
Abstract
Background
To characterize neurodevelopmental abnormalities in children up to 36 months of age with congenital Zika virus exposure.
Methods
From the U.S. Zika Pregnancy and Infant Registry, a national surveillance system to monitor pregnancies with laboratory evidence of Zika virus infection, pregnancy outcomes and presence of Zika associated birth defects (ZBD) were reported among infants with available information. Neurologic sequelae and developmental delay were reported among children with ≥1 follow-up exam after 14 days of age or with ≥1 visit with development reported, respectively.
Results
Among 2248 infants, 10.1% were born preterm, and 10.5% were small-for-gestational age. Overall, 122 (5.4%) had any ZBD; 91.8% of infants had brain abnormalities or microcephaly, 23.0% had eye abnormalities, and 14.8% had both. Of 1881 children ≥1 follow-up exam reported, neurologic sequelae were more common among children with ZBD (44.6%) vs. without ZBD (1.5%). Of children with ≥1 visit with development reported, 46.8% (51/109) of children with ZBD and 7.4% (129/1739) of children without ZBD had confirmed or possible developmental delay.
Conclusion
Understanding the prevalence of developmental delays and healthcare needs of children with congenital Zika virus exposure can inform health systems and planning to ensure services are available for affected families.
Impact
-
We characterize pregnancy and infant outcomes and describe neurodevelopmental abnormalities up to 36 months of age by presence of Zika associated birth defects (ZBD).
-
Neurologic sequelae and developmental delays were common among children with ZBD.
-
Children with ZBD had increased frequency of neurologic sequelae and developmental delay compared to children without ZBD.
-
Longitudinal follow-up of infants with Zika virus exposure in utero is important to characterize neurodevelopmental delay not apparent in early infancy, but logistically challenging in surveillance models.
Similar content being viewed by others


Introduction
Given the impact of Zika virus (ZIKV) infection on the developing fetal brain and eye, it is critical to examine neurodevelopment in infancy and early childhood as well as pregnancy outcomes associated with congenital Zika virus exposure (CZVE).1 Uncertainty remains regarding frequency and spectrum of long-term neurodevelopmental outcomes for these children. In 2016, the Centers for Disease Control and Prevention (CDC) and state, local, and territorial health departments established the U.S. Zika Pregnancy and Infant Registry (USZPIR) to monitor pregnancy, infant, and childhood outcomes among pregnancies with laboratory evidence of confirmed or possible Zika virus infection.2,3 A previous USZPIR report evaluated outcomes among 1450 children born in the U.S. territories and freely associated states, who were ≥1 year old, finding 6% had at least one Zika-associated birth defect (ZBD), 9% had at least one neurodevelopmental abnormality, and 1% had both.4 However, pregnancy outcomes and neurodevelopmental data from the U.S. states and D.C. have not yet been reported from the USZPIR. Few cohort studies have reported on the longer-term neurodevelopment of children with CZVE, with or without ZBD.5,6,7 Emerging evidence suggests that children with ZBD can exhibit neurodevelopmental delays not detected until after their first year of life.8,9 However, among children without ZBD, information about the longer-term neurodevelopmental effects of CZVE is limited.1,10
A study in Colombia examined 77 infants with laboratory evidence of maternal ZIKV during pregnancy but no clinical signs of congenital Zika syndrome and normal prenatal neuroimaging.11 This study, which reported on neurodevelopment as assessed by validated measures at around 6 and 13 months of age, showed neurodevelopmental scores falling further below the mean as the children aged. Other studies have reported that children with prenatal ZIKV exposure can have normal findings on neurodevelopmental assessments in the first year of life but exhibit neurodevelopmental delays in the second year of life.11 A concern for language delays has also been reported for children greater than12 months of age with a history of CZVE with and without ZBD.5,6,7,12 Given the progressive nature of early child neurodevelopment and the possibility for delays to emerge beyond the first year of life, longitudinal surveillance is necessary.
