
Abstract
Previous literature has suggested a significant association between loneliness and depression. Importantly, research has shown that rumination can modulate the loneliness–depression relationship. However, most studies only treated loneliness, rumination or depression as unitary constructs. Considering the heterogeneity of the three concepts, we examined the relationship between specific loneliness, rumination items and depressive symptoms using the network analysis approach. In a large community adult sample (N = 900), we constructed the loneliness–depression and loneliness–rumination–depression network using a cross-sectional design. The results suggested that loneliness has no robust association with depressive symptoms. Instead, a connection between a specific ruminative thought (‘think about how alone you are’) and a specific loneliness item (‘how often do you feel alone’) is essential in maintaining the loneliness–rumination–depression network (partial r = 0.307). Our findings indicate that ruminating on the feeling of loneliness is the key underlying factor modulating the loneliness–depression relationship. Interventions for depression should focus on ameliorating ruminative thoughts, especially on loneliness feelings.
Similar content being viewed by others

Main
Depression is one of the most common mental health problems, affecting around 280 million of the population around the world1. During the COVID-19 pandemic in particular there has been a surge in the rate of depressive disorder, with an increase of over 25% within just the first year of the pandemic2.
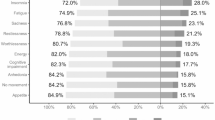
Loneliness has been identified as a critical risk factor for depression throughout the previous literature. Loneliness refers to a distressing state due to the unmet interpersonal needs stemming from a discrepancy between one’s desired social connection and the actual social connection that one receives3. A close relationship between loneliness and depressive symptoms has been consistently supported in both theoretical works (for example, the ‘evolutionary theory of loneliness’ by Cacioppo and Cacioppo4) and multiple empirical studies, such as those reported in refs. 5,6. The Diagnostic and Statistical Manual of Mental Disorders fifth edition (DSM V) diagnostic criteria evaluate depression as the presence of five or more symptoms over two weeks for a major depressive episode. Anhedonia or a depressed mood must be among these symptoms, with others including changes in appetite, sleep disturbances, psychomotor issues, concentration difficulties, fatigue, feelings of worthlessness and suicidal thoughts. Given the widely reported high co-occurrence of loneliness and depression, it is of great importance and urgency to understand the underlying mechanism behind the relationship between loneliness and depression.
One possible way to explain the link between loneliness and depression is by exploring the role of rumination. Rumination is defined as a set of repetitive, intrusive and uncontrollable focuses on one’s negative thoughts and feelings7. Rumination has multiple closely related psychological processes, such as worry, negative mind wandering, self-focus thoughts and so on. The definitions and clear cutoffs between these processes remain unclear in the current literature. However, the common feature shared by these processes is the prolonged and recurrent thinking process post certain stressors, the so-called perseverative cognition. The perseverative cognition hypothesis serves as an important theoretical model elucidating the crucial mediation role of rumination on the pathway between stressors (that is, loneliness) and mental disorders (that is, depression).
Perseverative cognition hypothesis
One important theoretical model, proposed by Brosschot and colleagues8, is the ‘perseverative cognition hypothesis’. In their theory, they state that perseverative cognition can serve as a mediator of the psychopathological pathways through which stressors (both physical and psychosocial stressors) impact health. More specifically, in combination with the theory of Tallis and Eysenck9, worry and rumination, in response to stressors, can disrupt ongoing stressors and trigger the need to look for coping strategies, thus eliciting acute stress responses. However, under chronic stress, perseverative cognition can prolong stressor and stress responses, which continuously activate and maintain the unresolved threatening situations. Furthermore, perseverative cognition overly prepares an organism for action, keeping the individual in a hypervigilant state in preparation for potential threats, even without the actual existence of a stressor. The prolonged state of action readiness and vigilant state have long-term impacts on health through excessive activation of the cardiovascular system, immune functioning, the hypothalamic–pituitary–adrenal axis and other core life-supporting physiological systems10. The chronic pathogenic state can eventually develop into future organic diseases8.
According to their theory, Brosschot and colleagues8 hypothesized that a stressor would not have a direct impact on health if there was no perseverative cognition about the stressor that maintained the mental representation of it and prolonged the physiological activation. They thus state that perseverative cognition plays a critical part in mediating the way in which chronic stress becomes detrimental to our physical and mental health. In line with perseverative cognition theory, we can speculate that loneliness, as a specific stressor, can exert its impact by contributing to the development of depression indirectly through the prolonged cognitive representation of the loneliness feelings elicited by rumination.
Empirical evidence
Some studies have advocated that rumination and depression are highly associated with each other11,12, and the relationship between rumination and loneliness has also been repeatedly supported across studies12,13. Furthermore, an increasing number of recent studies have proposed the potential transdiagnostic role of rumination in the loneliness–depression relationship. For example, researchers have demonstrated that loneliness is associated with depressive symptoms through the mediating effects of rumination14,15,16. However, other studies have found a moderating effect of rumination for specific types of loneliness (for example, parent-related loneliness), where individuals with a higher loneliness in terms of their relationships with parents, together with a higher level of rumination, are more vulnerable to depression development15. Altogether, previous studies have postulated that rumination can be critical in explaining the effects of loneliness on depression.
Multidimensionality issues
However, most of the studies only conceptualized the three concepts at an aggregate level. For example, studies usually operationalize depression as a single disorder using the sum of scores from a self-report questionnaire. However, the manifestation of depression is known to be heterogeneous, with varied symptom combinations across individuals. Park and colleagues17 identified a total of 119 distinct depression patterns stemming from diverse depressive symptom combinations. Furthermore, the complexity of depression treatment was underscored by the work of Park and Kim18, who identified 227 unique symptom combinations meeting DSM V diagnostic criteria. Studies have also suggested that different depressive symptoms are related to different cognitive risk factors, indicating that each specific depressive symptom can carry different characteristics19,20. Moreover, the contemporary psychopathological network paradigm proposes a causal system among symptoms causing each other to form a mental disorder21. Treating depression as a single disorder may ignore the potential causal relationships among depressive symptoms. As such, we propose to reconceptualize depression more at a symptom level, considering the unique contents carried by each depressive symptom and the causal relationships among them.
Similarly, studies have highlighted the multidimensionality of rumination. A recent study by Bernstein and colleagues22 systematically explored the network structure of rumination. In the rumination network, they found that different items, even within the same subscales, interconnected differently with other items within or outside the subscales. Treating rumination as a unitary construct may mislead people that all the items within a scale or subscale are measuring the same things. However, only a few recent studies have begun to examine the effects of specific ruminative thoughts23. The existence of diverse potential subpatterns within each scale underscores the limitation of relying solely on the broader term, or these subfactors to capture the entirety of these complex constructs.
