Li, B. et al. Inhibition of neurogenic and thromboxane A2 -induced human prostate smooth muscle contraction by the integrin alpha2beta1 inhibitor BTT-3033 and the integrin-linked kinase inhibitor Cpd22. Prostate 80, 831–849. https://doi.org/10.1002/pros.23998 (2020).
Wang, X. et al. Onvansertib, a polo-like kinase 1 inhibitor, inhibits prostate stromal cell growth and prostate smooth muscle contraction, which is additive to inhibition by alpha1-blockers. Eur. J. Pharmacol. 873, 172985. https://doi.org/10.1016/j.ejphar.2020.172985 (2020).
Wang, X. et al. Ghrelin aggravates prostate enlargement in rats with testosterone-induced benign prostatic hyperplasia, stromal cell proliferation, and smooth muscle contraction in human prostate tissues. Oxid. Med. Cell Longev. 2019, 4748312. https://doi.org/10.1155/2019/4748312 (2019).
Yu, Q. et al. A NAV2729-sensitive mechanism promotes adrenergic smooth muscle contraction and growth of stromal cells in the human prostate. J. Biol. Chem. 294, 12231–12249. https://doi.org/10.1074/jbc.RA119.007958 (2019).
Yu, Q. et al. Inhibition of human prostate smooth muscle contraction by the LIM kinase inhibitors, SR7826 and LIMKi3. Br. J. Pharmacol. 175, 2077–2096. https://doi.org/10.1111/bph.14201 (2018).
Yu, Q. et al. Inhibition of prostatic smooth muscle contraction by the inhibitor of G protein-coupled receptor kinase 2/3, CMPD101. Eur. J. Pharmacol. 831, 9–19. https://doi.org/10.1016/j.ejphar.2018.04.022 (2018).
Hennenberg, M. et al. Inhibition of prostate smooth muscle contraction by inhibitors of polo-like kinases. Front. Physiol. 9, 734. https://doi.org/10.3389/fphys.2018.00734 (2018).
Tamalunas, A. et al. Efficacy, efficiency, and safety of en-bloc vs three-lobe enucleation of the prostate: A propensity score-matched analysis. Urology 175, 48–55. https://doi.org/10.1016/j.urology.2023.02.014 (2023).
Huang, R. et al. Inhibition of neurogenic contractions in renal arteries and of cholinergic contractions in coronary arteries by the presumed inhibitor of ADP-ribosylation factor 6, NAV2729. Naunyn Schmiedebergs Arch. Pharmacol. 395, 471–485. https://doi.org/10.1007/s00210-022-02218-2 (2022).
Michel, M. C., Murphy, T. J. & Motulsky, H. J. New author guidelines for displaying data and reporting data analysis and statistical methods in experimental biology. Mol. Pharmacol. 97, 49–60. https://doi.org/10.1124/mol.119.118927 (2020).
Michel, M. C. & Vrydag, W. Alpha1-, alpha2- and beta-adrenoceptors in the urinary bladder, urethra and prostate. Br. J. Pharmacol. 147(Suppl 2), S88-119. https://doi.org/10.1038/sj.bjp.0706619 (2006).
Strand, D. W., Costa, D. N., Francis, F., Ricke, W. A. & Roehrborn, C. G. Targeting phenotypic heterogeneity in benign prostatic hyperplasia. Differentiation 96, 49–61. https://doi.org/10.1016/j.diff.2017.07.005 (2017).
Bauman, T. M. et al. Characterization of fibrillar collagens and extracellular matrix of glandular benign prostatic hyperplasia nodules. PLoS One 9, e109102. https://doi.org/10.1371/journal.pone.0109102 (2014).
Cao, Y. et al. The symptoms of benign prostatic hyperplasia patients with stromal-dominated hyperplasia nodules may be associated with prostate fibrosis. Int. J. Gen. Med. 16, 1181–1191. https://doi.org/10.2147/IJGM.S395705 (2023).
Rodriguez-Nieves, J. A. & Macoska, J. A. Prostatic fibrosis, lower urinary tract symptoms, and BPH. Nat. Rev. Urol. 10, 546–550. https://doi.org/10.1038/nrurol.2013.149 (2013).
Yang, Y. et al. Estrogen and G protein-coupled estrogen receptor accelerate the progression of benign prostatic hyperplasia by inducing prostatic fibrosis. Cell Death Dis. 13, 533. https://doi.org/10.1038/s41419-022-04979-3 (2022).
Hennenberg, M. et al. Non-adrenergic, tamsulosin-insensitive smooth muscle contraction is sufficient to replace alpha1 -adrenergic tension in the human prostate. Prostate 77, 697–707. https://doi.org/10.1002/pros.23293 (2017).
Gilfrich, C. et al. Morbidity and mortality after surgery for lower urinary tract symptoms: A study of 95 577 cases from a nationwide German health insurance database. Prostate Cancer Prostatic Dis 19, 406–411. https://doi.org/10.1038/pcan.2016.33 (2016).
Weinstein, I. C. et al. Adoption and outcomes of holmium laser enucleation of the prostate in the United States. Urology 179, 106–111. https://doi.org/10.1016/j.urology.2023.05.028 (2023).