Using the data from the USZPIR, we sought to expand on prior reports from this cohort by providing an updated estimate of adverse pregnancy outcomes, including not previously reported findings for small-for-gestational age (SGA) and preterm birth (PTB), neurologic sequelae, and neurodevelopmental abnormalities among children up to 3 years of age.
Methods
Study population and inclusion
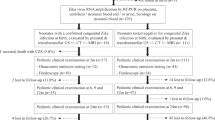
This report includes pregnancies reported to the USZPIR by December 31, 2021, that were completed in the U.S. states and D.C. from December 1, 2015 to March 31, 2018, with laboratory evidence of confirmed or possible maternal ZIKV and infants resulting from these pregnancies. Laboratory evidence of confirmed or possible recent ZIKV was defined as (1) recent ZIKV infection detected by a ZIKV RNA nucleic acid amplification test (NAAT, e.g., reverse transcription–polymerase chain reaction [RT-PCR]) on any maternal, placental, or fetal/infant specimen or (2) detection of recent ZIKV or recent unspecified flavivirus infection by serologic tests on a maternal or infant specimen (i.e., either positive or equivocal ZIKV immunoglobulin M [IgM] and ZIKV plaque reduction neutralization test [PRNT] titer ≥10, regardless of dengue virus PRNT value [if PRNT is conducted in the jurisdiction]; or negative ZIKV IgM, and positive or equivocal dengue virus IgM, and ZIKV PRNT titer ≥10, regardless of dengue virus PRNT titer). Additional details on methodology have been published previously.3,13
Surveillance follow-up and pregnancy, infant and neurodevelopmental outcomes
Data from prenatal care, birth hospitalization and delivery, and early childhood outcomes up to 36 months of age when available, were abstracted from medical records. Follow-up information included physical examinations, neurodevelopmental screenings, assessments and evaluations, neuroimaging, hearing screenings, audiological evaluations, and ophthalmology examinations.
Birth outcomes were classified as live birth, pregnancy loss <20 weeks gestation, and pregnancy loss ≥20 weeks gestation (stillbirth). Live births were further classified as preterm birth (<37 weeks), and SGA defined as birth weight <10th percentile for sex and gestational age according to INTERGROWTH-21st standards.14 Deaths were reported overall and categorized by age of child at death: neonatal (<28 days), post-neonatal (≥28 days to 1 year), and child (>1 year of age),15 after accounting for loss to follow up.
All mother-infant pairs with indication of any possible infant Zika-associated abnormality were reviewed by Zika subject matter experts in a first stage review. In a second stage, mother-infant pairs that included an infant with a ZBD or suspected neurodevelopmental abnormality were reviewed independently by two or more collaborating clinicians (i.e., pediatrician, obstetrician-gynecologist, clinical geneticist, pediatric neurologist) to confirm the abnormality. All discrepancies in classification between independent reviews were discussed and resolved among the full panel. The case definition for ZBDs has been previously described.3,16 Neurologic sequelae include hearing abnormalities, visual impairment, congenital contractures, seizures, body tone abnormalities, movement abnormalities, and swallowing abnormalities (Supplementary 1).
Data from children with at least one reported infant follow-up visit after 14 days of age were evaluated for notations in developmental domains (i.e., gross motor, fine motor, language, and social/emotional). The results of validated screening tools (e.g., Ages and Stages Questionnaire®, Parents’ Evaluation of Developmental Status) and non-validated/unknown screening tools (e.g., provider documentation, developmental screening data without name of screening tool used) were reviewed. Developmental data were evaluated among children with data reported by age intervals (0–5 months, 6–11 months, 12–17 months, 18–23 months, and 24- < 36 months of age). Developmental data are described by each interval among children with developmental data reported (e.g., number of children with a delay noted at the age interval/total number of children with developmental data reported at the age interval). Separately, a cumulative assessment of the presence of developmental delay (Supplemental 1) per child was classified as (1) confirmed (i.e., multiple notations of delay with mention of receipt of early intervention or rehabilitative therapy, supportive neuroimaging findings, or extreme premature birth (<28 weeks)), (2) possible (failing 1 or more ___domain on a validated screening tool at 1 or more time points, notations of abnormality in the gross motor ___domain but not on a validated screening tool, or notations of abnormality on 2 or more other developmental domains at 2 or more time points but not reported on a validated screening tool), or (3) no known developmental delay based on data reported.