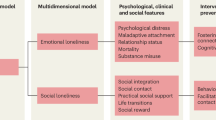
Researchers have also tried to consider the multifaced nature of loneliness. For example, studies have categorized loneliness into different facets, such as emotional versus social loneliness (two basic types of loneliness24), existential loneliness25 or three-faceted constructs (intimate versus relational versus collective loneliness26). Although researchers have not yet reached agreement as to the structure of loneliness, this suggests a need to treat loneliness as a multifaceted construct. However, studies that included loneliness using more specific items are scarce27. The UCLA Loneliness Scale is one of the most widely used scales to measure loneliness. Previous factor analyses have shown that the scale can be factorized into three constructs of loneliness: intimate loneliness, relational loneliness and collective loneliness26. The absence of consensus on the precise factor structure of the UCLA Loneliness Scale indicates potential underlying subpatterns within the construct. We thus suggest treating the UCLA Loneliness Scale more at an item level to take into account the different loneliness constructs measured through the scale.
Admittedly, using total scores to describe the relationships between loneliness, rumination and depression can give us a general idea of their relationships. To better understand the complex psychological relationships in more detail, we should also look into the interconnections among variables at an item level. However, to the best of the our knowledge, no study has yet examined the relationship between individual items of loneliness and rumination and depressive symptoms all at once.
Considering the above literature review, the present study will take a first step to examine the relationship between specific loneliness items, rumination items and individual depressive symptoms using a network analysis approach in a cross-sectional study. Previous studies have suggested that there is a large gender difference in the prevalence of depression28. Studies have also shown mixed effects of gender differences in loneliness (for example ref. 29). According to the previous literature, gender can be an important factor in influencing the behavior of the network structure (for example, the network may be more connected for women than for men). Therefore, a network comparison between women and men subsamples was conducted following the general network analysis. The aims of the present study are twofold. First, we aim to establish the relationship between loneliness, rumination and depression using their total scores to confirm the mediation effects of rumination, in line with previous research. Second, to achieve a more in-depth understanding of the relationship, we will construct a network of loneliness and depressive symptoms and a network of loneliness, rumination and depressive symptoms using more specific items. We hypothesize that rumination mediates the relationship between loneliness and depression, with a higher level of loneliness predicting more rumination, which will, in turn, predict a higher severity of depression. We also hypothesize that in the network analysis, specific loneliness items, rumination items and depressive symptoms will be positively related to each other.
Results
Sample characteristics
Two participants below the Montreal Cognitive Assessment (MoCA) cutoff score of 22 were excluded. Two participants were also excluded from the analyses due to voluntary withdrawal from the study or a large amount of missing data on the variables of interest. A final sample of 900 adults (68.3% women, Mage = 26.25 years, s.d.age = 13.35) were included in the analyses. Complete descriptive statistics are presented in Table 1.
Mediation model
Spearman’s correlations suggest that loneliness, rumination and depression are significantly positively correlated with each other (Supplementary Table 1). Spearman’s correlations were examined between loneliness and rumination (ρ = 0.68, P < 2 × 10−16), loneliness and depression (ρ = 0.19, P < 2 × 10−16) and rumination and depression (ρ = 0.17, P < 2 × 10−16).
Mediation analysis (Fig. 1) was performed to examine the role of rumination in the loneliness–depression relationship. The total effect of loneliness on depression was significant (bootstrapped total effect = 0.193, 95% confidence interval (CI) [0.169, 0.220]). Loneliness was significantly associated with rumination, and a higher level of loneliness statistically predicted more ruminative thoughts (ρ = 0.680, 95% CI [0.614, 0.744]). Rumination was significantly associated with depression, with more ruminative thoughts statistically predicting more depression (ρ = 0.120, 95% CI [0.092, 0.148]). The direct effects of loneliness on depression were significant (bootstrapped direct effect = 0.112, 95% CI [0.083, 0.141]) The indirect effects of loneliness on depression through rumination were significant (bootstrapped indirect effect = 0.081, 95% CI [0.061, 0.104]). Therefore, rumination mediated the loneliness–depression relationship.

Loneliness is the independent variable, rumination the mediating variable and depression the dependent variable. Total effects (c) and direct effects (c′) are also illustrated in the model.
Network robustness checks
The robustness check contains two components that support the credibility of the constructed networks. For network accuracy and stability, the non-parametric bootstrap procedure for the edge weights of both networks (Supplementary Fig. 1a,c) has a narrow 95% CI, indicating excellent accuracy. Case-dropping subset bootstrapping on the edge and centrality indices of both networks (Supplementary Fig. 2) suggests excellent stability for the edge weights and node expected influence (EI) over other centrality indices. As such, the present study reports the node EI for node centrality. The stability of the edge weights and node EI of the loneliness–depression network was excellent (both with a correlation stability (CS) coefficient of 0.75). The stability of the loneliness–rumination–depression network is excellent (CS-coefficient = 0.75) for node EI and good (CS-coefficient = 0.672) for edge weights. The bootstrapped difference test of the edge weights of the two networks suggests that most of the edges are significantly different from each other (Supplementary Fig. 3a,c).
The case-dropping bootstrap results of bridge centrality indices (bridge EI and bridge strength) are shown in Fig. 2b,d. The bridge centrality of the loneliness–depression network is not stable (CS-coefficient of bridge strength = 0.128; CS-coefficient of bridge EI = 0.128). The loneliness–rumination–depression network has stable bridge EI (CS-coefficient = 0.594) but unstable bridge strength (CS-coefficient = 0.206). The bridge EI of both networks indicates better network accuracy, with a narrower 95% CI after the non-parametric bootstrap, compared to bridge strength (Fig. 2a,c). Accordingly, the present study reports bridge EI as the indicator of bridge centrality. Supplementary Fig. 1b,d presents the non-parametric bootstrap results of the bridge strength of the two networks.

The non-parametric bootstrap method estimates the accuracy of the bridge EI. Red dots represent each node’s corresponding bridge EI, from the highest to the lowest. Gray shading represents the 95% CI for the bridge EI. A narrower gray shadow means better accuracy for the bridge EI. The case-dropping bootstrap method increasingly dropped cases from the original sample and compared the centrality indices in the new versus the original dataset. The x axis indicates the proportion of the dataset that can be dropped. The y axis represents the correlation between the original bridge centrality indices and those after the cases were dropped with a 95% probability. The shades represent the 95% CI for the bridge centrality indices. a, Accuracy of the bridge EI of the loneliness–depression network. b, Stability of bridge centrality indices: bridge strength and bridge EI (one-step) of the loneliness–depression network. c, Accuracy of the bridge EI (one-step) of the loneliness–rumination–depression network. d, Stability of bridge centrality indices: bridge strength and bridge EI (one-step) of the loneliness–rumination–depression network.
In terms of the network comparison test on the two subsamples randomly split from the original dataset, neither the network invariance test (M (maximum statistic) = 0.322, P = 0.0500) nor the global strength invariance test (S (distance) = 0.381, P = 0.707) suggests any substantially significant differences between the two network structures. Visual examination also supports a similar structure for the two networks (Supplementary Fig. 4a,b). For the networks of both subsamples, the most influential bridge symptoms are L4 (‘how often do you feel alone’) and R1 (‘think about how alone you feel’, partial r = 0.253 and 0.378, respectively, for the two subsamples), bridging the loneliness and rumination communities (Supplementary Fig. 4c,d). The network structure and central bridge symptoms found in the two subsamples support the reliability and credibility of the network structure and bridge symptoms found in the original dataset and described in the following sections.