Behr, A. et al. Comparison of surgical procedures for benign prostatic hyperplasia of medium-volume prostates: Evaluation of the causes of rehospitalization from the French National Hospital Database (PMSI-MCO). World J. Urol. 41, 2481–2488. https://doi.org/10.1007/s00345-023-04509-6 (2023).
Magistro, G. et al. Enucleation vs. Resection: A Matched-pair Analysis of TURP, HoLEP and Bipolar TUEP in Medium-sized Prostates. Urology 154, 221–226. https://doi.org/10.1016/j.urology.2021.04.004 (2021).
Tamalunas, A. et al. The clinical value of holmium laser enucleation of the prostate in octogenarians. Low Urin. Tract Symptoms 13, 279–285. https://doi.org/10.1111/luts.12366 (2021).
Bozzini, G. et al. A prospective multicenter randomized comparison between holmium laser enucleation of the prostate (HoLEP) and thulium laser enucleation of the prostate (ThuLEP). World J Urol 39, 2375–2382. https://doi.org/10.1007/s00345-020-03468-6 (2021).
Hein, S. et al. Thermal effects of thulium: YAG laser treatment of the prostate-an in vitro study. World J. Urol. 40, 161–167. https://doi.org/10.1007/s00345-021-03805-3 (2022).
Yilmaz, M. et al. Temperature assessment study of ex vivo holmium laser enucleation of the prostate model. World J Urol 40, 1867–1872. https://doi.org/10.1007/s00345-022-04041-z (2022).
Yilmaz, M. et al. In vivo temperature assessment during holmium laser enucleation of the prostate. Urol Int 107, 363–369. https://doi.org/10.1159/000528849 (2023).
Aldoukhi, A. H., Ghani, K. R., Hall, T. L. & Roberts, W. W. Thermal response to high-power holmium laser lithotripsy. J. Endourol. 31, 1308–1312. https://doi.org/10.1089/end.2017.0679 (2017).
Maxwell, A. D. et al. Simulation of laser lithotripsy-induced heating in the urinary tract. J. Endourol 33, 113–119. https://doi.org/10.1089/end.2018.0485 (2019).
Breitling, C., Nenning, H. & Rassler, J. Necrosis zone depth after bipolar plasma vaporization and resection in the human prostate. Asian J Urol. 10, 144–150. https://doi.org/10.1016/j.ajur.2021.11.002 (2023).
Gilling, P. J., Cass, C. B., Malcolm, A. R. & Fraundorfer, M. R. Combination holmium and Nd:YAG laser ablation of the prostate: initial clinical experience. J. Endourol. 9, 151–153. https://doi.org/10.1089/end.1995.9.151 (1995).
Drake, M. J. et al. Diagnostic assessment of lower urinary tract symptoms in men considering prostate surgery: A noninferiority randomised controlled trial of urodynamics in 26 hospitals. Eur. Urol. 78, 701–710. https://doi.org/10.1016/j.eururo.2020.06.004 (2020).
Lewis, A. L. et al. Clinical and patient-reported outcome measures in men referred for consideration of surgery to treat lower urinary tract symptoms: baseline results and diagnostic findings of the urodynamics for prostate surgery trial; randomised evaluation of assessment methods (UPSTREAM). Eur. Urol. Focus 5, 340–350. https://doi.org/10.1016/j.euf.2019.04.006 (2019).
Michel, M. C. et al. Current and emerging pharmacological targets and treatments of urinary incontinence and related disorders. Pharmacol. Rev. 75, 554–674. https://doi.org/10.1124/pharmrev.121.000523 (2023).
Bailey, K. et al. Urodynamics for Prostate Surgery Trial; Randomised Evaluation of Assessment Methods (UPSTREAM) for diagnosis and management of bladder outlet obstruction in men: study protocol for a randomised controlled trial. Trials 16, 567. https://doi.org/10.1186/s13063-015-1087-1 (2015).
Young, G. J. et al. Statistical analysis plan for the urodynamics for prostate surgery trial; randomised evaluation of assessment methods (UPSTREAM). Trials 18, 455. https://doi.org/10.1186/s13063-017-2206-y (2017).
Acknowledgements
This work was supported by the “Horst-Jürgen-Lühl-Stiftung” [grant number 19-12-2022] Work in the lab is funded by the Deutsche Forschungsgemeinschaft [grant number HE 5825/9-1]. The position of SH in the lab was funded by a scholarship from the China Scholarship Council (CSC) [grant number 202108430037].
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
PK: Conception and design of the work, acquisition and interpretation of data, drafting of the work. SH: Acquisition and analysis of data, substantial revision of the work. LB: Acquisition of data. PN: Acquisition of data. FS: Acquisition of data. AT: Acquisition and interpretation of data, substantial revision of the work. OEK: Acquisition of data, substantial revision of the work. PW: Acquisition of data. RW: Acquisition and interpretation of data. CGS: Conception of the work, acquisition of data. MH: Conception and design of the work, acquisition, analysis and interpretation of data, drafting the work. All authors approved the submitted version, and have agreed to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the wordk, even ones in which the author was not personally involved, are appropriately investigated, resolved and the resolution documented in the literature.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Keller, P., Hu, S., Berger, L. et al. Smooth muscle contractility of laser-enucleated prostate tissues and impacts of preoperative α1-blocker treatment in patients with and without catheterization. Sci Rep 15, 4985 (2025). https://doi.org/10.1038/s41598-025-88884-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-88884-7