Statistical analysis
Descriptive analyses were conducted for children with and without ZBD for the following maternal characteristics: age, symptoms, and trimester of possible Zika exposure (calculated using symptom onset, travel history, or positive laboratory results). Developmental abnormalities by ___domain were reported for each time point as an overall classification of possible or confirmed developmental delay. Analyses were stratified by presence of ZBD. An analysis was conducted on a subgroup of pregnancies with a positive NAAT-confirmed infection to assess whether findings were similar to those for the full cohort.
Data were uploaded into REDCap (version 11.1; Research Electronic Data Capture) and analyzed with SAS software (version 9.4; SAS Institute). This activity was reviewed by CDC and conducted consistent with applicable federal law and policy; this activity was deemed public health surveillance and outside the scope of research, thus exempt from Institutional Review Board (IRB) review.
Results
A total of 2,374 pregnancies meeting inclusion criteria were reported to CDC by December 31, 2021 (Supplementary 2). The median age of pregnant people was 27 years (interquartile range [IQR]: 22–32) (Table 1). Among pregnant people with known trimester of ZIKV exposure (n = 2106, 88.7%), 38.9% had possible Zika exposure detected in the first, 38.0% in the second, and 23.1% in the third trimester. One-quarter (n = 653) were reported as symptomatic; the most common symptoms reported were rash (80.6%), fever (43.6%), and joint pain (44.3%). Similar demographics, trimester of possible ZIKV exposure, and symptoms were reported among the subset with NAAT-confirmed infection (n = 423, 17.8%).
Among 2374 pregnancy outcomes, there were 2248 (94.7%) live births (36 multiples) and 126 pregnancy losses (76.2% <20 weeks and 23.8% ≥20 weeks) (Table 2). Overall, 10.1% (n = 226) of infants were born preterm (<37 weeks), including 14.8% (18/122) of infants with ZBD and 9.8% (208/2126) of infants without ZBD. Overall, 5.4% (122) live-born infants had a ZBD; 91.8% (n = 112) had brain abnormalities or microcephaly (47 cases with only microcephaly), 23.0% (n = 28) had eye abnormalities (10 cases with eye abnormalities only), and 14.8% (n = 18) had both brain and eye abnormalities. Ten percent (n = 225) of live-born infants were born SGA, including 53.3% of infants with ZBD (65/122) and 8.1% of infants without ZBD (172/2126). There were 20 infant deaths reported (11 with ZBD and 9 without ZBD). Of these, 60.0% (n = 12) of deaths occurred in the neonatal period (≤28 days), 30.0% (n = 6) in the postneonatal period (29–364 days), and 10.0% (n = 2) were ≥1 year of age.
Overall, 1881 (83.7%) children had at least one follow-up examination (>14 days of age) reported to USZPIR; of these, 91.6% had visits reported <6 months, 62.4% between 6–11 months, 60.1% between 12 and 17 months, 44.8% between 18–23 months, and 37.4% 24- < 36 months of age. Among children with ZBD and follow-up data (N = 112), 44.6% (n = 50) had neurologic sequelae. Among these 50, the most common sequelae were tone abnormalities (80.0%), and seizures (30.0%) (Fig. 1), with similar frequencies seen among children in the NAAT-confirmed population (data not shown). Twenty-six (1.5%, n = 26/1769) children without ZBD had neurologic sequelae, most frequently body tone abnormalities (34.6%) and hearing impairment (15.4%).