Bridge and node centrality
Figure 3 presents the network structures of the loneliness–depression and loneliness–rumination–depression networks. The bridge symptom with the highest bridge EI in the loneliness–depression network is D7 (‘trouble concentrating on things’). The symptom of loneliness that D7 most strongly connected with is L11 (‘how often do you feel left out’, partial r = 0.094). However, the bridge centrality of the loneliness–depression network should be interpreted with caution, as the case-dropping bootstrap procedure indicated poor stability of the bridge centrality indices. In the loneliness–rumination–depression network, the bridge symptoms with the highest bridge EI, significantly different from other bridge symptoms, are L4 (‘how often do you feel alone’) and R1 (‘think about how alone you feel’). L4 is most strongly connected to R1 (partial r = 0.307). Similarly, R1 is most strongly connected to L4 (partial r = 0.307). Supplementary Tables 2 and 3 present the edge weight matrices of the two networks. Illustrations of the full bridge EI plot and its bootstrapped difference test results are provided in Fig. 4b,d and Supplementary Fig. 5.

a,b, Network structures of loneliness and depressive symptoms (a) and loneliness, rumination and depressive symptoms (b) in 900 adults. Each community is colored to represent the variables of interest in this study (namely, loneliness, rumination and depression). The nodes belonging to the same community are assigned the same colors. Blue nodes represent individual items from the UCLA Loneliness Scale version 3. Green nodes represent individual items from the Ruminative Responses Scale (RRS). Purple nodes represent specific depressive symptoms from the Patient Health Questionnaire (PHQ). The thickness and length of the edges represent the strength of the partial correlation between the two nodes, with thicker or shorter edges representing a larger partial correlation between nodes. The colors of the edges represent the directionality of the partial correlation between nodes, where blue indicates a positive partial correlation and red a negative partial correlation. Bridge symptoms are highlighted in yellow, keeping the nodes above the 80% percentile of the bridge EI by convention43.

The EI (one-step) and bridge EI (one-step) were used in the present study. One-step EI is defined as the sum of all the edges extending from a node, including both negative and positive ones. One-step bridge EI is the sum of edge weights extending from one node to all nodes in other communities. a,b, EI (a) and bridge EI (b) of each node, from the highest to the lowest, of the loneliness–depression network. c,d, EI (c) and bridge EI (d) of each node, from the highest to the lowest, of the loneliness–rumination–depression network.
Figure 4a,c and Supplementary Fig. 3b,d illustrate the node EI plot and the bootstrap difference test results of the two networks. The central nodes with significantly higher node EI over the other nodes in the loneliness–depression network are L14 (‘how often do you feel isolated from others’) and D2 (‘feeling down, depressed or hopelessness’). The nodes with significantly higher EI in the loneliness–rumination–depression network are R6 (‘think about how passive and unmotivated you feel’), L4, L14 and R11 (‘go away by yourself’) and R17 (‘think about how sad you feel’).
Directed acyclic graph
Figure 5 presents directed acyclic graphs for the loneliness–depression and loneliness–rumination–depression networks. In the loneliness–depression graph, nodes of loneliness and depression are only connected to the nodes within their own communities, without any interconnection between the two communities. In the loneliness–rumination–depression graph, nodes from loneliness generally point to rumination nodes, which point to the depression community. Paths can be found linking the loneliness, depression and rumination communities through important bridge symptoms identified in the previous section. For example, R1 points to L4, which then points to D2. Other paths suggest a link between loneliness and depressive symptoms through rumination. For example, L7 (‘no longer closer to others’) and L12 (‘relationships with others are meaningless’) point to R19 (‘not feel up to doing anything’), which points directly to R4 (‘hard to concentrate’) or indirectly through R18 (‘think about shortcomings’), R16 (‘think “Why can’t I handle things betterˮ’) and R14 (‘not able to concentrate’) to R4. R4, in the end, points to D7 and other specific depressive symptoms.

a, Directed acyclic graph of the loneliness–depression network. b, Directed acyclic graph of the loneliness–rumination–depression network. This approach draws the possible directional links between individual items in the network by considering their conditional independence relationships.
Subsample network comparisons
To examine the effects that gender may have on a network, we constructed a loneliness–rumination–depression network for subsamples of women (N = 615) and men (N = 285), as illustrated in Supplementary Fig. 6. In particular, the women’s network has good edge stability (CS-coefficient = 0.595) and excellent node EI stability (node EI = 0.75), but unstable bridge EI (bridge EI CS-coefficient = 0.439; Supplementary Figs. 7 and 9). In comparison, the men’s network shows poor stability in either edge or bridge centrality indices (CS-coefficient edge = 0.361, bridge EI CS-coefficient = 0.126), but good stability in its node EI (CS-coefficient = 0.516; Supplementary Figs. 8 and 9). Supplementary Fig. 10 shows the full node centrality and bridge EI plots of both networks.
The network comparison test (NCT) with Holm–Bonferroni correction did not find significant differences in the network structure (network invariance test: M = 0.294, P = 0.257) or overall symptom connectivity (global strength invariance test: S = 1.571, P = 0.146).
Discussion
Going beyond traditional conceptualization and methodology, the present study utilizes network analysis to understand the relationship between specific loneliness items, rumination items and individual depressive symptoms. Specifically, we found no robust direct connection between individual loneliness items and depressive symptoms. Instead, ruminating on loneliness feelings was found to play an important role in mediating the loneliness–depression relationship.
Our two major hypotheses were satisfied by the study. First, in the mediation model, rumination indeed mediated the relationship between loneliness and depression. Our second hypothesis was also satisfied. In the loneliness–depression network, the present study did not reveal stable bridge symptoms due to the poor reliability of the bridge centrality indices. The instability of the loneliness–depression only network means that the two constructs are not the whole picture. Note that a high correlation between loneliness and depression does not equate to a causal relationship that loneliness will always trigger depression or vice versa. Therefore, in the present study, the loneliness–depression network indicated that the activation of the loneliness community alone is not stably associated with the manifestation of specific depressive symptoms. It explains, in real practice, why some individuals with a high level of loneliness may not necessarily connect to depressive symptoms.
In the loneliness–rumination–depression network, we found two influential bridge symptoms: L4 (‘frequently feeling alone’ thereafter) and R1 (‘ruminating on loneliness’ thereafter). In particular, ‘frequently feeling alone’ most strongly connects to other communities through the bridge symptom ‘ruminating on loneliness’. Similarly, ‘ruminating on loneliness’ also has the strongest connection to ‘frequently feeling alone’. The strong connection between the two nodes makes it the most influential pair of connections essential to the loneliness–rumination–depression network. In other words, frequently feeling loneliness and subsequently ruminating on the feeling of loneliness together can activate and sustain the close relationship between loneliness, rumination and depressive symptoms.