Children with developmental follow-up data and reported neurologic sequelaea, with and without Zika-associated birth defectsb (ZBD) (n = 76/1881 [50/112 children with ZBD and 26/1769 children without ZBD]), U.S. Zika Pregnancy and Infant Registry, U.S. States and DC. aY-axis shows percentage of children presenting with each abnormality among those with any neurologic sequelae. bThe case definition for ZBD has been previously described.3,16
Among the 1881 children with follow-up data reported, there were 1848 with at least one visit with information reported about development. The proportion of visits with reported information about development decreased with increasing age from 92.7% at <6 months to 38.9% at 24- < 36 months of age (Supplementary 2). Reported information on development decreased from 85.3 to 50.5% for children with ZBD and from 93.2% to 38.1% for children without ZBD. Among children with ZBD and information on development (n = 109), developmental ___domain abnormalities were >25% in children by 6 months of age (Fig. 2). The frequency of reported abnormalities noted across multiple domains was 9.7% by age <6 months and was highest at 41.7% by age 18–23 months for children with ZBD. Among children without ZBD (N = 1739), the frequency of reported developmental abnormalities was <20% across all domains and all age intervals. Language ___domain abnormalities were the most frequently reported by age >12 months and was 16.0% at the 24- < 36 months age interval.

Children with developmental follow-up data by age interval at assessmenta, with and without Zika-associated birth defectsb (ZBD) (N = 1848), U.S. Zika Pregnancy and Infant Registry, U.S. States and DC. aDenominator for each ___domain is all children with any notation of developmental data for each time point. bThe case definition for ZBDs has been previously described.3,16
Documentation of a validated developmental screening tool or developmental assessment ranged from 4.9% (n = 2/41) for children 6–11 months to 45.5% (n = 25/55) for children 24- < 36 months with ZBD and 5.2–33.5% (n = 57/1101 to 222/663, respectively) for the same timepoints for children without ZBD. A secondary analysis comparing data from validated screening tool and non-validated/unknown screening tools did not demonstrate any meaningful differences by developmental ___domain.
Among the 109 children with ZBD and developmental follow up, 51 (46.8%) had confirmed or possible developmental delay (42 [38.5%] confirmed and a further 9 [8.3%] possible). Gross and fine motor delays were most frequently reported among children with ZBD and confirmed developmental delay; more than one-third had delays noted across multiple domains (Fig. 3). Among these 109, 38 had structural brain abnormalities and of those 28 (73.8%) had confirmed or possible delay. Among children without ZBD and with developmental follow up (n = 1739), confirmed or possible developmental delay was noted among 7.4% (n = 129) (28 [1.6%] confirmed and 101 [5.8%] possible).

Children with developmental follow-up data who are classified as having confirmeda or possibleb developmental delay by ___domain, with and without Zika-associated birth defectsc (ZBD) (N = 1848), U.S. Zika Pregnancy and Infant Registry, U.S. States and DC. aConfirmed developmental delay: submitted specialist assessment, receipt of therapy, or multiple notations of delay with supportive neuroimaging findings. bPossible developmental delay: failing ≥1 ___domain on a validated screener at ≥1 time point, or ≥2 domains noted as abnormal at ≥2 time points but not reported as a validated screener. cThe case definition for ZBD has been previously described.3,16
Discussion
Children and families affected by the 2016–2017 ZIKV outbreaks in the Americas continue to experience the longstanding impacts of this virus, and we continue to learn about the spectrum of long-term effects of CZVE. This analysis provides insights regarding the neurodevelopmental trajectory for children up to 3 years of age. Based on the data that could be obtained through 3 years of age, approximately 1 out of 20 (5%) children with CZVE had ZBD and estimates for neurologic sequelae and neurodevelopmental abnormalities among children with CZVE varied by ZBD status. As expected, we observed a higher frequency of neurologic sequelae and developmental abnormalities among children with ZBD when compared with children without ZBD. Although the most severe outcomes of CZVE are apparent at birth, some neurodevelopmental sequelae manifested over time, requiring longitudinal surveillance to detect them. Close neurodevelopmental follow-up is recommended for all infants born to a person with ZIKV in pregnancy.17 Despite this recommendation, records available for about 20% of all children in USZPIR lacked reported developmental information and reported developmental information was often limited, and it is unclear whether these children received recommended follow-up and care.
Estimates of adverse pregnancy outcomes associated with CZVE have been limited by small sample size in individual cohorts and differential testing practices. A total of 30 stillborn infants were reported to USZPIR for an estimated rate of 1 stillbirth per 74 live births and stillbirths, higher than the national baseline estimate of 1 stillbirth per 160 live births and stillbirths.18 A higher-than-expected frequency of stillbirths was also reported within other cohorts of ZIKV in pregnancy.19 However, these data should be interpreted with caution given the differential Zika testing among people who had a stillbirth (e.g., higher likelihood of testing among those with a history of travel to Zika-affected areas or presence of Zika-associated abnormalities). Although early pregnancy losses were reported to the USZPIR, these are very likely to be underestimates given the numerous challenges with ascertaining early pregnancy losses through surveillance. The frequency of preterm birth reported to USZPIR (9.9%) was not greater than what is seen in the general U.S. population.20 Frequency of infants born SGA in this cohort (10.0%) was similar to national baseline estimates for 2015–2018 (9.63–10.02%),21,22,23,24 though was higher among infants with ZBD (50.8%, n = 62/122).25 The most frequent neurologic sequelae included tone abnormalities, seizures, and swallowing abnormalities. These findings are consistent with earlier reports from the USZPIR and existing literature describing other surveillance cohorts.9,26
Developmental delays were common among children with ZBD in this cohort. Structural brain malformation and injury from CZVE can affect all areas of development. Reports have described an association with the degree of structural brain abnormalities on neuroimaging with the severity of neurodevelopmental sequelae in children with possible ZIKV exposure.27 Thus, our finding of multi-___domain developmental delays among children with ZBD is expected. Children with ZBD and neurodevelopmental sequelae require access to a broad range of specialized services and have high healthcare expenditures (median total expenditure per infant with defects of $30,544 for the first year), particularly for public insurance programs in the U.S.28 Understanding the prevalence of developmental delays and healthcare needs among children with CZVE (both those with and without ZBD) can inform health systems and planning to ensure there are services available for affected families.
In our surveillance cohort, we did not observe an increased frequency of developmental delays among children without ZBD beyond what would be expected in the baseline population up to 3 years of age; however, the lack of an effect should be interpreted with caution given the observational nature of the report and reliance on documentation of development in the medical record. Language delays were the most common delay, mirroring the pattern in the general population.29 Similar findings were described among a large surveillance cohort of children with CZVE in Colombia.9 However, ZIKV clearly demonstrates neurotropism, and there is concern that CZVE may lead to long term neurodevelopmental abnormalities in children without ZBD. This has been demonstrated in several other published surveillance and research cohorts in the U.S. and internationally.8,11 Differences in findings may be due to inconsistencies in methodology among these cohorts. Surveillance for developmental delays is fraught with challenges, including differences in developmental screening and assessment practices, differences in case definitions and classification of developmental delays, inconsistent and incomplete documentation in the medical record, and loss to follow-up after infancy. Although prospective cohort studies with rigorous and standardized neurologic and developmental assessments are necessary to fully characterize developmental outcomes, they are logistically challenging and costly to implement.
Timing of diagnoses of developmental delays varied by type of delay. Within our cohort, most gross motor delays were detected by 6–11 months of age, whereas language delays continued to increase in frequency over time up to 2 years of age, which is unsurprising given the timing of development of language skills.30 This pattern of detection of language delays with increasing child age was similar among those with or without ZBD. It is important for surveillance systems following children congenitally exposed to the ZIKV to assess developmental outcomes longitudinally and over a protracted period of child development to identify developmental differences that may only emerge at later stages of child development, including intellectual disorders and learning disabilities, as well as behavioral and mental health conditions.