Our findings can be explained by previous theoretical works. In line with the Perseverative Cognition Hypothesis8, the stressor (here, loneliness) leads to health damage (that is, depressive symptoms) through the effect of rumination. In our study, the maladaptive way of coping with the stressor—in this case, ruminating on the loneliness feelings—can be the reason why loneliness can result in the development of further depressive symptoms. Especially during the pandemic, due to the Chinese government’s compulsory implementation of social distancing policies, people had less chance to gather with their socially significant others and form or maintain their social bonds in person. Social activities are especially important for younger adults (the primary participants of the present study), who require a larger amount of social connection with their friends and colleagues compared to other age groups. With the decrease in social activities, mismatches between the actual and desired social connections resulted in an elevation of loneliness levels among young adults. In response to chronic interpersonal stress, people started to ruminate the loneliness feelings repeatedly, maintaining the stressful responses in the long term. Furthermore, social distancing policies hindered lonely individuals from reconnecting with others and removing themselves from a fixation on loneliness, further exacerbating the negative impacts of rumination on mental health. This prolonged rumination in response to loneliness can, in turn, elicit sustained physiological responses to chronic stress, which eventually leads to negative impacts on health, such as developing depressive symptoms30.
Our results are also consistent with previous empirical studies. A previous network analysis of rumination using the Ruminative Responses Scale (RRS) showed that thinking about how lonely one feels is among the most central nodes with the highest bridge EI in the rumination network22. Our study goes beyond previous works and elucidates how ruminating on loneliness contributes to explaining the association between loneliness and depressive symptoms. A recent study by Everaert and colleagues23 revealed that ruminating on feelings of loneliness repeatedly and stably emerged as one of the best predictors of the central symptoms of depression. In line with these previous studies, we demonstrated that ruminating on loneliness is central in contributing to the loneliness–depression relationship. People may question whether our results are due to original overlaps between the content of the three questionnaires. In response to this, we confirm that our chosen questionnaires possess excellent face validity to assess the three constructs in the present study. Specifically, the UCLA Loneliness Scale focuses on subjective perceptions of social interactions, whereas RRS centers on the repetitive contemplation of past events. The UCLA Loneliness Scale and RRS distinctly measure separate constructs, with the former assessing subjective evaluations of interpersonal relationships and the latter addressing intrusive cognitive patterns concerning past feelings and events. In comparison, PHQ-9 targets depression, emphasizing maladaptive emotional and somatic states. The UCLA Loneliness Scale and PHQ-9 evaluate disparate aspects, with the former concentrating on subjective feelings specifically regarding interpersonal relationships and the latter scrutinizing individuals’ historical and current mood states and somatic discomfort. Furthermore, the distinctions between RRS and PHQ-9 are evident, as RRS examines a maladaptive cognitive loop entailing repetitive recollections of past events, and PHQ-9 directly delineates abnormal mood states through various mood-related issues, cognitive challenges and somatic symptoms. These distinctions indicate that each questionnaire uniquely measures separate constructs. Therefore, the observed connections between items from the loneliness and rumination clusters in our results probably reflect meaningful associations bridging across distinct constructs rather than indicating content overlap among the scales.
Our findings also have some inconsistencies with the previous literature. For example, we did not find any depressive symptoms as influential bridge symptoms. This could be due to the characteristics of the current dataset, with most of the participants having minimal or lack of a clinical diagnosis of depressive disorders. It is possible that community participants were still at the early stage where rumination started to exacerbate the negative effects of loneliness on depressive symptoms, but they had not yet reached the full development of depression. As such, the connection between loneliness and rumination is more a determinant in the network at the current stage. This interpretation implies that focusing on reducing the ruminative thoughts on loneliness is essential in breaking the loneliness–depression association, especially for the community population at an earlier development stage of depression. Moreover, Everaert and colleagues23 also worked on exploring the rumination–depression relationship at the item level and found that both thinking ‘Why can’t I get going’ and rumination on loneliness feelings are among the cardinal items to predict future depressive symptoms. In our study, however, we only confirmed the important role of ruminating on loneliness. This could be due to methodology differences. For example, the unique contents covered by different questionnaires used in different studies may influence results.
The present study has multiple clinical implications. Researchers have suggested that deactivating bridge symptoms is the more effective way to deactivate the whole network compared to using symptoms based on other centrality indices31. As such, by removing or disrupting the connection between ‘frequently feeling alone‘ and ‘ruminating on loneliness’, we may begin to deactivate the network of loneliness, rumination and depression and alleviate the adverse effects of loneliness on depression. Therefore, we suggest that ruminative thoughts on loneliness feelings can be a critical target for effective intervention preceding the full clinical development of depression for people with high loneliness. For example, psychotherapy such as cognitive behavioral therapy (CBT) could intentionally add cognitive training content targeting specific people with high loneliness to reappraise the negative feelings of rumination rather than ruminating on them. In addition, studies have found that rumination is a vital factor in explaining treatment resistance in depressive disorders32. As such, focusing on ruminative thoughts can also improve the treatment effects and decrease the treatment resistance of depressive disorders. However, identifying and targeting one specific kind of ruminative thought alone can be difficult in practice. Therefore, future studies should also consider how to specifically deactivate certain ruminative content for better practice.
The current study is not without limitations. First, the study recruited from a community population, with most participants being women. However, we have conducted network comparison tests to compare gender-stratified subsamples. The results suggest no significant difference between the two networks observed. This could be due to the characteristics of our dataset being mostly composed of women or due to the fact that our results were less likely driven by gender. In spite of this, future studies should try to use a more balanced sample to avoid the bias of the results and also try using clinical samples to see whether our results can be generalized to clinical settings as well. Second, this is a cross-sectional study that can only suggest correlations but not causations. However, we utilized the directed acyclic graph to infer putative causal links. The directional links drawn from loneliness to depression through rumination imply that loneliness can trigger specific ruminative thoughts, which eventually lead to more specific depressive symptoms. The findings form important first evidence of correlational relationships, and future studies are encouraged to validate our findings using a longitudinal design. Third, the scales we used to operationalize loneliness or rumination may not exhaustively capture the contents of the concept. For example, Maes and colleagues33 reviewed the current conceptualization and measurements of loneliness, and suggested that most of the scales captured social and emotional loneliness but not other types (for example, existential or collective loneliness), which usually receive less attention. In terms of rumination, researchers have also discussed including the motivational, behavioral and metacognitive contents of rumination in addition to the cognitive construct13. Admittedly, the conceptualization and operationalization of the three constructs are not comprehensive enough. We are just tapping part of the construct based on widely accepted definitions and measurements we chose to use. By no means are we referring to our findings as thorough enough to explain every aspect of rumination, loneliness or depression. We acknowledge the inherent limitations of our study in fully capturing the complexity of rumination, loneliness and depression, and we understand that modifications to definitions or measures could impact our specific findings. Some may argue for a replication study. However, we may encounter practical challenges that necessitate our reliance on the UCLA Loneliness Scale and RRS in particular. Introducing lesser-known measures could hinder interpretability and comparability. Our study’s specific definitions align with ongoing debates in the literature about loneliness, rumination and depression definitions. Although this may limit generalizability, we highlight the need for future research to refine construct definitions and develop comprehensive measurement tools. Despite these limitations, the chosen questionnaires demonstrate sufficient face validity and prior validity, supporting their use in our study and suggesting potential for further refinement in future studies. Fourth, the network structures and results should be interpreted or generalized with caution, as we only utilized one commonly used scale for each of the three concepts in a community population from China. Nevertheless, we have included a robustness check with an examination of network accuracy and stability and a split-halves network comparison test to increase the credibility of our results. Future studies are encouraged to replicate the current findings using other loneliness, rumination or depression scales or using different populations from different cultural backgrounds to increase the generalizability of the current findings.