Limitations
Our findings should be considered in the context of several limitations. First, pregnancy losses are likely under-ascertained limiting our ability to understand any association with pregnancy loss. Second, maternal laboratory evidence of confirmed or possible ZIKV during pregnancy was based on presence of ZIKV RNA by a positive NAAT (e.g., RT-PCR), serologic evidence of a ZIKV, or serologic evidence of an unspecified flavivirus infection. Although this cohort was assembled during the height of the Zika virus outbreak in the Americas which reduces the likelihood of false positives due to IgM persistence, we conducted a sensitivity analysis among persons tested with positive NAAT for Zika. The subgroup analysis showed that demographic characteristics, pregnancy, and infant outcomes were similar to the full cohort among pregnant people with a positive NAAT. Third, this analysis uses data abstracted from clinical records of neurodevelopmental screenings and/or evaluations; although health departments attempted complete follow up of all pregnancy outcomes and children to obtain complete medical record information, many children were missing data points across various developmental age intervals, with 61.2% missing 24- < 36 months and only 17.1% of children having visits during all five time points. Additionally, there is potential for reporting bias; providers may be more likely to indicate developmental follow up information in children with pertinent findings. For these reasons, we assessed the developmental data at each age interval but were not able to perform statistical testing across timeframes given the loss to follow-up for each age group. Fourth, little information about the type of developmental screening or assessment was reported to USZPIR. There was wide variation in the quality of developmental data reported from the medical records. Although screenings may have been under ascertained in this surveillance system, multiple reports have described substandard use of validated screening tools in the general population at recommended timepoints of 9, 18, and 30 months.31 Inadequate screening may also result in an underreporting of the developmental delays associated with CZVE. A combination of both validated screening tool data and non-validated/unknown screening tool data was used; however, we did a secondary analysis by ZBD status and screening tools type with no clear differences between the groups. Additionally, we developed conservative criteria to define possible and confirmed developmental delay using multi-specialist clinician review of available abstracted data. Thus, we are only able to classify confirmed developmental delay, as few cases had documented validated developmental screening or evaluations and follow-up.
Conclusions
CZVE may manifest with a wide array of adverse pregnancy and infant outcomes including birth defects, neurologic sequelae, and developmental delay. The longitudinal mother-baby linked surveillance provided a unique ability to describe the long-term outcomes of children exposed to ZIKV in utero. These findings indicate a high prevalence of developmental delay among children with ZBD, emphasizing the importance of rapid and complete detection of congenital infections and ZBD as well as the need for serial developmental evaluations in these children. Longitudinal neurodevelopmental follow-up of all children with exposure to ZIKV in utero may improve the accuracy of neurodevelopmental delay estimations and improve planning efforts. Surveillance of these rare but significant adverse outcomes has informed comprehensive follow-up and evaluation as well as the provision of services necessary to help children with CZVE reach their full potential.
Data availability
These data are collected under relevant provisions of the Public Health Service Act and are protected at CDC by an Assurance of Confidentiality (Section 308(d) of the Public Health Service Act, 42 U.S.C. §242 m(d)) (https://www.cdc.gov/od/science/integrity/confidentiality/), which prohibits use or disclosure of any identifiable or potentially identifiable information collected under the Assurance for purposes other than those set out in the Assurance. Requests for access will be considered on a case-by-case basis, and inquiries should be directed to [email protected].
References
Wheeler, A. C. Development of infants with congenital Zika syndrome: What do we know and what can we expect? Pediatrics 141, S154–s60 (2018).
Reynolds, M. R. et al. Vital signs: Update on Zika virus-associated birth defects and evaluation of all U.S. infants with congenital Zika virus exposure—U.S. Zika pregnancy registry, 2016. MMWR Morb. Mortal. Wkly. Rep. 66, 366–73 (2017).
Honein, M. A. et al. Birth defects among fetuses and infants of US women with evidence of possible Zika virus infection during pregnancy. JAMA 317, 59–68 (2017).
Rice, M. E. et al. Vital signs: Zika-associated birth defects and neurodevelopmental abnormalities possibly associated with congenital Zika virus infection—U.S. territories and freely associated states, 2018. MMWR Morb. Mortal. Wkly. Rep. 67, 858–67 (2018).
Alves, L. V., Paredes, C. E., Silva, G. C., Mello, J. G. & Alves, J. G. Neurodevelopment of 24 children born in Brazil with congenital Zika syndrome in 2015: a case series study. BMJ Open 8, e021304 (2018).
Faical, A. V. et al. Neurodevelopmental delay in normocephalic children with in utero exposure to Zika virus. BMJ Paediatr. Open 3, e000486 (2019).
Lopes Moreira, M. E. et al. Neurodevelopment in infants exposed to Zika virus in utero. N. Engl. J. Med 379, 2377–2379 (2018).
Stringer, E. M. et al. Neurodevelopmental outcomes of children following in utero exposure to Zika in Nicaragua. Clin. Infect. Dis. 72, e146–e53 (2021).
Mercado-Reyes, M. et al. Pregnancy, birth, infant, and early childhood neurodevelopmental outcomes among a cohort of women with symptoms of Zika virus disease during pregnancy in three surveillance sites, project Vigilancia de Embarazadas con Zika (VEZ), Colombia, 2016–2018. Trop. Med. Infect. Dis. 6, 183 (2021).
Marbán-Castro, E. V. G. L. et al. Neurodevelopment in normocephalic children exposed to Zika virus in utero with no observable defects at birth: A systematic review with meta-analysis. Int J. Environ. Res Public Health 19, 7319 (2022).
Mulkey, S. B. et al. Neurodevelopmental abnormalities in children with in utero Zika virus exposure without congenital Zika syndrome. JAMA Pediatr. 174, 269–276 (2020).
Nielsen-Saines, K. et al. Delayed childhood neurodevelopment and neurosensory alterations in the second year of life in a prospective cohort of ZIKV-exposed children. Nat. Med. 25, 1213–1217 (2019).
Roth, N. M. et al. Zika-associated birth defects reported in pregnancies with laboratory evidence of confirmed or possible Zika virus infection—U.S. Zika pregnancy and infant registry, December 1, 2015-March 31, 2018. MMWR Morb. Mortal. Wkly. report. 71, 73–79 (2022).
Villar, J. et al. International Fetal and Newborn Growth Consortium for the 21st Century (INTERGROWTH-21st). International standards for newborn weight, length, and head circumference by gestational age and sex: the Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 384, 857–868 (2014).
Paixao, E. S. et al. Mortality from congenital Zika syndrome—nationwide cohort study in Brazil. N. Engl. J. Med 386, 757–67 (2022).
Olson, S. M. et al. Updated baseline prevalence of birth defects potentially related to Zika virus infection. Birth Defects Res. 111, 938–40 (2019).
Adebanjo, T. et al. Update: Interim guidance for the diagnosis, evaluation, and management of infants with possible congenital Zika virus infection—United States, October 2017. MMWR Morb. Mortal. Wkly. Rep. 66, 1089–99 (2017).
Hoyert, D. L. & Gregory, E. C. W. Cause-of-death data from the fetal death file, 2015–2017. Natl. Vital-. Stat. Rep. 69, 1–20 (2020).
Hoen, B. et al. Pregnancy outcomes after ZIKV infection in French territories in the Americas. N. Engl. J. Med 378, 985–94 (2018).
Martin J. A., Hamilton B. E., Osterman M. J. K. Births in the United States, 2020. NCHS Data Brief. 2021; 1–8.
Martin J. A., Hamilton B. E., Osterman M. J. K. Births in the United States, 2015. NCHS Data Brief. 2016; (no 258): 1–8.
Martin J. A., Hamilton B. E., Osterman M. J. K. Births in the United States, 2016. NCHS Data Brief. 2017; (no 287): 1–8.
Martin J. A., Hamilton B. E., Osterman M. J. K. Births in the United States, 2017. NCHS Data Brief. 2018; (no 318): 1–8.
Martin J. A., Hamilton B. E., Osterman M. J. K. Births in the United States, 2018. NCHS Data Brief. 2019; (no 346): 1–8.
Cooper, H. J. M. et al. Maternal Zika virus infection. Obstet. Gynecol. 134, 1197–204 (2019).