Altogether, ruminating on the feeling of loneliness is the most influential factor that contributes to modulating the loneliness–depression relationship. This finding emphasizes the importance of considering the heterogeneity of depression and the multidimensionality of loneliness and rumination. Future studies are recommended to further replicate the current study and target resolving ruminative thoughts to alleviate the effects of loneliness on depressive symptoms.
Methods
Participants
A sample of 904 adult participants were recruited from the community population residing in Hong Kong, Guangzhou and Fuzhou, China, between 2021 and 2023 during the outbreak of the COVID-19 pandemic. A Montreal Cognitive Assessment (MoCA) was conducted during the screening. Any participants who scored below 22, a cutoff score validated in Chinese older populations34, was regarded as having cognitive impairments and excluded from the final analysis.
Ethical approval of the project was obtained from the Human Research Ethics Committee of the affiliated institute of the first author and the last corresponding author (Human Research Ethics Committee ref. no. EA200161). All participants provided informed consent at the beginning of the study. They were notified of the potential harms and benefits of the study and their right to exit the study at any time. Participants who voluntarily gave their consent completed a series of questionnaires. Participants received no more than HK$80 for compensation.
Questionnaires
The questionnaires included measures of loneliness, rumination, depression, demographic characteristics and a variety of other individual features as part of a larger project.
Loneliness was measured through one of the most widely used scales, the UCLA Loneliness Scale version 3 (UCLA-3 Loneliness Scale35). The UCLA-3 Loneliness Scale includes 20 items with 11 positively worded items (for example, ‘How often do you feel left out’) and nine negatively worded items (for example, ‘How often do you feel close to people’). Participants were instructed to indicate the frequency of their feelings of loneliness on a four-point Likert scale from 1 (never) to 4 (often). A higher score in positively worded items represents a higher level of loneliness. For negatively worded items, we reversely coded the items so that a higher score represented a higher level of loneliness. The UCLA Loneliness Scale has wide applicability. For instance, recent reviews on loneliness included studies that exclusively use the UCLA Loneliness Scale, suggesting the wide usage of the measure of loneliness36. Studies among parents of children with autism spectrum disorder (ASD), college students and older adults in China have repeatedly utilized the UCLA Loneliness Scale37,38,39. We adopted a validated Chinese version that has high internal consistency (Cronbach’s α = 0.85; ref. 40). The internal consistency of the items of the scale in the present sample is excellent (MacDonald’s ω = 0.91). Our factor analyses reveal strong internal validity of the UCLA Loneliness Scale, with high item loadings (above 0.5) across most items. Previous research consistently supports its external validity and reliability across various populations and settings (for example refs. 35,41). A recent review42 confirmed the scale’s good content validity and reliability, with widespread application in diverse contexts such as patients with diabetes43 and COVID-1944.
Rumination was evaluated using the 22-item RRS45, derived from the Response Styles Theory of Nolen-Hoeksema7. The scale was scored on a four-point Likert scale from 1 (almost never) to 4 (almost always). The questionnaire asked participants how frequently they generally do or think as the statements in the questionnaire. An example of a questionnaire item is ‘Think about how passive and unmotivated you feel’. A higher score indicates a higher level of ruminative response style. Recent reviews have utilized RRS as a measure of rumination, suggesting its wide usage (29 out of 58 studies in the review of Nagy and colleagues46; Stade and Ruscio47; exclusively for RRS, Stelmach-Lask and colleagues48). The RRS has also been extensively used in studies involving Chinese adolescents, individuals with mood disorders, and college students (for example, refs. 49,50). We adopted the Chinese version with good internal consistency reliabilities (Cronbach’s α = 0.90; ref. 51). The scale has excellent internal consistency for the present sample (MacDonald’s ω = 0.95). Our factor analysis for the RRS indicates strong internal validity, with most items showing high loadings on a single factor. Past research, including studies by Treynor and colleagues45 and Liang and Lee49, has demonstrated the good test–retest correlations and reliability of the RRS, particularly in Chinese samples across genders and in adolescents.
Depression was assessed by the PHQ-952. The nine items from the PHQ-9 were designed based on the DSM-IV diagnostic criteria for depressive disorder53. Participants were asked about the frequency of suffering from depressive symptoms in the past two weeks. Examples of depressive symptoms are ‘Feeling down, depressed or hopeless’ and ‘Feeling tired or having little energy’. The questionnaire utilized a four-point Likert scale, ranging from 0 (not at all) to 3 (nearly every day). A higher score for an item represents a higher severity of the specific depressive symptom. The PHQ-9 is a commonly utilized tool for measuring and tracking depression in large-scale samples given the short length of the questionnaire. Studies have systematically reviewed the wide use and good sensitivity and specificity of PHQ-9 in primary-care settings54. PHQ-9 has also been widely adopted in measuring depression among Chinese populations, as evidenced by its inclusion in various studies among Chinese college students55. The Chinese version adapted by Yu and colleagues56 also suggests excellent internal consistency (Cronbach’s α = 0.82), comparable to the English version in a primary-care study (Cronbach’s α = 0.89). The internal consistency of the questionnaire in the present sample is good (MacDonald’s ω = 0.87). Our factor analysis suggests good factor loadings of all items on one factor. Research indicates strong reliability and test–retest correlations of the PHQ-9 with other depression scales and professional mental health diagnoses52,54,57. Recent reviews, such as by Levis and colleagues57, underscore PHQ-9’s exceptional sensitivity in screening major depression, surpassing semistructured diagnostic interviews, and highlighting its reliability in clinical contexts.
Data analysis
We first conducted Spearman correlations among loneliness, rumination and depression using their total scores to confirm the correlations between them as unitary constructs. We specifically chose to use the Spearman’s correlation test because it is a non-parametric test that does not require the satisfaction of normality assumption, which is more suitable for the present dataset.
A mediation model was then drawn between loneliness, rumination and depression. The model defined loneliness as the independent variable, rumination as the mediating variable, and depression as the dependent variable. All paths, total effect, direct effect and indirect effect, were evaluated using bootstrapped 95% CIs with 5,000 bootstrap samples. The mediation effect of rumination was regarded as significant if the 95% CIs did not include zero.