Satterfield-Nash, A. et al. Health and development at age 19–24 months of 19 children who were born with microcephaly and laboratory evidence of congenital Zika virus infection during the 2015 Zika virus outbreak—Brazil, 2017. MMWR Morb. Mortal. Wkly. Rep. 66, 1347–1351 (2017).
Daza, M. et al. Clinical and neurodevelopmental outcomes based on brain imaging studies in a Colombian cohort of children with probable antenatal Zika virus exposure. Birth Defects Res. 113, 1299–312 (2021).
Bergman, K., Forestieri, N. E., Di Bona, V. L., Grosse, S. D. & Moore, C. A. Medicaid healthcare expenditures for infants with birth defects potentially related to Zika virus infection in North Carolina, 2011–2016. Birth Defects Res. 114, 80–89 (2022).
Black L. I., Vahratian A. & Hoffman H. J. Communication disorders and use of intervention services among children aged 3–17 years: United States, 2012. NCHS Data Brief. 2015; (205): 1-8.
CDC. Learn the Signs. Act Early. 2021 [updated February 18, 2021]. Available from: https://www.cdc.gov/ncbddd/actearly/index.html.
Lipkin, P. H. et al. Trends in pediatricians’ developmental screening: Pediatrics 145, 2002–2016 (2020).
Funding
CDC provided funding support and technical assistance to all U.S. states, territories, and freely associated states that reported cases to the U.S. Zika Pregnancy and Infant Registry (USZPIR) through the Epidemiology and Laboratory Capacity for Prevention and Control of Emerging Infectious Diseases (ELC) cooperative agreement (https://www.cdc.gov/ncezid/dpei/epidemiology-laboratory-capacity.html) and to selected jurisdictions through the Zika Local Health Department Initiative (https://www.cdc.gov/pregnancy/zika/research/lhdi.html).
Author information
Authors and Affiliations
Contributions
V.N., K.W., D.C., N.R., M.R., C.C., V.T. conceptualized the study; K.W., V.T., took responsibility for the integrity of the study; M.R., A.A., E.L., A.E., S.S., S.S., N.L., M.A., P.L., S.K., S.B., L.L., K.S., M.G., R.B., S.K., U.H., A.L., M.C., T.W., J.T., N.M., N.A.B., C.S., J.F., S.H., A.N., L.I., S.A., E.P., E.S., D.R., M.M., B.S., E.L., L.D., D.C., P.R., E.F., M.M., K.S., A.C., V.L., S.B., L.O., L.C., L.R. coauthors conducted the data collection, data quality checks, are reported data to CDC; S.G.C., C.A.M., K.W., N.R., K.A., S.B., R.D., C.B. participated in the clinical review to determine whether pregnancies met surveillance case definition; V.N., D.C., N.R. conducted the data analysis and replication; V.N., D.C., K.W., N.R., S.B., V.T. participated in drafting the manuscript; all authors contributed to reviewing and revising the manuscript’s content and approving the final version of the paper.
Corresponding author
Ethics declarations
Competing interests
All authors have no conflicts of interest to disclose. The findings and conclusions in this article are those of the authors and do not necessarily represent the views or opinions of the California Department of Public Health or the California Health and Human Services Agency nor the official position of the Centers for Disease Control and Prevention.
Patient consent
Patient consent was not required as this activity was conducted as part of public health surveillance and deemed not research at CDC, thus exempt from IRB review.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations
Supplementary Information
Rights and permissions
About this article

Cite this article
Neelam, V., Woodworth, K.R., Chang, D.J. et al. Outcomes up to age 36 months after congenital Zika virus infection—U.S. states. Pediatr Res 95, 558–565 (2024). https://doi.org/10.1038/s41390-023-02787-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-023-02787-9
This article is cited by
-
Helping kids through early developmental screening
Pediatric Research (2025)
-
Continuing development of vaccines and monoclonal antibodies against Zika virus
npj Vaccines (2024)
-
Trends in prenatal and pediatric viral infections, and the impact of climate change
Pediatric Research (2024)