The data were then analyzed using a network analysis approach following a cross-sectional design. Network analysis is an advanced statistical analytic strategy. Network analysis focuses on how individual items connect within and across the larger variables58 and how these connections influence the behavior of the network to explain the larger phenomena59. Network analysis can help address the heterogeneity of larger concepts and thus contribute to better capturing how individual items play roles within and outside their own concept clusters. Specifically, the bridge symptoms in a network can be essential in linking the clusters of symptoms between different disorders or conditions and thus transferring the activation from one disorder or condition to another. Therefore, interventions or treatments targeting the most influential bridge symptoms in a network can be effective in ameliorating the co-occurrence of multiple maladaptive conditions. The whole analysis was performed in R version 4.1.360 using the psych version 2.3.361, lavaan version 0.6.1562, bootnet version 1.563, qgraph version 1.9.364, networktools version 1.5.065, pcalg version 2.7.866 and NetworkComparisonTest version 2.2.167 packages.
Estimation of network structure
The graphical least absolute shrinkage and selection operator (LASSO) algorithm and the extended Bayesian information criterion (EBIC) were used to obtain the optimal partial correlation network structure using the bootnet package63. Spearman partial correlation was used as recommended and widely accepted across the literature68. The network was visualized with each item of the questionnaire depicted as a node and the line that interconnects between two nodes as an edge.
Network centrality indices
The centrality indices of the weighted networks were calculated and visualized using the CentralityPlot function from the qgraph package64. Traditional centrality indices, including strength, closeness, and betweenness, have all been used commonly in previous studies. However, recent research has pointed out the unreliability of using closeness and betweenness in assessing the centrality role of nodes69. In addition, studies argue that strength cannot accurately capture the centrality of nodes when one node has both negative and positive edges69. On the other hand, the one-step EI is defined as the sum of all the edges extending from the node, considering both negative and positive ones. Therefore, following the suggestions of Robinaugh and colleagues70, we focused on reporting the EI (one-step) as the indicator of centrality in the present analyses. For the sake of completeness, we also report other centrality indices (for example, strength, closeness and betweenness) in Supplementary Fig. 11.
Network robustness checks
The robustness checks contain two components. The first includes the estimation of network stability and accuracy. The second includes a network comparison test on two subsamples from the original larger sample randomly split into halves to examine the replicability of the loneliness–rumination–depression network structure.
Network stability and accuracy were evaluated by two bootstrap approaches using the bootnet package63. The non-parametric bootstrap procedure with 1,000 permutations was used to assess the accuracy of the edge weights by generating a 95% CI through random sampling of the original dataset. A narrower CI suggests good network accuracy. A case-dropping bootstrap method with 1,000 permutations was used to capture the stability of the centrality indices and edges. The CS-coefficient was obtained from the bootstrapping, and indicates the maximum proportion of the dataset that can be dropped while maintaining the correlation between the original centrality indices or edges and those after case-dropping above at least 0.7 (by default) with 95% probability. By convention, a CS-coefficient above 0.7 indicates excellent stability. A CS-coefficient above 0.5 but below 0.7 represents good stability. A CS-coefficient below 0.5 indicates poor stability63. The results from the case-dropping bootstrap test can also be used to support our selection of central indices in the present analyses (details are presented in the Results). Bootstrapped difference tests were performed at the end to evaluate the significance of the centrality indices of one node or edge compared to the others71.
A network comparison test was carried out on the two randomly split halves from the original dataset using the ‘NetworkComparisonTest’ package67. The original dataset was randomly split into two datasets with 450 participants in each subsample. The network comparison test was performed on the loneliness–rumination–depression networks of the two subsamples using 1,000 iterations with two major tests: (1) network invariance test to examine whether any edges in the two networks are different and (2) global strength invariance test to examine any differences in the overall edge connectivity. Finally, the two subsample networks were compared for the parameters that are meaningful for the current studies (for example, the most influential bridge symptoms, the bridge connections between communities, and so on).
Bridge symptoms
To illustrate the nodes that play essential roles in bridging between clusters of items belonging to the same larger variable, or communities, we used the bridge function from the networktools package65 to evaluate the bridge symptoms in the network. Similarly, we selected to report the bridge EI (one-step) for the centrality of the bridge symptoms70. One-step bridge EI is the sum of edge weights extending from one node to all nodes in other communities. Supplementary Fig. 12 presents other bridge indices (for example, bridge strength). Studies have suggested that activation of the nodes with the highest bridge EI are the most influential in activating other communities65. Non-parametric and case-dropping bootstrap procedures were also performed to evaluate the stability and accuracy of the bridge centrality indices.
Complete partially directed acyclic graph
To explore the potential directional influence between individual items in the network, a directed acyclic graph approach was applied to the estimated network using the ‘pcalg’ package66. A directed acyclic graph is a type of Bayesian network that draws the possible directional links between individual items in the network by considering their conditional independence relationships71. Such directed acyclic graphs can help reveal the most possible causal processes in cross-sectional observational datasets. The function of causal inference allows for identifying the potential risk factors or optimizing intervention targets preceding certain adverse processes71.
Network comparison by gender
Finally, to understand whether the networks are different for women versus men, we also examined the potential gender differences in loneliness–rumination–depression networks by doing a network comparison test using the NetworkComparisonTest package67. We performed difference tests between the networks of subsamples (women versus men) using 1,000 iterations. Two general hypothesis tests were conducted for the two networks: (1) a network invariance test, whose null hypothesis states that all corresponding pairs of edges in two networks are the same, and (2) a global strength invariance test, which examines the overall edge connectivity in a network. Differences in each individual edge and centrality indices between the two subsamples’ networks were also evaluated. Holm–Bonferroni correction was adopted to adjust the P value of the result for multiple comparisons.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this Article.
Data availability
The minimum anonymized data that support the findings of this study are available upon reasonable request from the corresponding authors. The participants did not consent to the sharing of the raw data to the public. Source data are provided with this paper.
Code availability
No custom code was used in this study.
References
Institute of Health Metrics and Evaluation. Global Health Data Exchange (GHDx) https://vizhub.healthdata.org/gbd-results/ (IHME, 2019).
World Health Organization. COVID-19 Pandemic Triggers 25% Increase in Prevalence of Anxiety and Depression Worldwide https://www.who.int/news/item/02-03-2022-covid-19-pandemic-triggers-25-increase-in-prevalence-of-anxiety-and-depression-worldwide (WHO, 2022).
Peplau, L. A. & Perlman, D. in Loneliness: A Sourcebook of Current Theory, Research and Therapy (eds Peplau, L. A. & Perlman, D.) 1–18 (Wiley, 1982).
Cacioppo, J. T. & Cacioppo, S. in Advances in Experimental Social Psychology (ed. Olson, J. M.) Vol. 58, 127–197 (Academic Press, 2018).
Erzen, E. & Çikrikci, Ö. The effect of loneliness on depression: a meta-analysis. Int. J. Soc. Psychiatry 64, 427–435 (2018).
Lee, C. M., Cadigan, J. M. & Rhew, I. C. Increases in loneliness among young adults during the COVID-19 pandemic and association with increases in mental health problems. J. Adolesc. Health 67, 714–717 (2020).
Nolen-Hoeksema, S. & Morrow, J. A prospective study of depression and posttraumatic stress symptoms after a natural disaster: the 1989 Loma Prieta earthquake. J. Pers. Soc. Psychol. 61, 115–121 (1991).
Brosschot, J. F., Gerin, W. & Thayer, J. F. The perseverative cognition hypothesis: a review of worry, prolonged stress-related physiological activation, and health. J. Psychosom. Res. 60, 113–124 (2006).
Tallis, F. & Eysenck, M. W. Worry: mechanisms and modulating influences. Behav. Cogn. Psychother. 22, 37–56 (1994).
Ottaviani, C. et al. Physiological concomitants of perseverative cognition: a systematic review and meta-analysis. Psychol. Bull. 142, 231–259 (2016).
Espinosa, F., Martín-Romero, N. & Sanchez-Lopez, A. Repetitive negative thinking processes account for gender differences in depression and anxiety during adolescence. Int. J. Cogn. Ther. 15, 115–133 (2022).
O’Connor, D. B. et al. Effects of COVID-19-related worry and rumination on mental health and loneliness during the pandemic: longitudinal analyses of adults in the UK COVID-19 mental health & wellbeing study. J. Ment. Health 32, 1122–1133 (2022).
Smith, J. M. & Alloy, L. B. A roadmap to rumination: a review of the definition, assessment and conceptualization of this multifaceted construct. Clin. Psychol. Rev. 29, 116–128 (2009).
Luttenbacher, I., Breukel, J. S. & Adamson, M. M. The mediating role of rumination in the relationship between loneliness and depression in university students during the COVID-19 pandemic. COVID 1, 447–457 (2021).
Vanhalst, J., Luyckx, K., Raes, F. & Goossens, L. Loneliness and depressive symptoms: the mediating and moderating role of uncontrollable ruminative thoughts. J. Psychol. 146, 259–276 (2012).
Zawadzki, M. J., Graham, J. E. & Gerin, W. Rumination and anxiety mediate the effect of loneliness on depressed mood and sleep quality in college students. Health Psychol. 32, 212–222 (2013).
Park, S.-C. et al. How many different symptom combinations fulfil the diagnostic criteria for major depressive disorder? Results from the CRESCEND study. Nord. J. Psychiatry 71, 217–222 (2017).
Park, S.-C. & Kim, Y.-K. in Major Depressive Disorder: Rethinking and Understanding Recent Discoveries (ed. Kim, Y.-K.) 103–116 (Springer, 2021).
Fried, E. I. The 52 symptoms of major depression: lack of content overlap among seven common depression scales. J. Affect. Disord. 208, 191–197 (2017).
Fried, E. I. & Nesse, R. M. Depression sum-scores don’t add up: why analyzing specific depression symptoms is essential. BMC Med. 13, 72 (2015).
Borsboom, D. Psychometric perspectives on diagnostic systems. J. Clin. Psychol. 64, 1089–1108 (2008).
Bernstein, E. E., Heeren, A. & McNally, R. J. Reexamining trait rumination as a system of repetitive negative thoughts: a network analysis. J. Behav. Ther. Exp. Psychiatry 63, 21–27 (2019).
Everaert, J., Benisty, H., Gadassi Polack, R., Joormann, J. & Mishne, G. Which features of repetitive negative thinking and positive reappraisal predict depression? An in-depth investigation using artificial neural networks with feature selection. J. Psychopathol. Clin. Sci. 131, 754–768 (2022).
Weiss, R. Loneliness: The Experience of Emotional and Social Isolation (MIT Press, 1975).
van Tilburg, T. G. Social, emotional and existential loneliness: a test of the multidimensional concept. Gerontologist 61, e335–e344 (2020).
Hawkley, L. C., Browne, M. W. & Cacioppo, J. T. How can I connect with thee?: let me count the ways. Psychol. Sci. 16, 798–804 (2005).
Anyan, F. & Hjemdal, O. Loneliness in social relationships: mapping the nomological network of loneliness with key conceptual domains and theoretical constructs. J. Soc. Pers. Relat. 39, 132–154 (2022).
Piccinelli, M. & Wilkinson, G. Gender differences in depression: critical review. Br. J. Psychiatry 177, 486–492 (2000).
Maes, M., Qualter, P., Vanhalst, J., Van den Noortgate, W. & Goossens, L. Gender differences in loneliness across the lifespan: a meta-analysis. Eur. J. Personality 33, 642–654 (2019).
Nolen-Hoeksema, S. in Depressive Rumination (ed. Papageorgiou, C. & Wells, A.) 104–124 (Wiley, 2004).
Jones, P. J., Ma, R. & McNally, R. J. Bridge centrality: a network approach to understanding comorbidity. Multivar. Behav. Res. 56, 353–367 (2021).
Chu, S. A., Tadayonnejad, R., Corlier, J., Wilson, A. C. & Leuchter, A. F. Rumination: relationships with repetitive transcranial magnetic stimulation treatment of major depressive disorder. Brain Stimul. 14, 1693 (2021).
Maes, M., Qualter, P., Lodder, G. M. A. & Mund, M. How (not) to measure loneliness: a review of the eight most commonly used scales. Int. J. Environ. Res. Public Health 19, 10816 (2022).
Yeung, P., Wong, L., Chan, C., Leung, J. L. & Yung, C. A validation study of the Hong Kong version of Montreal Cognitive Assessment (HK-MoCA) in Chinese older adults in Hong Kong. Hong Kong Med. J. 20, 504–510 (2014).
Russell, D. W. UCLA Loneliness Scale (Version 3): reliability, validity and factor structure. J. Pers. Assess. 66, 20–40 (1996).
Luo, Q. & Shao, R. The positive and negative emotion functions related to loneliness: a systematic review of behavioural and neuroimaging studies. Psychoradiology 3, kkad029 (2023).
Lu, M., Wang, R., Lin, H., Pang, F. & Chen, X. Perceived social support and life satisfaction of Chinese parents of children with autism spectrum disorder: loneliness as a mediator and moderator. Res. Autism Spectr. Disord. 87, 101829 (2021).
Ren, L. et al. The association between loneliness and depression among Chinese college students: affinity for aloneness and gender as moderators. Eur. J. Dev. Psychol. 18, 382–395 (2021).
Zhu, Y., Liu, J., Qu, B. & Yi, Z. Quality of life, loneliness and health-related characteristics among older people in Liaoning province, China: a cross-sectional study. BMJ Open 8, e021822 (2018).
Wang, X. D., Wang, X. L. & Ma, H. Rating scales for mental health. Chin. Mental Health 12, 413–434 (1999).
Lin, C.-Y. et al. Psychometric evaluation of three versions of the UCLA Loneliness Scale (full, eight-item and three-item versions) among sexual minority men in Taiwan. Int. J. Environ. Res. Public Health 19, 8095 (2022).
Alsubheen, S. A., Oliveira, A., Habash, R., Goldstein, R. & Brooks, D. Systematic review of psychometric properties and cross-cultural adaptation of the University of California and Los Angeles loneliness scale in adults. Curr. Psychol. 42, 11819–11833 (2023).
Hackett, R. A., Poole, L., Hunt, E., Panagi, L. & Steptoe, A. Loneliness and biological responses to acute stress in people with Type 2 diabetes. Psychophysiology 56, e13341 (2019).
Gillespie, S. M., Jones, A., Uzieblo, K., Garofalo, C. & Robinson, E. Coping using sex during the coronavirus disease 2019 (COVID-19) outbreak in the United Kingdom. J. Sex. Med. 18, 50–62 (2021).
Treynor, W., Gonzalez, R. & Nolen-Hoeksema, S. Rumination reconsidered: a psychometric analysis. Cogn. Ther. Res. 27, 247–259 (2003).
Nagy, L. M., Shanahan, M. L. & Seaford, S. P. Nonsuicidal self‐injury and rumination: a meta‐analysis. J. Clin. Psychol. 79, 7–27 (2023).
Stade, E. C. & Ruscio, A. M. A meta-analysis of the relationship between worry and rumination. Clin. Psychol. Sci. 11, 552–573 (2022).
Stelmach-Lask, L., Glebov-Russinov, I. & Henik, A. What is high rumination? Acta Psychol. 248, 104331 (2024).
Liang, L. & Lee, Y.-H. Factor structure of the ruminative response scale and measurement invariance across gender and age among Chinese adolescents. Adv. Appl. Sociol. 9, 193–207 (2019).
Liu, D. et al. Rumination and depression in Chinese adolescents with mood disorders: the mediating role of resilience. J. Clin. Psychiatry 84, 48097 (2023).
Han, X. & Yang, H. F. Chinese version of Nolen-Hoeksema Ruminative Responses Scale (RRS) used in 912 college students: reliability and validity. Chin. J. Clin. Psychol. 17, 549–551 (2009).
Spitzer, R. L., Kroenke, K. & Williams, J. B. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. JAMA 282, 1737–1744 (1999).
Kroenke, K., Spitzer, R. L. & Williams, J. B. W. The PHQ-9. J. Gen. Intern. Med. 16, 606–613 (2001).
Costantini, L. et al. Screening for depression in primary care with Patient Health Questionnaire-9 (PHQ-9): a systematic review. J. Affect. Disord. 279, 473–483 (2021).
Luo, W., Zhong, B.-L. & Chiu, H. F.-K. Prevalence of depressive symptoms among Chinese university students amid the COVID-19 pandemic: a systematic review and meta-analysis. Epidemiol. Psychiatric Sci. 30, e31 (2021).
Yu, X., Tam, W. W. S., Wong, P. T. K., Lam, T. H. & Stewart, S. M. The Patient Health Questionnaire-9 for measuring depressive symptoms among the general population in Hong Kong. Compr. Psychiatry 53, 95–102 (2012).
Levis, B., Benedetti, A. & Thombs, B. D. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ 365, l1476 (2019).
Borsboom, D. & Cramer, A. O. J. Network analysis: an integrative approach to the structure of psychopathology. Annu. Rev. Clin. Psychol. 9, 91–121 (2013).
Borsboom, D. A network theory of mental disorders. World Psychiatry 16, 5–13 (2017).
R Core Team. R: a language and environment for statistical computing version 4.1.3 (R Foundation for Statistical Computing, 2022).
Revelle, W. psych: procedures for psychological, psychometric and personality research. R package version 2.3.3. https://CRAN.R-project.org/package=psych (Northwestern Univ., 2023).
Rosseel, Y. lavaan: an R package for structural equation modeling. J. Stat. Softw. 48, 1–36 (2012).
Epskamp, S., Borsboom, D. & Fried, E. I. Estimating psychological networks and their accuracy: a tutorial paper. Behav. Res. 50, 195–212 (2018).
Epskamp, S., Cramer, A. O. J., Waldorp, L. J., Schmittmann, V. D. & Borsboom, D. qgraph: network visualizations of relationships in psychometric data. J. Stat. Softw. 48, 1–18 (2012).
Jones, P. networktools: tools for identifying important nodes in networks. R package version 1.5.0 https://CRAN.R-project.org/package=networktools (Harvard Univ., 2022).
Hauser, A. & Buehlmann, P. Characterization and greedy learning of interventional Markov equivalence classes of directed acyclic graphs. J. Mach. Learn. Res. 13, 2409–2464 (2012).
van Borkulo, C. D. et al. Comparing network structures on three aspects: a permutation test. Psychol. Methods. 28, 1273–1285 (2023).
Epskamp, S. & Fried, E. I. A tutorial on regularized partial correlation networks. Psychol. Methods 23, 617–634 (2018).
Bringmann, L. F. et al. What do centrality measures measure in psychological networks? J. Abnorm. Psychol. 128, 892–903 (2019).
Robinaugh, D. J., Millner, A. J. & McNally, R. J. Identifying highly influential nodes in the complicated grief network. J. Abnorm. Psychol. 125, 747–757 (2016).
Moffa, G. et al. Using directed acyclic graphs in epidemiological research in psychosis: an analysis of the role of bullying in psychosis. Schizophr. Bull. 43, 1273–1279 (2017).
Acknowledgements
The project was supported by the Hong Kong Research Grants Council General Research Fund (17600522 to T.M.C.L.). The funding body played no role in the original study or the preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
C.C.H.C. and T.M.C.L. conceived the research idea. N.M.L.W. and T.M.C.L. designed the study. N.M.L.W., R.Z. and J.W. collected the data. J.L. analyzed the data. All authors discussed the findings. J.L. produced the first draft of the manuscript. J.L., N.M.L.W., R.Z., J.W., R.S., C.C.H.C. and T.M.C.L. revised the manuscript. All authors approved the final version to be published and agreed to be accountable for the integrity and accuracy of all aspects of the work.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Mental Health thanks Juan Ramos-Cejudo and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Inclusion statement
The research included local researchers in Guangzhou, Fuzhou and Hong Kong where local community populations were recruited for the current study. Roles and responsibilities were discussed and agreed among all collaborators ahead of the research. The research has also been approved by the University of Hong Kong Human Research Ethics Committee.
Supplementary information
Supplementary Information
Supplementary Tables 1–3 and Figs. 1–13.
Source data
Source Data Fig. 1
Source data for Fig. 1.
Source Data Fig. 2
Source data for Fig. 2.
Source Data Fig. 3
Source data for Fig. 3.
Source Data Fig. 4
Source data for Fig. 4.
Source Data Fig. 5
Source data for Fig. 5.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Luo, J., Wong, N.M.L., Zhang, R. et al. A network analysis of rumination on loneliness and the relationship with depression. Nat. Mental Health 3, 46–57 (2025). https://doi.org/10.1038/s44220-024-00350-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s44220-024-00350-x
